
Abstract
Introduction
Distal clavicular resection (DCR) is a procedure used to alleviate acromioclavicular joint (ACJ) pain, often done alongside rotator cuff repair (RCR). This investigation explored the relationships between DCR and RCR, outcomes of DCR during RCR, and complication rates of DCR.
Methods
This retrospective study used electronic medical record data from the TriNetX database. Cohorts were subdivided based on the timeline of DCR in comparison to RCR, as well as comparing RCR with DCR against RCR without DCR.
Results
In total 46 534 patients underwent RCR with 14.8% (6898) of these patients also undergoing DCR. And 72.8% (5021) had DCR during RCR, and 10.7% (740) had DCR after RCR. Less than 5% (<10) of patients with preexisting ACJ pain required DCR 3 years postoperatively, and 0.002% (78) patients without ACJ pain developed ACJ pain within 3 years. Less that 20 patients underwent DCR within 3 years of being diagnosed with ACJ pain. Patients who had RCR with DCR were more likely to have chronic pain postoperatively (P < .0001).
Conclusion
Patients undergoing RCR do not require subsequent DCR. Performing DCR does not offer significant benefit when compared to performing isolated RCR without DCR in patients with preexisting ACJ pain, but increases risk for ACJ instability and chronic pain.
Introduction
Rotator cuff tears and associated shoulder pathologies are prevalent musculoskeletal disorders that significantly impact patients’ quality of life and functional capabilities. 1 Surgical repair of the rotator cuff is frequently employed to alleviate symptoms, restore shoulder functionality, and improve overall patient outcomes.2,3 Distal clavicular resection (DCR), often performed concomitantly with rotator cuff repair (RCR), has been utilized to address acromioclavicular joint (ACJ) pain and associated pathology.4,5 However, the indications, benefits, and potential risks of DCR during RCR remain topics of ongoing research and clinical investigation.6,7
The ACJ plays a critical role in shoulder biomechanics, and its dysfunction can lead to pain, impingement, and limited range of motion.4,5 The decision to perform DCR alongside RCR is based on the belief that addressing ACJ pathology concurrently with RCR may lead to better postoperative outcomes and overall patient satisfaction.7–10 Nevertheless, controversies persist regarding the necessity of DCR in all cases of RCR, and its potential association with complications following surgery.7,8,11,12 While some studies have been performed regarding the outcomes of DCR performed with RCR, few have evaluated clinical outcomes in conjunction with recurrence or necessity of subsequent repair, and fewer have evaluated these surgeries in the context of ACJ pathology.
In this study, we utilized TriNetX, a large multisite national database to analyze a large cohort of patients undergoing RCR. This study aims to address when most patients receive DCR with respect to RCR and whether patients with known ACJ pain benefit from DCR at the time of RCR. This study seeks to address 2 main questions. We sought to explore when most patients receive DCR with respect to RCR and if patients with known ACJ pain benefit from DCR at the time of RCR. Additionally, this study evaluates the development of ACJ pain following RCR and the risks of performing concomitant DCR and RCR versus RCR alone. The findings of this study may serve to refine surgical practices, enhance patient selection criteria, and improve the overall efficacy and safety of RCR as well as DCR.
Methods
Study Design and Data Collection
The TriNetX database is a health research network which provides access to longitudinal electronic medical records from 81 healthcare organizations and over 98 million patients. The TriNetX network was retrospectively queried on June 28, 2023 using cohorts developed with current procedural terminology (CPT) and International Classification of Disease 10th edition (ICD-10) codes. Only patient data collected over the past 10 years was considered in the study.
Cohort Selection
Patients in all cohorts underwent rotator cuff repair, which was identified by CPT codes (Table 1). Laterality was determined by ICD-10 codes (Table 2). DCR CPT codes 29 824 (arthroscopic DCR) and 23 120 (open DCR) were combined with RCR, with the temporal relationship either before, during, or after the procedure. Additionally, patients were grouped based on prevalence of ACJ pain before or after surgery, and if they received distal clavicular resection within 3 years of the diagnosis of ACJ pain.
Procedural Definitions.

Abbreviation: SLAP, superior labral anterior posterior.
Diagnostic Definitions.
Finally, outcomes were compared between patients who had undergone DCR concomitantly with RCR and patients who had solely undergone RCR, as well as patients who underwent RCR concomitantly with DCR as compared to patients undergoing DCR after initial RCR. Once cohorts were created, they were then propensity matched on age, race, body mass index (BMI), nicotine use, history of osteoarthritis, and history of diabetes.
