
Abstract
Purpose:
To clarify the cut-off value of the Japanese Orthopaedic Association (JOA) score corresponding to rotator cuff tear outcome as evaluated by the Constant score.
Methods:
The subjects were 230 patients with rotator cuff tear. The Constant and JOA scores on the first examination in our hospital were evaluated. After investigation of the correlation between the Constant and JOA scores, the cut-off JOA score was calculated, corresponding to excellent, good and fair outcomes as evaluated by the Constant score.
Results:
The Constant and JOA scores on the first examination were 49.64 ± 12.84 and 72.52 ± 12.84, respectively, with a strong correlation (r = 0.87, p < 0.01). Receiver operating characteristic analysis revealed that the cut-off JOA score was 87.0 for excellent outcome (area under the curve, AUC: 0.93; sensitivity: 100%; specificity: 88.6%; p < 0.01), 84.0 for good outcome (AUC: 0.94; sensitivity: 100%; specificity: 83.4%; p < 0.01) and 78.0 for fair outcome (AUC: 0.88; sensitivity: 100%; specificity: 71.3%; p < 0.01).
Conclusions:
In patients with rotator cuff tear, good outcome as judged by a Constant score of ≥80 corresponds to a JOA score cut-off of 84.0. Judgement of the treatment outcomes and evaluation of the surgical method may be more accurate when using clear cut-off values for the scoring system employed, such as those determined in our study.
Introduction
Rotator cuff tears represent a painful shoulder condition frequently noted in middle-aged and elderly individuals. 1 The development of rotator cuff tear is considered to involve both external and internal factors, in the form of subacromial impingement 2 and tendon degeneration, 3 respectively. Conservative treatment 4 with medication 5 and physical therapy 6 represents the first therapeutic option, while surgical treatment 7 is indicated for treatment-resistant cases.
The Japanese Orthopaedic Association (JOA) score is typically used to evaluate the treatment outcome of shoulder conditions and consists of assessment of pain (30 points), function (overall function: 10 points; activities of daily living: 10 points), range of motion (active motion: 30 points), radiographic findings (5 points) and joint stability (15 points), amounting to a full score of 100 points (Table 1). While many minor changes have been applied, the JOA score is currently the most frequently used scoring system to evaluate patients with shoulder disease in Japan and is applied mostly for the purpose of comparing between pre- and post-treatment outcomes. 8 –16 A post-operative JOA score of 80 is regarded as clinically favourable, while a score of 50 or lower is regarded as clinically serious. However, no actual score representing satisfactory treatment outcomes has been established and no clear cut-off values have been set for the treatment outcomes assessed using this scoring system.
Assessing shoulder outcomes based on the JOA score.
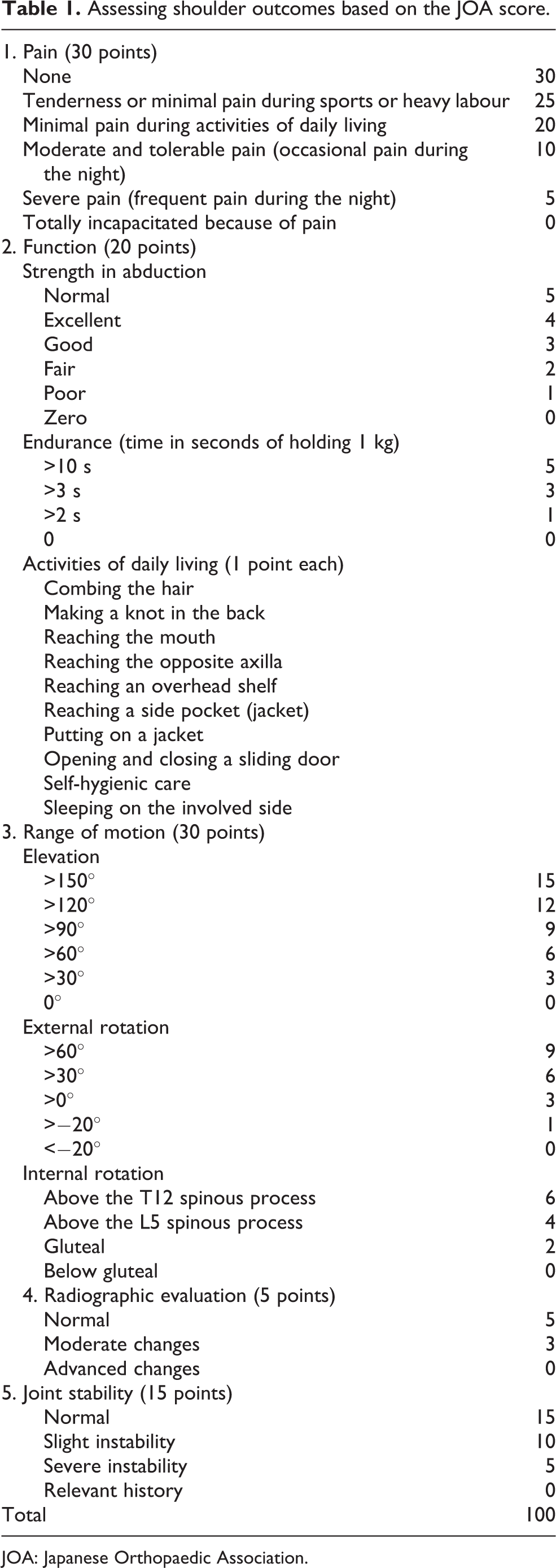
JOA: Japanese Orthopaedic Association.
