
Abstract
Background:
Massive blood loss during posterior spinal fusion for adolescent idiopathic scoliosis remains a significant risk for patients. There is no consensus on the benefit of acute normovolemic hemodilution (ANH) or intraoperative cell salvage (ICS) in scoliosis surgery.
Methods:
Patients were randomized to one of two groups. Group A received ANH and ICS during operation, while group B received only ICS. Patients’ age, sex, height, weight, body blood volume, number of fusion level, Cobb angle, number of screws, duration of surgery, and skin incision length were recorded. Hemoglobin and hematocrit levels were obtained preoperatively and postoperatively (0 h and 24 h).
Results:
There were 22 patients in each group. There was no significant difference in total blood loss. The perioperative decrease in hemoglobin levels between preoperation and postoperation 24 h (group A 2.79 ± 1.15 and group B 2.76 ± 1.00) showed no significant difference (p = 0.93). Group A observed a larger decrease in hemoglobin levels at postoperative 0 h relative to preoperative level (2.57 ± 0.82 g/dl), followed by a smaller decrease within the next 24 h (0.22 ± 1.33 g/dl). Group B showed a continued drop in hemoglobin levels of similar magnitude at postoperation 0 h (1.60 ± 0.67 g/dl) and within the next 24 h (1.16 ± 0.78 g/dl). One patient from group B received 1 unit of allogenic blood transfusion (p = 0.33).
Conclusions:
The addition of ANH to ICS in posterior spinal fusion surgery for AIS resulted in a similar decrease in hemoglobin levels between preoperative values and at 24 h postoperatively.
Keywords
Introduction
Massive blood loss during posterior spinal fusion (PSF) for adolescent idiopathic scoliosis (AIS) remains a significant risk for patients. Excessive bleeding is a common perioperative complication with a prevalence of 0.85%. 1 Yoshihara et al. noted that the transfusion rate of allogenic blood was stable (over a 10 years period) with transfusion rate as high as 23.0%. 2 This is despite an advancement in the surgical technique for AIS. 3 –5
Recently, there is an increased interest in utilizing autologous blood in scoliosis surgery. Two popular techniques as part of the armamentarium of perioperative blood conservation strategy are acute normovolemic hemodilution (ANH) and intraoperative cell salvage (ICS). ANH and ICS have been reported to reduce the incidence of allogenic blood transfusion. 6,7 Most studies were carried out in cardiac, vascular, and arthroplasty surgery. ATIS trial (autologous versus allogenic transfusion in aortic surgery) found that ANH with ICS reduced allogenic blood transfusion compared with control group. 8 Another study by McGill et al. found that ANH and ICS during elective coronary artery bypass grafting surgery have no additional benefit in terms of allogenic transfusion incidence. 9
Only very few studies were performed to assess the benefit of ANH or ICS in scoliosis surgery, and the results were conflicting. 10 –14 In this prospective randomized study, we compared the perioperative hemoglobin levels in patients who had both the ANH and ICS technique against those who only had ICS technique during PSF surgery.
Materials and methods
After receiving approval from the Institutional Review Board, we performed this randomized trial between February 2014 and August 2014. The protocol for this study was registered at ClinicalTrials.gov (identification number NCT02112409).
Patients aged 10–25 years old who were American Society of Anesthesiologists physical status I and II, with preoperative hemoglobin level >10 g/dl and preoperative platelet level >150,000/l, and scheduled for elective single-stage PSF were recruited. Exclusion criteria were patient’s refusal of homologous blood, hematological disorder, patients who received anticoagulants and antiplatelets perioperatively, and severe restrictive pulmonary disease.
Patients were randomly assigned to one of two groups, that is, A or B, using concealed allocation method. A computerized random number generator was used to formulate an allocation schedule. Group A received both ANH and ICS during operation, and group B received only ICS as sole autologous transfusion strategy. Allocation was revealed prior to the surgery from an opaque envelope containing the allocation (labeled as group A or B).