Outcomes
Several postoperative outcomes were compared between the cohort that received DCR alongside RCR and the cohort that had solely received RCR. These outcomes were assessed at 1 month, 6 months, and 1 year postoperatively. The outcomes assessed include general surgical complications, injury to the rotator cuff, need for upper extremity repair, musculoskeletal, neurological, and circulatory postoperative complications, infection, acute pain, heterotopic ossification, ACJ instability, and chronic pain (Table 3).
Outcome Definitions.

Abbreviation: ACJ, acromioclavicular joint.
Statistical Analysis
In order to compare postoperative outcomes between patients who had received DCR with RCR and patients who had solely received RCR, both cohorts were propensity matched based on sex, age, nicotine dependence, BMI, and prior history of osteoarthritis in the same shoulder. Outcomes of the 2 cohorts were compared with odds ratios. A P value of <.05 was deemed significant between the cohorts.
About TriNetX
TriNetX is a “global health research network that optimizes clinical research and enables discoveries through the generation of real-world evidence,” and has been described well in other published literature 13 (TriNetX: Answers at the Speed of Thought, 2019. https://www.trinetx.com/.). The data encompasses various aspects such as demographics, diagnoses (coded using ICD-10), procedures (coded with ICD-10 PCS and CPT), medications, laboratory values, and genomic data. To achieve accurate analysis, the data is processed using parallel R and Python queries within the analytics platform. TriNetX functions as a federated network and has obtained a waiver from the Western Institutional Review Board. The data received by TriNetX consists solely of aggregated counts and statistical summaries of de-identified information.
Results
From January 2013 to June 2023, there were 46 534 patients who underwent RCR from over 45 healthcare organizations in the database. Regarding demographics, patients who underwent RCR were more likely to be individuals with a higher BMI and a history of osteoarthritis, with African American and Asian populations being less likely to undergo DCR with RCR (Table 4).
Demographics of RCR Compared to RCR and DCR (in Right Shoulder).

Abbreviations: BMI, body mass index; DCR, Distal clavicular resection; RCR, rotator cuff repair.
Bold text denotes significant results.
Data regarding temporality of DCR in the context of RCR can be found in Table 5. Of the 46 534 patients who underwent RCR, there were 6898 patients who have at some point undergone DCR. In total 1137 patients underwent DCR before their RCR, 740 patients underwent DCR after the initial RCR, and 5021 patients underwent DCR during their RCR procedure. Additionally, there were 318 diagnoses of isolated ACJ pain in patients who underwent RCR. Two hundred and forty patients were diagnosed with ACJ pain before their RCR procedure, and 72 of those patients underwent DCR at the time of their RCR procedure. Of those who did not get DCR at the time of RCR, <10 of those patients required future DCR over the next 3 years. Additionally, 82 patients were diagnosed with ACJ pain within 3 years of their RCR procedure, and <20 of these patients elected to undergo DCR within 3 years of undergoing RCR (Table 6).
Temporality of DCR.

Abbreviations: DCR, Distal clavicular resection; RCR, rotator cuff repair.
ACJ Pain in the Context of RCR.

Abbreviations: ACJ, acromioclavicular joint; DCR, Distal clavicular resection; N/A, not applicable; RCR, rotator cuff repair.
When comparing risk of postoperative complications between RCR and DCR as compared to RCR without DCR, we determined that there are few differences in risk for general postoperative surgical complications. These include musculoskeletal, neurological, or circulatory complications, risk of rotator cuff injury, risk of general perioperative complications, infection, or acute pain. There are no significant differences in complication rates in patients undergoing DCR during RCR as compared to patients who undergo DCR within 3 years of initial RCR (Table 7). We found that patients undergoing RCR and DCR concomitantly as compared to patients undergoing RCR alone had a slightly higher risk for chronic pain, primarily after 6 months and onwards (1.74% increase at 12 months, P < .0001). We also determined that there is a slightly higher risk for ACJ instability within a relatively short postoperative period of 6 months and onwards when comparing these same groups (0.16% increase at 12 months, P < .0001) (Table 8).
Postoperative Complications in Patients Receiving DCR During RCR versus DCR After RCR.