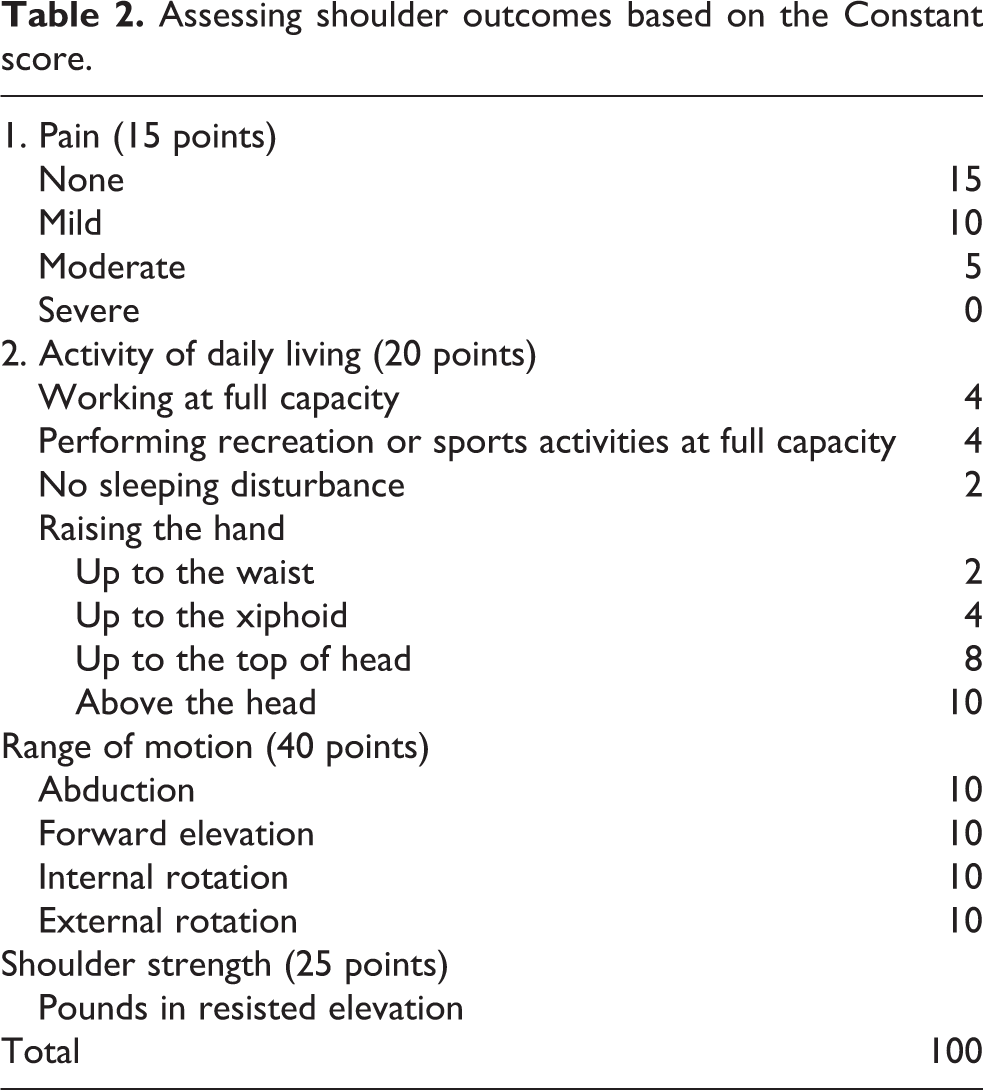
Among the 44 scoring systems for assessing shoulder outcomes, 17 the Constant score is one of the most frequently used worldwide. 17 –19 The Constant score comprised items related to pain (15 points), activities of daily living (20 points), range of motion (40 points) and muscle strength (25 points), amounting to a full score of 100 18,19 (Table 2); Constant scores of ≥90, ≥80, ≥70 and <70 are regarded as excellent, good, fair and poor, respectively. 2 –26 Both the JOA and Constant scores were used for shoulder evaluation in a number of recent studies on rotator cuff tear in Japan. 2 –32 Therefore, the objectives of the present study were to apply the Constant and JOA scores for evaluating shoulder outcomes in patients with rotator cuff tear, to investigate the correlation between the two scoring systems and to establish clear cut-offs for the JOA score indicative of various outcomes.
