
Abstract
By analyzing a case of total knee arthroplasty (TKA) in a knee with complex deformity and secondary osteoarthritis, we demonstrated the rationale of preoperative planning and the detail of intraoperative execution. The lady had right TKA with combined medial closing wedge femoral osteotomy, neutral wedge valgus derotational tibial osteotomy, fibular osteotomy, and quadriceplasty. Four months later, she had left TKA. Osteotomies healed well and she was pain-free at 18 months after right TKA. Combination of intra-articular and extra-articular correction of deformity was the key to achieve a well-aligned TKA with good soft tissue balancing in both coronal and sagittal planes. The choice of osteotomy fixation method should follow the principles of bone healing. Fibular osteotomy should have been made at the level of tibial osteotomy with caution. Use of appropriate TKA prosthesis could have enhanced the osteotomy fixation while decreasing the complication.
Introduction
Extra-articular deformity of femur and/or tibia increases the difficulty of total knee arthroplasty (TKA). To align the TKA prosthesis along the mechanical axis of lower limb, the deformity has to be corrected by either intra-articular or extra-articular method. 1,2 Femoral deformity is especially more difficult to manage by intra-articular correction because it would produce asymmetry of extension and flexion gap. 2 This can be further complicated when there are co-existing torsional deformity and shortening of femur or tibia, and extensor mechanism malalignment. Therefore, preoperative planning is important for accurate intraoperative execution and choice of correct implant and prosthesis. We also need to thoroughly discuss with the patient to get her trust, build the rapport, and explain the potential risks and benefits and also the rehabilitation plan.
Most of the literatures 2 –7 about the TKA in the presence of extra-articular deformity reported cases of either femoral or tibial deformity and managed by concomitant single osteotomy. Moyad et al. 8 discussed about the technical detail of simultaneous femoral and tibial osteotomies during TKA. However, preoperative planning, details of deformity, and choice of osteotomy fixation implant were not clearly discussed. In this report, we will elaborate all the preoperative and technical details in the correction of combined femoral, tibial, and extensor mechanism deformities during primary TKA.
Case summary
A 56-year-old lady had right knee deformity after a right knee operation at 8-years old. She complained of bilateral knee pain for 6 years and failed to respond to conservative treatment with shoe raise, knee brace, and analgesics. Her walking tolerance was limited to 15 min. Physical examination showed bilateral genu varum deformity, tenderness in all three compartments, and knee range of motion from 0° to 100°. Right knee had 10° extension lag. An old surgical scar was present at her right proximal medial tibia. Her right patella was laterally subluxed and tibial tuberosity (TT) faced laterally. The patella tendon lengths were equal bilaterally (Figure 1(a) and (b)). The right medial collateral ligament (MCL) was intact while the lateral collateral ligament had grade II laxity. The right tibial segment was 4 cm shorter, while both femurs were equal in length. Apparent limb length of right lower limb was 65 cm, and left side was 68 cm. She walked with right-sided short-limb gait and varus thrusting. Standing scanogram of both lower limbs, knee lateral and skyline X-ray were taken (Figure 1(c) to (e)). Computer tomography (CT) of right hip, knee, and ankle was done to check the rotational profile and visualize the bony deformity by 3-D reconstruction (Figure 2)

Preoperative clinical pictures and X-ray. (a) Standing photograph of both lower limbs. (b) Close-up frontal view of right knee when she was lying supine. (c) Skyline X-ray of right knee showing lateral patella subluxation. (d) Standing scanogram of both lower limbs. Right/left FTA are 54°/20°. Right/ left mLDFA are 74°/89°. Right/left MPTA are 33°/78°. (E) Anteroposterior and lateral X-ray of right knee. Insall–Salvati index (b/a) = 1. FTA: femoral tibial angle; mLDFA: mechanical lateral distal femoral angle; MPTA: medial proximal tibial angle.

CT of right knee. Line A: femoral neck axis. Line B: posterior condylar axis. Line C: anteroposterior axis of proximal tibia. Line D: transmalleolar axis. Line E: perpendicular to line B passing through the TG. Line F: parallel to line E passing through TT. Femoral neck anteversion (AB angle) is 30°. Foot–thigh angle (BD angle) is 20° external rotation. Torsional deformity of proximal tibia (CD angle) is 40° external rotation. TT–TG distance is 40 mm. CT: computer tomography; TG: trochlear groove; TT: tibial tuberosity.