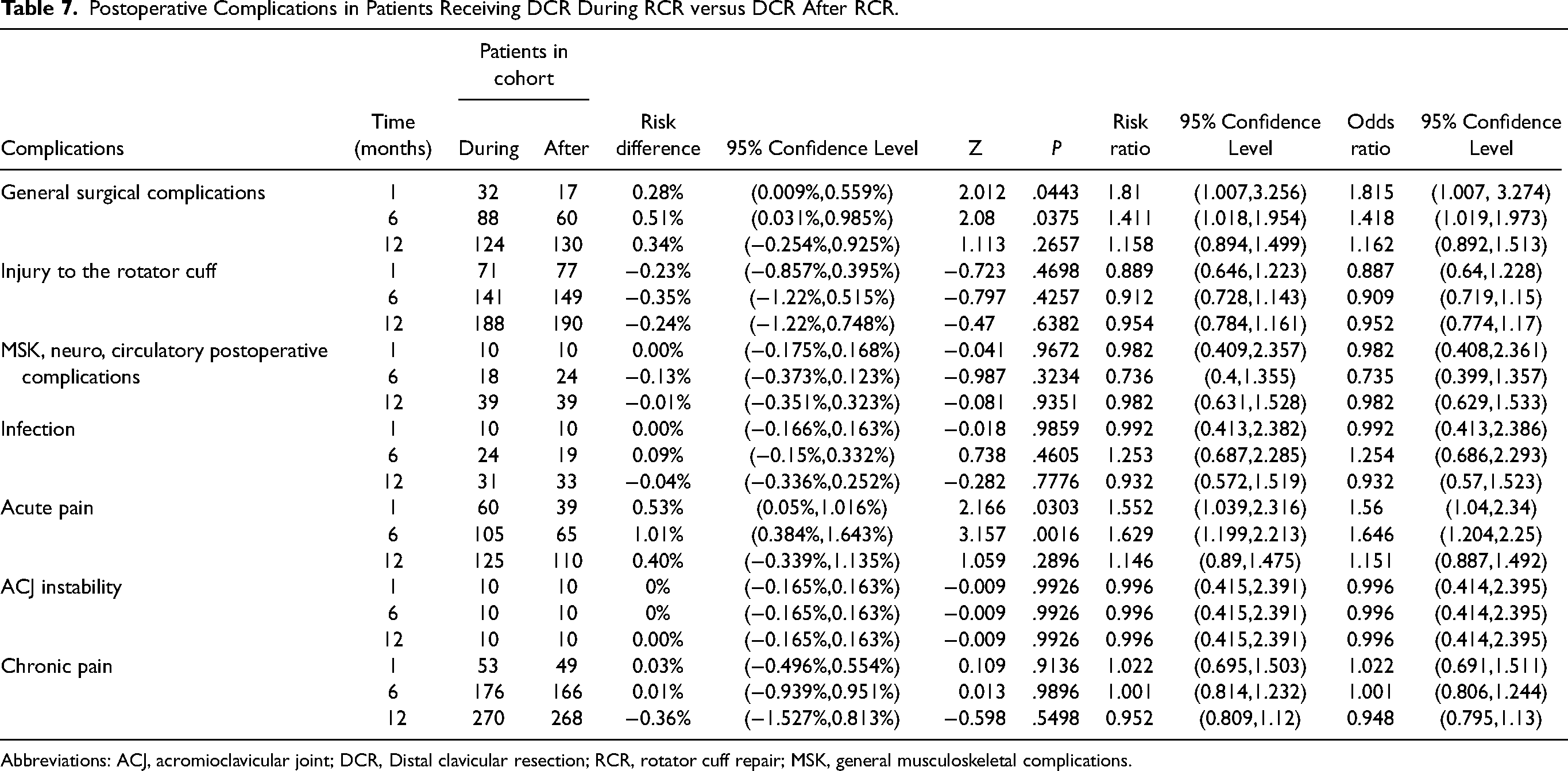
Abbreviations: ACJ, acromioclavicular joint; DCR, Distal clavicular resection; RCR, rotator cuff repair; MSK, general musculoskeletal complications.
Postoperative Complications in Patients Receiving RCR Without DCR versus RCR Concomitantly With DCR.

Abbreviations: ACJ, acromioclavicular joint; DCR, Distal clavicular resection; RCR, rotator cuff repair; MSK, general musculoskeletal complications.