Assessing shoulder outcomes based on the Constant score.
Materials and methods
This study was performed after approval by the relevant ethics committees. All subjects provided written informed consent for participation.
Subjects
The study involved patients diagnosed with rotator cuff tear at our institutions between April 2013 and April 2015. The inclusion criteria were rotator cuff tear diagnosed by an orthopaedist, based on clinical and magnetic resonance imaging findings; and determination of the Constant and JOA scores on the first examination. The exclusion criteria were no determination of the JOA and Constant scores; fracture around the shoulder joint; bilateral rotator cuff tears; conditions of the joint such as progressive arthritis, osteoarthritis or infection. JOA score includes the question regarding the motion that needs the work by bilateral upper extremities (e.g., can the patients wear outer wear?). Therefore, we excluded the patients with bilateral rotator cuff tears.
Data collection
Functional evaluation of the shoulder joint was performed on the first examination and expressed in terms of the JOA and Constant scores. These data were collected by a physical therapist that was not involved in the present study. Demographic data and clinical information were also collected. Radiographic evaluation was performed by physicians and included an assessment of the sternoclavicular and acromioclavicular joints on plain radiographs.
JOA scoring method
Pain was evaluated using a questionnaire concerning the use of analgesics, frequency of night pain and pain intensity in daily life.
Regarding the overall functional state, abductor muscle strength and endurance of holding a 1 kg iron dumb-bell were evaluated via manual muscle testing, with the subject in the sitting position. Each item reflecting the functional state for activities of daily living was scored as 1, 0.5 and 0, respectively, if the activity could be performed smoothly, with difficulty, or not at all. The patients recalled their ability to perform various motions at home, and this information was logged using the questionnaire.
The range of motion was measured using a goniometer, with the subject in a sitting position. Elevation in the sagittal plane and external rotation were evaluated only on the affected side. On evaluation of internal rotation (making a knot in the back), the patient rotated the upper limb from the ipsilateral inferior side and touched the spinous process of the highest vertebral level that was reachable with the thumb.
Joint stability was evaluated not only in the glenohumeral joint, but also in the sternoclavicular and acromioclavicular joints. Instability, anxiety for dislocation (apprehension test) and past medical history of subluxation and dislocation were evaluated. The inferior, anterior and posterior regions were individually examined. The following conditions were evaluated as mild instability and anxiety for dislocation: inferior subluxation, caused by loading 5 kg (3 kg for women) in inferior instability; anxiety, caused by weight loading in anterior or posterior instability; and subluxation by ≤1/2 of the diaphyseal diameter. The following conditions were evaluated as serious instability or the state of subluxation: inferior subluxation, caused by loading only the upper limb in inferior instability; subluxation, caused by loading a weight in anterior instability that had previously led to subluxation, as revealed by the subject’s medical history; and subluxation by ≥1/2 of the diaphyseal diameter, caused by weight loading in posterior instability. Past medical history consisted of dislocation and subluxation that occurred within the 5 years before the examination.
Constant scoring method
Significant pain in daily life was assessed by means of a questionnaire, as was the functional (activity) state in activities of daily life, and the influence of the shoulder condition on work, recreation/sports and sleep. The ability to achieve a certain position of the limb in activities of daily life (positioning) was also assessed by means of the questionnaire, by asking the subjects to recall the maximum height they could raise their hand.