Preoperative planning
Analysis of problems
Her right TT pointed laterally while her right ankle faced anteriorly. This indicated an external torsional deformity of the proximal tibia. The significant medial proximal tibial defect as shown in anteroposterior (AP) X-ray actually represented a posteromedial proximal tibial defect. CT scan (Figure 2) confirmed the findings: (1) patella sitting on the lateral femoral condyle, (2) 40° of proximal tibial external torsional deformity and 40 mm of TT-TG distance, and (3) proximal tibial bony defect at the posteromedial region. The entire extensor mechanism of quadriceps muscle and patella was expected to be contracted and adhered to the lateral femur as in the situation of congenital patella dislocation. 9 The patella height was normal (Figure 1(e)). There was grade II laxity of lateral collateral ligament.
Bilateral femurs were of equal length of 41 cm. In Figure 3(a), right anatomical medial proximal femoral angle was 96°, indicating coxa valga. Her right hip was asymptomatic, and proximal femoral osteotomy was not necessary. Distal femoral valgus deformity of 13° with CORA at 60 mm from distal femoral joint line was present.
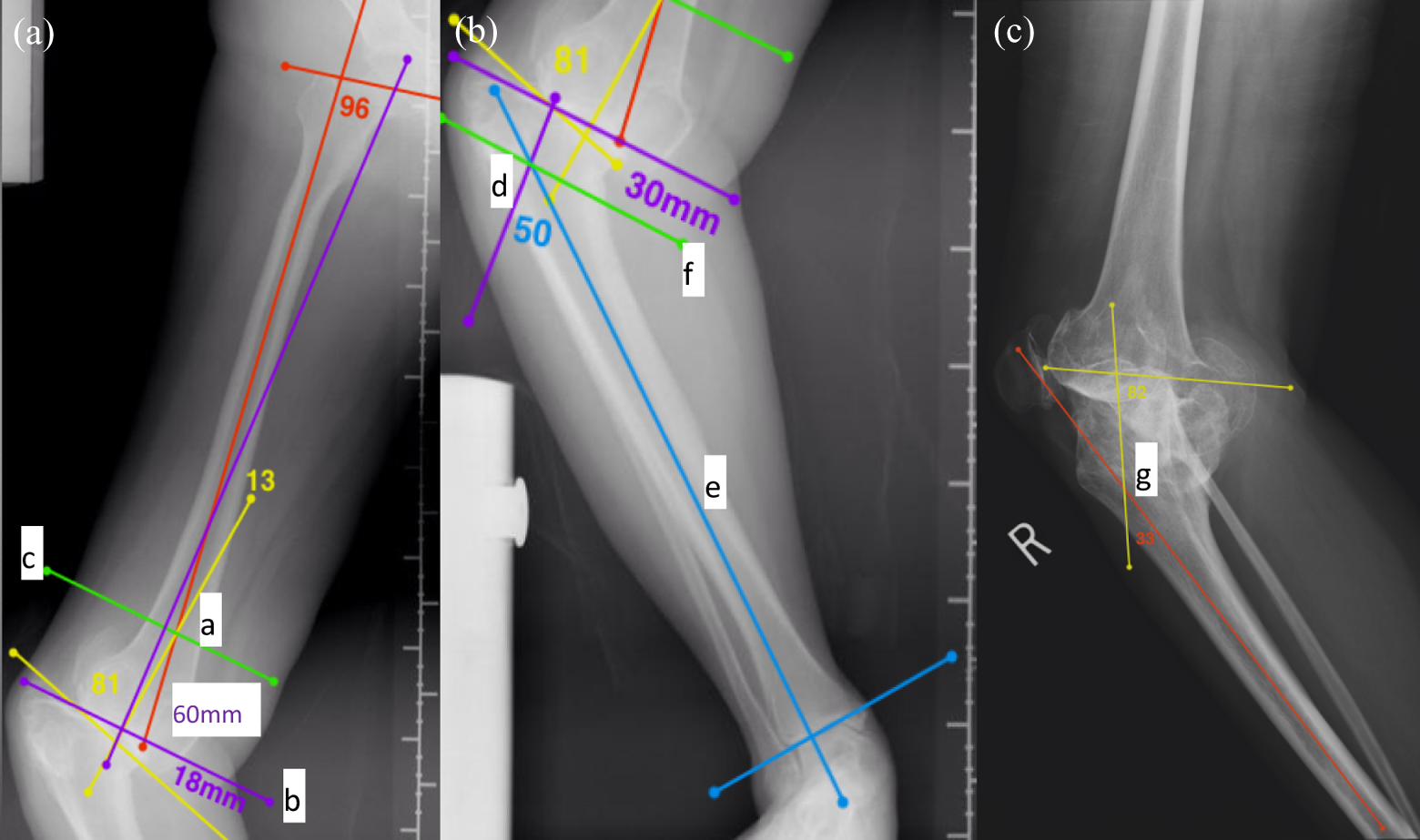
Preoperative planning for femoral and tibial deformity correction. (a) Point a: CORA formed by intersection of anatomical axes of proximal segment (red line) and distal segment (yellow line) at 60 mm from distal femoral joint line. Line b: perpendicular to mechanical axis of femur anticipating femoral condylar resection for intra-articular deformity correction. Line c: plane of femoral osteotomy for extra-articular correction. (b) Point d: CORA formed at 30 mm from proximal tibial joint line. Line e: anatomical axis of distal tibial segment. Line f: plane of tibial osteotomy for extra-articular correction. (c) Point g: CORA of proximal tibia in sagittal plane. CORA: center of rotation of angulation.
Right tibia was 4 cm shorter. Figure 3(b) indicated a coronal-plane varus deformity of 50° with CORA at 30 mm from proximal tibial joint line. Figure 3(c) showed a sagittal plane procurvatum deformity of 33° with CORA just distal to TT. By method of trigonometry, 10 the resultant oblique plane angular deformity was 60° with apex pointing anterolaterally in the plane forming 33° from frontal plane.
Treatment options