Anesthetic protocol and ANH technique
For group A, 500 ml of whole blood was removed via the radial artery after induction of anesthesia, and was collected into two separate JMS blood bag system (JMS Singapore PTE LTD, 440, Ang Mo Kio Industrial Park 1, Singapore 569620) containing anticoagulant citrate-dextrose (ACD) and stored at ambient temperature. Simultaneously, equal volume of 500 ml of Voluven® (Fresenius Kabi, Halden, Norway) (6% hydroxyethyl starch 130/0.4 in 0.9% sodium chloride) was infused to the patient via peripheral vein to maintain isovolemia. ICS was used in both groups during surgery using the Cell Saver® 5+ autologous blood recovery system (Haemonetics Corporation, Braintree, MA, USA) which was operated by a trained perfusionist.
Induction of anesthesia was carried out with intravenous (IV) propofol 2–4 mg/kg, single dose IV rocuronium 1.0 mg/kg, and target controlled infusion (TCI) of remifentanil 5 ng/ml to facilitate endotracheal intubation. Subsequently, balanced anesthesia using volatile anesthetic desflurane with minimum alveolar concentration of 0.6–0.8, TCI remifentanil 2–7 ng/ml, and IV rocuronium 5 mg intermittent bolus were used to maintain anesthesia. Bispectral index monitor (BIS) was used to monitor depth of anesthesia with a target BIS of 40–60. IV tranexemic acid 20 mg/kg was administered to both groups of patients. Ringer’s lactate solution was used throughout the operation as maintenance fluid therapy and as replacement for intraoperative insensible fluid losses in accordance with Holliday–Segar formula. Additional 5 ml/kg bolus of crystalloid or colloid would be given when mean arterial pressure decreases below 60 mmHg, heart rate increases by 20% from baseline, and urine output of less than 0.5 ml/kg/h.
Surgical protocol
The surgical protocols for all patients were similar. Alternate level pedicle screw instrumentation was performed for all patients. Two pairs of consecutive base screws were inserted as distal anchors and two pairs of consecutive screws were also placed as proximal anchors. In between, alternate level paired pedicle screws were inserted. Posterior release consisted of facetectomy with no Ponte osteotomies performed for this cohort of patients. Additional hemostatic strategy such as usage of gelfoam, surgicel, or bone wax was at the discretion of the attending surgeon. A subfascial drain was inserted prior to completion of the surgery. The two senior surgeons, KMK and CCYW, operated on all the cases. Postoperative drainage was managed using the following protocol. Immediately after completion of the operation, the suction drain was clamped. At 18–24 h postoperatively, the drain would then be removed after draining a maximum of 200 ml of blood. The postoperative drainage was not included into the estimation of the blood loss in this study.
Baseline characteristics of patients such as age, sex, height, weight, body blood volume (estimated using Nadler’s formula), and baseline operative details such as number of spine level involved, Cobb angle, screws used, duration of surgery, and skin incision length were recorded. The estimated total blood loss (EBL) was estimated from the cell salvage system and the difference between the weights of dry and blood-soaked sponges. Blood loss from the floor, surgical gowns, and drapes were not included. EBL by the cell salvage system is calculated using the following formula

Our perfusionist calculated the total volume of ACD used and total unfiltered blood (difference between weights of used versus dry reservoir). The total irrigation fluid was measured by the nurses prior to use in the operative field.
Collected autologous blood would be reinfused to patient at completion of surgery. However, it would be given to patient during surgery if there were 30% or more blood volume lost. Allogenic blood would be administered when the intraoperative hemoglobin concentration fell below 8 g/dl despite completion of autologous blood and adequate fluid resuscitation, persistent hypotension, or tachycardia >20% from baseline. Hemoglobin and hematocrit levels were obtained preoperatively and postoperatively (at 0 h and 24 h). Patients with postoperative hemoglobin value of less than 8 g/dl will receive one unit of allogenic packed red cell transfusion.