Discussion
The purpose of this study was to identify general trends in use of DCR with respect to RCR as well as address whether patients with ACJ pain benefit from undergoing DCR and RCR concomitantly. We also sought to further characterize the relationship of ACJ pain to RCR and the complications of concomitant RCR and DCR versus RCR alone.
With respect to the general trends in use of DCR with respect to RCR, our results show that roughly a minority of patients (15% in our cohort) undergoing RCR have also undergone or will undergo DCR. Of those that do undergo DCR, the vast majority of these DCR procedures occur concomitantly with RCR. While our numbers are larger than some other studies, the overall temporality is similar to contemporary literature.7,14 DCR does not appear to benefit patients with ACJ pain, nor is it beneficial when used in a preventative manner. Of the 46 534 patients who received RCR, only 240 patients had a diagnosis of ACJ pain prior to surgery. Of the 168 patients who did not undergo DCR and RCR, <10 patients required DCR within 3 years postoperatively. Furthermore, only 82 patients or 0.17% of the total cohort went on to develop ACJ pain following RCR, and only 20 of these patients subsequently underwent DCR. Again, these findings corroborate newer literature showing no difference in postoperative reoperation, revision, ACJ injection, and complications. 15 Overall, DCR does not appear to have a preventative or therapeutic role for most patients. Of the 240 patients diagnosed with ACJ pain before RCR, 72 received a DCR at the time of their RCR, and if they did not, less than ten of the remaining patients underwent DCR within 3 years. In patients who did not undergo DCR during or before their RCR, the frequency of developing ACJ pain is very low, with <0.01% (n = 82) of patients receiving a diagnosis of ACJ pain within 3 years following RCR. Of these patients, even fewer eventually underwent DCR within 3 years. While correlating these differences in performed procedure to postoperative outcomes, the only difference observed between the RCR and DCR and the RCR group was the risk of chronic pain and ACJ instability. The patients who underwent DCR were more likely to have either chronic pain or ACJ instability. Specifically, patients undergoing RCR and DCR had a 0.16% greater chance of developing ACJ instability (P < .0001) 1 year postoperatively and a 1.74% greater chance of having later incidences of chronic pain (P < .0001) 1 year postoperatively. It could be extrapolated that the statistical risk would be even greater as time progresses. These results not only reinforce that DCR performed alongside RCR does not provide any measurable prophylactic advantage to reduce instances of ACJ instability, but also indicate that DCR may predispose patients toward worse outcomes.
These results may need to be interpreted with caution, as some significant limitations may be inherent in the study due to the format used. Use of TriNetX, while comprehensive, only includes data based on CPT codes and ICD-10 codes. When evaluating chronic pain, there is no ICD-10 code specific for chronic shoulder pain, so this specific result may be taken with caution. We attempted to create the best matches for ACJ pain, RCR, DCR, and complications for postoperative risk analysis, but this could not be completely comprehensive, as we did not have access to direct patient charts to evaluate patient data. For instance, when accounting for laterality, we attempted to include patients only with a diagnosis on the operative arm. However, that does not exclude patients with bilateral ACJ pain, or bilateral RCR, or other instances where patients may have been excluded or included unnecessarily. Additionally, we did not account for differences in outcomes for open versus arthroscopic procedures. This applies to all the statistical groups evaluated, so while there would not be any differences in the results, the implications of this study may not apply universally to DCR when considering open against arthroscopic procedures. We would recommend further research in this area to continue to evaluate the efficacy of open and arthroscopic procedures in this context. A further limitation of this study is due to the TriNetX database itself since it defaults to reporting a minimum value of 10, preventing analysis of single-digit values. As such, we cannot report exact values for some parameters, such as patients with ACJ pain undergoing DCR within 3 years of RCR. While this does not change the interpretation of the results, this does prevent complete accuracy of the reported values. Lastly, large database studies are not capable of evaluating causal relationships in the same manner as prospective studies. Due to this, none of the findings can be taken as causative, but are purely correlative.
Conclusion
This investigation found that patients who receive isolated RCR do not require subsequent DCR. Even in the setting of the above limitations, temporal data seems to indicate that DCR does not have any added benefit when performed to address diagnosed ACJ pain at the time of RCR, or to prevent development of ACJ pain following RCR. In fact, performing DCR at the same time as RCR may even predispose some patients to increased surgical complications and chronic ACJ pain. Such findings should be further studied in clinical trials for confirmation but are an important first step in highlighting an area for potential improvement.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.