The first method was primary TKA with rotating-hinge knee tumor prosthesis. The marked posteromedial tibial defect could be replaced by custom-made prosthesis. This involved sacrificing the collateral ligament and using greater prosthesis constraint. This posed a potential problem of limited prosthesis longevity in a young lady. 11 Moreover, the tibial torsional deformity could only be corrected by derotational osteotomy.
The second method was two-stage primary TKA. First stage is acute varus distal femoral osteotomy and the use of the Ilizarov method for gradual tibial correction. Prolonged period of use of external fixator was expected for 40 mm lengthening, 40° derotation, and 60° angular correction. Nonunion of distraction osteogenesis and pin-tract infection were potential complications that would increase risks of second stage of TKA.
The third method, chosen by patient, was one-stage primary TKA and tibial with/without femoral osteotomy. Right lower limb shortening could not be corrected. There was greater technical difficulty. The postoperative recovery period was intermediate among all three methods.
Surgical planning
Femoral deformity correction (Figure 3(a))
The anticipated distal femoral condylar resection for intra-articular correction cut at 18 mm from distal medial femoral condylar joint line. The resultant trapezoidal extension gap increased the difficulty of soft tissue balancing. The MCL femoral origin was located intraoperatively to determine whether it would be jeopardized by the anticipated cut. About 13° medial closing wedge osteotomy at 60 mm from distal femoral joint line was the contingency plan to realign the distal to the proximal segment. The chosen model of TKA was Press Fit Condylar (PFC) Sigma posterior stabilized (Depuy, Leeds, England) because it allowed addition of metal augment or intramedullary rod. The depth of femoral box cut for size 2–3 was 23.8 mm from joint line. Conversion to Total Condylar 3 (TC3) was also possible in case of lateral collateral insufficiency, and the box-cut depth was 29.1 mm. This would not split the distal femoral segment after osteotomy.
Osteotomy could be fixed by lag screw and long cementless rod. Tomofix medial distal femur (MDF; DepuySynthes, Oberdorf, Switzerland) could also be used when short cemented rod was used. Short unicortical locking screws were necessary to avoid the femoral box and the rod. Cemented rod had the advantage of greater freedom of femoral component offset placement in case of dysplastic femur.