Statistical analysis
We used PS (Power and Sample Size Calculation Software) version 3.0 to determine our sample size. Based on a pilot sample of 10 subjects (five subjects per each arm), the response within each arm was normally distributed with a standard deviation of 0.70. The true difference in means between the two arms was 0.68. We set the type I error probability as 0.05 and power of 0.8. Hence, the required sample size was 18 subjects per each group, that is, total of 36 subjects to fulfill the required sample size. To add on a 20% dropout rate, the final calculated sample size was 44 subjects, that is, 22 subjects/arm.
All data were analyzed using SPSS software version 22 (Chicago, Illinois, USA). Variables with normal distribution were expressed as mean ± standard deviation and compared with the parametric unpaired two-tailed t-test. Data with skewed distribution were compared with the Mann–Whitney U test and expressed as median (interquartile range). Categorical data were presented as frequencies (percentages) and compared with the χ2 test. Level of significance is set at p < 0.05. One-way repeated measures analysis of variance was used to obtain the profile plots to demonstrate serial hemoglobin level at different time frame.
Bivariate correlation analysis and simple linear regression were used to identify variables that influenced the total blood loss. The independent variables were age, body weight, height, total body blood volume, preoperative hemoglobin level, Cobb angle of spine, vertebral level being fused, screws used, duration of surgery, and skin incision length.