The range of motion was measured using a goniometer, with the subject in a sitting position. In the measurement of elevation, the subject raised the limb to the forehead, in the sagittal plane. In the measurement of external rotation, the palm was placed on the parietal region and the elbow joint was moved forward without moving the palm. The elbow joint was then moved backward to a site posterolateral to the head. The palm was then placed on the occipital region and the elbow joint was moved to a site anterior to the head and then to a site posterolateral to the head. In the measurement of internal rotation, the patient rotated the upper limb from an ipsilateral inferior site and touched the spinous process of the highest vertebral level that was reachable with the thumb.
In the muscle strength evaluation, the subject performed a 90° scapular plane elevation in a sitting position and maintained the position for 3 s. Muscle strength was measured using a handheld dynamometer (COMMANDER Power Track IITM; JTECH Co., Ltd., Midvale, Utah, USA), and each measurement was repeated 3 times. The mean strength was calculated in N and converted to pounds. When the patient could not perform a 90° scapular elevation, the evaluation was performed at the maximum abduction angle.
Statistical analysis
All statistical analyses were performed using JMP version 11 (SAS Institute Inc., Cary, North Carolina, USA). To investigate the correlation between the JOA and Constant scores, the correlation coefficient was calculated using the least squares method. Then, the subjects were divided into two groups, according to whether or not they met the Constant score of 90 points, which indicates excellent treatment outcome. The data for these groups were subjected to logistic regression analysis, followed by calculation of the relevant cut-off JOA score (i.e., the JOA score corresponding to excellent Constant score) via receiver operating characteristic (ROC) analysis. We are aware of small size in the excellent and good Constant score group, since patients were evaluated before treatment started. Logistic regression model was fitted using the unbalanced data. Although small sample in the excellent and good Constant score group affects the shape of the ROC curve, we thought that sensitivity and specificity estimation can be done. To this end, Youden’s index defined as (sensitivity + specificity−1) was used to obtain JOA cut-off values correspond to Constant score’s cut-off value. A similar procedure was applied to calculate the cut-off JOA values corresponding to the good (80 points) and fair (70 points) Constant scores. In all analyses, the significance level was set at 5%. The values were presented as the mean ± standard deviation.
Results
The study considered 422 patients diagnosed with rotator cuff tear between April 2013 and April 2015, of whom 230 patients (male, 116; female, 114) were included in the analysis after applying the inclusion and exclusion criteria. The mean age at the time of the first examination was 67.7 ± 10.2 years, and the mean duration of the illness was 13.7 ± 16.56 months. The tear size was assessed as partial thickness, small/medium and massive/extended in 83, 147 and 83 cases, respectively. Diabetes, hypertension and hyperlipidaemia were noted in 25, 49 and 26 patients, respectively.
The Constant and JOA scores on the first examination were 49.64 ± 12.84 (Pain: 6.61 ± 4.29; Activities of daily living: 12.41 ± 4.48; Strength: 5.57 ± 4.80; Movement: 25.05 ± 9.92) and 72.52 ± 12.84 (Pain: 17.11 ± 5.98; Function: 6.67 ± 2.85; Activities of daily living: 7.59 ± 2.64; Range Of Motion: 21.15 ± 5.73; X-ray: 5.00 ± 0.00; Instability: 15.00 ± 0.00), respectively. The correlation coefficient between the total scores provided by the two scoring systems was r = 0.87 (p < 0.01; Figure 1).

Correlation between the Constant score and the JOA score for assessing shoulder outcomes. JOA: Japanese Orthopaedic Association.
The cut-off JOA scores corresponding to the Constant scores indicative of excellent, good and fair outcomes were investigated. A total of 2, 8, 28 and 198 patients, respectively, had Constant scores of ≥90, ≥80, ≥70 and <70, and were thus included in the groups with excellent, good, fair and poor outcome. ROC curve analysis revealed that the cut-off JOA score was 87.0 for excellent outcome (area under the curve, AUC: 0.93; sensitivity: 100%; specificity: 88.6%; p < 0.01; Figure 2), 84.0 for good outcome (AUC: 0.94; sensitivity: 100%; specificity: 83.4%; p < 0.01; Figure 3) and 78.0 for fair outcome (AUC: 0.88; sensitivity: 100%; specificity: 71.3%; p < 0.01; Figure 4).

ROC curve of the JOA score corresponding to Constant scores indicating excellent outcomes. ROC: receiver operating characteristic; JOA: Japanese Orthopaedic Association.

ROC curve of the JOA score corresponding to Constant scores indicating good outcomes. ROC: receiver operating characteristic; JOA: Japanese Orthopaedic Association.