Tibial deformity correction (Figure 3(b))
Anatomical axis of distal tibial segment passed outside the tibial plateau; therefore, intra-articular correction was not possible. 4 The osteotomy plane was 30 mm distal to and parallel to the articular surface. Neutral wedge osteotomy followed by derotation was planned because this could provide reasonable bony stability and avoid further tibial shortening. Because of the anticipated medial gap at osteotomy site, fixation was accomplished with double methods of long cementless intramedullary rod and LCP medial proximal tibial plate 3.5 (DepuySynthes, Oberdorf, Switzerland). Concomitant fibular osteotomy at the distal mid-third was planned to minimize the risk of injury of deep peroneal branch to extensor hallucis longus and allow the valgus correction of tibial deformity. 12
Extensor mechanism realignment
After the implantation of TKA trial prosthesis and fixation of osteotomy, the patella tracking and also the flexion knee range were tested for abnormality. Quadricepsplasty 9,13 was performed to derotate the quadriceps together with muscle slide.
Surgical technique
Her right lower limb was prepared from groin to toe, and sterile tourniquet was used. Longitudinal lateral parapatellar incision was made to maintain a 5-cm skin bridge with the old medial longitudinal scar and facilitate the planned quadricepsplasty. Medial parapatellar arthrotomy was performed for an adequate knee exposure and easier femoral and tibial osteotomy from medial side. The MCL femoral origin from articular margin was measured to be 18 mm (Figure 4(a)). There was risk of MCL injury if further distal femoral cut was necessary to balance the flexion and extension gap. Medial distal femoral closing wedge osteotomy was done (Figure 4(b)). Because of the significant dysplasia of femoral condyle and possible mismatch with femoral canal center, osteotomy was fixed with Tomofix and unicortical screws in the presence of intramedullary reaming rod.

Surgical technique. (a) The MCL femoral origin from articular margin was measured to be 18 mm. (b) Medial distal femoral closing wedge osteotomy of 13° was done at 60 mm from the distal femoral joint line. (c) The medial soft tissue had 10 mm more laxity in flexion gap as shown. (d) Proximal tibial osteotomy done at 3 cm from joint margin was found distal to MCL tibial insertion and TT. (e) Medial plate fixation using unicortical locking screws was performed with the reaming rod in-situ. (f) Operation was completed with fixation of distal femoral osteotomy with Tomofix medial distal femur plate, fixation of tibial osteotomy with medial proximal tibial plate and total knee replacement. TT: tibial tuberosity; MCL: medial collateral ligament.
TKA was done in the extension gap first technique by conventional intramedullary femoral guide. The medial soft tissue had 10 mm more laxity in both extension and flexion (Figure 4(c)). Fibular osteotomy at distal mid-third with 1 cm excision was done. Proximal tibial osteotomy done at 3 cm from joint margin was found distal to MCL tibial insertion and TT (Figure 4(d)), by which medial–lateral (ML) soft tissue tension would not be changed after osteotomy realignment. The plane of tibial osteotomy was made at 10° divergent from joint surface so that 10 mm more was cut from lateral side on proximal tibia cut for TKA after realignment of osteotomy, and the ML soft tissue would be more balanced. Neutral wedge of proximal end of distal fragment was excised. The proximal tibial segment was put in valgus direction and was impeded by the long proximal fibular segment. With sustained valgus force, the tibia was reoriented while fracture crack of fibula was heard. Intramedullary reaming of tibia was performed through both segments. The medial third of TT was realigned with second toe for rotational correction. Medial plate fixation using unicortical locking screws was performed with the reaming rod in situ (Figure 4(e)).