Results
Sixty patients were eligible for trial entry (Figure 1). Sixteen patients were excluded (exclusion criteria (n = 12), refusal (n = 4)), leaving 44 patients for analysis. No differences in the basic demographic characteristics and operative details were observed (Table 1).

Patient flow diagram.
Characteristics and operative details of study participants.a
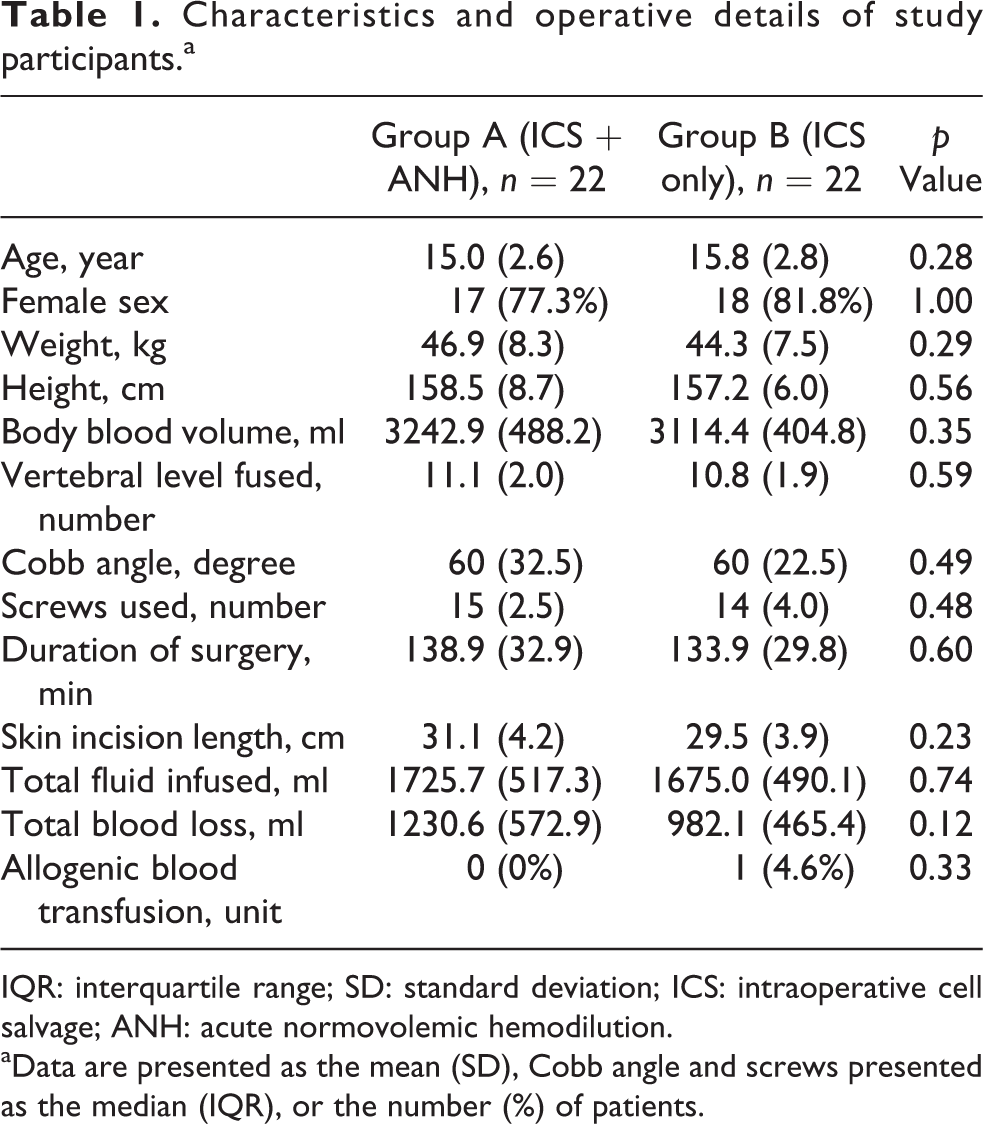
IQR: interquartile range; SD: standard deviation; ICS: intraoperative cell salvage; ANH: acute normovolemic hemodilution.
aData are presented as the mean (SD), Cobb angle and screws presented as the median (IQR), or the number (%) of patients.
There was no difference in terms of total blood loss in both groups. One patient from group B received 1 unit of allogenic blood transfusion but it was not significant (p = 0.33; Table 1). The hemoglobin and hematocrit values between different time frames are shown in Table 2.
Mean hemoglobin and hematocrit values.

ICS: intraoperative cell salvage; ANH: acute normovolemic hemodilution.
The total perioperative drop in hemoglobin level defined as the difference in hemoglobin level between preoperation and postoperation 24 h across the two groups (group A 2.79 ± 1.15, group B 2.76 ± 1.00) showed no significant difference (p = 0.93; Table 3).
Perioperative hemoglobin levels at different time frames.
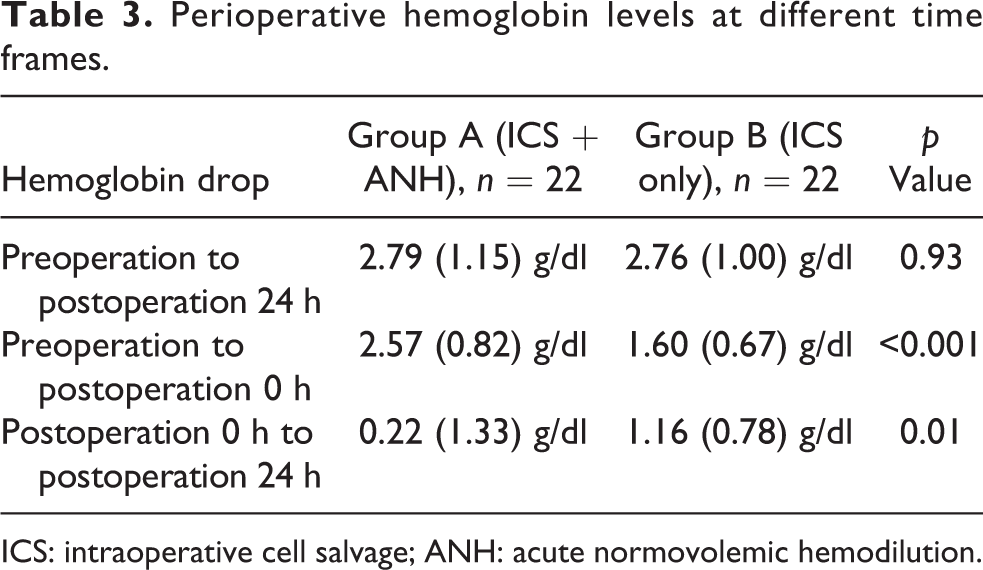
ICS: intraoperative cell salvage; ANH: acute normovolemic hemodilution.