ROC curve of the JOA score corresponding to Constant scores indicating fair outcomes. ROC: receiver operating characteristic; JOA: Japanese Orthopaedic Association.
Discussion
The JOA score is commonly used in Japan to evaluate the outcome of rotator cuff tear, but there are no clear cut-offs to assess treatment outcomes more precisely, making it difficult to judge whether or not the outcome is favourable. Thus, we investigated the coefficient of correlation between the JOA score and the Constant score, which is most frequently used internationally. 20 We regarded the Constant score as the standard and observed a favourable correlation between the two scores (r = 0.87, p < 0.01). Logistic regression followed by ROC curve analysis revealed clear cut-offs of the JOA score at 87.0, 84.0 and 78.0, corresponding to excellent, good and fair outcome, respectively, as judged by the Constant score.
The Constant score is one of the shoulder joint assessment methods that are used internationally to evaluate the outcome of rotator cuff tear. 1 –19 A Constant score of ≥80 is regarded to indicate satisfactory outcome. 20 Fuchs et al. 33 reported the outcomes of rotator cuff tear treated via open repair with suture fixation; the mean pre-operative Constant score of patients with supraspinatus muscle tear was 54.3, which improved to 80.5 at 38 months post-operatively; however, in patients with subscapularis tear, the score improved from 51.8 to 72.9 and two patients with musculotendinous tear did not achieve a satisfactory score. Mukovozov et al. 34 performed a systematic review of rotator cuff tear patients treated with surgery in an early phase. The mean Constant score improved from 39.5 (pre-operatively) to 73.0 in the patients treated within 3 months of the tear event and from 53.5 to 81.0 in the patients treated at over 3 months after the tear event. These results suggest that satisfactory outcome is more likely to be achieved if surgical treatment is applied at least 3 months after the tear event.
Matsuura et al. 35 followed the long-term (≥15 years) treatment outcomes in Japanese patients with massive rotator cuff tear treated via open repair with suture fixation and noted that the pre-operative JOA score of 38.7 improved to 74.2 after 15 years. Hashiguchi et al. 15 employed arthroscopic fascial patch grafting to treat irreparable massive rotator cuff tear patients and noted that the mean pre-operative JOA score of 62.4 (range, 38–83) improved to 81.7 (range, 69–97) after surgery. When applying the JOA score cut-off value of 84 points (as determined in our study to indicate good outcome) to the reports of Matsuura et al. 35 and Hashiguchi et al., 15 the outcome would be considered unsatisfactory, despite the fact that statistically significant improvement from the pre-operative score was achieved. While our results do not suggest to doubt the usefulness of surgical treatment for rotator cuff tear, we believe that judgement of the treatment outcomes and evaluation of the surgical method may be more accurate, when using clear cut-off values for the scoring system employed, such as those determined in our study.
It is relevant to discuss the current acceptance of the term ‘satisfactory’ or ‘good’ in terms of the Constant and JOA scores. A Constant score of ≥80 is regarded to indicate good or excellent outcome. 20 Takagishi et al. 36 regarded a JOA score of 80 as clinically favourable. Ide et al. 8,11 regarded the JOA scores of >90, 81–90, 71–80 and <71 to indicate excellent, good, fair and poor outcome, respectively; they also classified the excellent/good Constant scores as satisfactory and fair/poor Constant scores as unsatisfactory. The cut-off value of 84, identified in our present study as the JOA score corresponding to good outcome (as evaluated via the Constant score), was close to these previously reported values, suggesting its reliability.
There are several limitations to our study. Firstly, this was a retrospective study and the number of patients included in the analysis was limited, not including the surgical cases. Secondly, the Constant score was used as the standard to calculate the cut-off JOA score for various outcomes; when using other scoring systems to evaluate outcomes, different cut-offs of the JOA score may be obtained; on the other hand, the advantage of using the Constant score is that a clear cut-off value (JOA score 84), with statistically high sensitivity and specificity, was determined for good outcome in rotator cuff tear.
Conclusion
In patients with rotator cuff tear, good outcome as judged by a Constant score of ≥80 corresponds to a JOA score cut-off of 84.0.
Footnotes
Acknowledgements
We thank Dr Tatsuyuki Kakuma for his statistical assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
This study was performed after approval by the Ethics Committees of Saiseikai Yahata General Hospital (approval no. 81) and Kurume University School of Medicine Graduate School (approval no. 15,179).
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.