Group A observed a larger hemoglobin drop at postoperative 0 h compared to initial preoperative level (2.57 ± 0.82 g/dl), followed by a smaller decrease within the next 24 h (0.22 ± 1.33 g/dl). Group B showed a continued drop in hemoglobin level of similar magnitude at postoperation 0 h (1.60 ± 0.67 g/dl) and within the next 24 h (1.16 ± 0.78 g/dl; Figure 2, Table 3). These results were statistically significant B (p < 0.05).

Serial mean hemoglobin levels at preoperation, postoperation 0 h, and postoperation 24 h.
For both group A and B, significant positive correlations between number of vertebral level fused (r = 0.44, p = 0.04 vs. r = 0.60, p = 0.00), number of screws inserted (r = 0.51, p = 0.02 vs. r = 0.79, p = 0.00), duration of surgery (r = 0.56, p = 0.01 vs. r = 0.52, p = 0.01), skin incision length (r = 0.61, p = 0.00 vs. r = 0.56, p = 0.01), and total blood loss with medium (r ≥ 0.3) to large effect size (r ≥ 0.5) were noted. For group A, preoperative hemoglobin level showed significant positive correlation with total blood loss, r = 0.49, p =0.02 with medium effect size. Whereas, for group B, there was significant positive correlation between Cobb angle and total blood loss, r = 0.46, p = 0.03 with medium effect size (Table 4).
Bivariate correlations of variables and total blood loss for group A and group B.

ICS: intraoperative cell salvage; ANH: acute normovolemic hemodilution.
aCorrelation is significant at the <0.05 level (two tailed).
bCorrelation is significant at the <0.01 level (two tailed).
Discussion
Perioperative outcome of AIS patients undergoing PSF is dependent on few factors, which include intraoperative blood loss and allogenic blood transfusion. The amount of intraoperative blood loss is unpredictable. Many studies have reported on factors that affect blood loss in scoliosis surgery. These may be patient factors such as gender, skeletal maturity, Cobb angle, kyphosis, activated partial thromboplastin time level and fibrinogen level, and menstruation cycle phase 15 –19 or surgery-related, number of fusion level, operative time, stages of surgery, number of osteotomies, and surgical approach. 2,15,17,19 –23 Some of the above factors such as number of vertebral levels fused, number of screws inserted, duration of surgery, and Cobb angle demonstrated positive correlation with total blood loss in our study. Recently, a dual surgeon approach was also reported to result in shorter operative time, less blood loss, and lower risk of allogenic blood transfusion. 24
However, a lot of these factors are nonmodifiable. Blood conservation techniques have also been extensively studied. Among the strategies that have been investigated include the usage of autologous blood transfusion, 25 –27 cell salvage, 28 and the usage of various pharmacological agents like esmolol, 29 tranexemic acid, 30,31 amicar, 32,33 aprotinin, 34,35 and epsilon aminocaproic acid 36,37 to reduce blood loss. Two popular strategies that are frequently employed in PSF for AIS are ANH and ICS techniques.
Copley et al. carried out a case–control study on the effect of ANH in 86 AIS patients who underwent PSF surgery. Some of the subjects underwent preoperative autologous donation. Both case and control group received cell saver and hypotensive anesthesia, and the case group received additional ANH technique. Transfusion requirement were significantly higher in the nonhemodilution group (79% vs. 37%). 38 De Oliveira et al. demonstrated the benefit of ANH in 25 AIS patients who underwent PSF. Allogenic blood was required predominantly in nonhemodilution group as compared to hemodilution group (79% vs. 28%). 39 A randomized controlled trial by Lim et al. found that ANH coupled with intraoperative esmolol-induced hypotension in spine surgery significantly reduced the incidence of allogenic blood transfusion (67% vs. 100%). 40
However, the evidence regarding ICS was conflicting. A randomized controlled trial by Zhang et al. showed that ICS significantly reduced the incidence of allogenic blood transfusion in patients undergoing scoliosis surgery (31% vs. 100%). 10 Bowen et al. in his retrospective case–control study involving 54 AIS patients who underwent surgical correction reported a significantly lower allogenic transfusion rates and volume in the ICS group, particularly in long surgeries and estimated blood loss of more than 30% of total blood volume. 11 Liang et al. recently in their study confirmed that the use of cell saver significantly reduced the need for allogenic blood transfusion. 14 However, Weiss et al. concluded that the use of ICS did not reduce the need for allogenic blood transfusion in scoliosis surgery. 12
In the literature, the benefit of combined ANH and ICS was not well established. So this study was designed to assess the magnitude of change in the hemoglobin values perioperatively when comparing ANH combined with ICS versus ICS alone in PSF surgery. The decrease in hemoglobin levels between preoperation and postoperation 24 h was slightly higher in group A (ANH plus ICS) 2.79 ± 1.15 g/dl, compared to group B (ICS only) 2.76 ± 1.00 g/dl, and this was not statistically significant. However, when we examined the hemoglobin trends at different time frames, that is, between preoperation and postoperation 0-h period and between postoperation 0-h and postoperation 24-h period, the drop in hemoglobin levels was statistically significant. The values are shown in Table 3.
This pattern of hemoglobin drop in group A could be attributed by higher total blood loss in group A (1230.64 ± 572.89 ml) compared to group B (982.14 ± 465.44 ml). Furthermore, the initial larger drop in hemoglobin level in group A could be contributed by the hemodilution effect of ANH. Bourke and Smith 41 reported that hemoglobin concentration declines exponentially during ANH. In group A, when the collected whole blood (from ANH) and red cell concentrates (from ICS) were returned to the patient at the end of surgery, it replenished the intravascular plasma: erythrocytes fraction proportionately, however, this redistribution between interstitial compartment and intravascular compartment did not occur instantly but only took places after 8–12 h. This could explain the subsequent stabilization of the postoperation hemoglobin gap observed in group A. We did not see this in group B, in which the level of hemoglobin showed a continuous drop of similar magnitude postoperatively. Therefore, the combined technique could possibly produce a more stable and reliable hemoglobin trends within the first 24 h.
In this study, group A did not show additional benefit over group B. This could be as a result of ineffective hemodilution technique. The magnitude of hemodilution has been shown to affect the efficacy of ANH. In brief, a more profound hemodilution would result in fewer red cells lost during surgery. 42,43 However, the margin of safety is uncertain with higher degree of dilutional anemia.
The addition of ANH to ICS does not reduce the risk of allogenic blood transfusion. However, this study was not powered to analyze this outcome. Since the magnitude of hemoglobin drop between preoperation and at 24 h postoperation was similar in both groups, we could infer that the need of allogenic blood transfusion will not be influenced by either technique. Other factors such as the starting hemoglobin concentration, total blood loss, and the transfusion trigger would have to be taken into consideration.
Our study had several limitations. The postoperative hemoglobin was assessed at 24 h after the operation. Grant et al. demonstrated that the maximum hemoglobin drop was found to occur on day 3 of postoperation and became more stable afterward. 44 Future studies shall consider monitoring the hemoglobin trends for a longer period postoperatively. In this study, we attempted to estimate as accurately as possible the intraoperative blood loss, however, error in measurement would still exist due to unaccounted loss in the drapes and gown. Future studies shall also consider a more effective hemodilution technique involving a larger volume of blood. In this study, we used IV tranexamic acid as antifibrinolytic agent to reduce blood loss but both groups of patients received it. We did not have a control group in this study because the investigators did not want to expose the risk of allogenic blood transfusion to the patients. 10,11,14 We did not include postoperative drainage into the estimation of the blood loss in this study.
In conclusion, the addition of ANH technique to ICS technique during PSF surgery for AIS resulted in a similar decrease in hemoglobin levels between preoperative values and at 24 h postoperatively.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.