After the proximal tibial cut with jig, the reaming rod was removed to check the extension gap ML soft tissue balancing, which was satisfactory. However, the flexion gap was found to be larger than extension gap. About 2 mm more distal femoral cut was performed. Femoral component was sized, and the AP cutting jig mounted onto distal femur confirmed the larger flexion gap. One larger size AP cutting jig with +2 mm anterior stem offset was mounted onto femoral intramedullary reamer to decrease 6 mm flexion gap while achieving ML soft tissue balancing. After completion of AP femoral cut, the flexion gap was found to be 4 mm larger than extension gap. In order to prevent postoperative cam jump, TC3 with larger post was necessary. TC3 femoral box and chamfer cuts were made. The trial femoral component with short cemented stem was fitted successfully. Trial tibial tray with stem was inserted to test soft tissue balancing. Patella was then cut and resurfaced with trial.
Good patella tracking could not be achieved. Proximal skin incision was extended. Lateral retinaculum was released and vastus lateralis was mobilized from the lateral intermuscular septum and anterior femur by subperiosteal dissection. The whole quadriceps and patella were centralized with passive knee flexion. After pulsatile lavage, augmented fixation of lateral femoral condyle to shaft was done by 3.0-mm titanium screws, and the definitive components were cemented with Palacos R+G cement (Zimmer; Figure 4(f)). Autogenous cancellous bone graft was packed around the femoral and tibial osteotomy sites. Wound was closed with suction drain. Intraoperative range of motion was 0° to 120°.
Postoperative care and results
Her right knee was immediately mobilized after operation. She started nonweight bearing walking exercise on the next day and changed to partial weight-bearing walking at the 7th week and then proceeded to full weight bearing walking at 3 months. Left primary TKA was done at 4 months after right TKA. On serial monitoring of healing of osteotomy, the medial part of femoral osteotomy healed last. At 18 months after operation, she could walk unaided and resume original duty. True right lower limb length was 5 cm shorter (Figure 5(a)). Bilateral apparent limb lengths were equal at 71 cm. Her right knee active range was 5° to 85°, and left knee active range was 0° to 95°. Standing scanogram showed good position of both TKAs (Figure 5(b)).

Result at 18 months after operation. (a) Clinical photograph. (b) Standing scanogram.
Discussion
Deformity
Extra-articular knee deformities can be uniplanar, biplanar, or triplanar. 4 In our report, the lady had a uniplanar valgus deformity of distal femur and a triplanar deformity of the tibia. The latter was a severe Blount-like deformity of varus, procurvatum, and internal torsion. 14 This combination of valgus femoral and varus tibial deformity has been recognized as a particularly poor prognostic pattern, 15 and destabilized the knee to lateral subluxation, and led to osteoarthritic change. Interestingly, the extensor mechanism malalignment, which commonly happened in the valgus knee, added to the femoral–tibial varus deformity to form a triple deformity. This was because of the markedly increased TT-TG distance of 40 mm and the torsional deformity of the proximal tibia.
Femoral and tibial osteotomy
Moyad et al. 8 advocated that all intra-articular bone resections were performed first, without regard to the coexisting extra-articular femoral and tibial deformities. Distal bone cut was made parallel to the preexisting femoral joint line and then the AP and chamfer cuts were completed with reference to transepicondylar axis. The tibial cut was then performed parallel to preexisting tibial joint line obliquity. The extra-articular deformities of tibia and femur were then corrected under X-ray control to restore the mechanical alignment.
If the same method had been applied to the lady in this report, a few problems would be anticipated. First, a trapezoidal gap would have been made with medial side 10 mm larger. Second, the flexion gap would be 10 mm larger than extension gap, and this led to a difficult salvage. Third, patella tracking would have been even worse because femoral component rotation could not be corrected to compensate.
We advocated the use of extension gap first technique to solve this problem and created a rectangular extension gap. This could be done before or after osteotomy; the latter of which was technically easier in case of complex deformity and X-ray was not necessary. The size and rotation of femoral component could also be adjusted to attain a rectangular flexion gap after the tibial platform was fixed.
Although the femoral osteotomy surfaces were closely apposed with fixation of Tomofix and cemented rod, the healing on the medial part under the Tomofix was slower than the lateral part, where additional lag screws were applied. There was no problem with healing of tibial osteotomy where cementless rod and locking plate were used. We postulated that delay in healing was a result of conflict of principle of fixation on the medial side, where cemented rod across the osteotomy site did not allow micromotion but Tomofix plate encourage secondary bone healing by micromotion. For the lateral femoral condyle, primary bone healing occurred, while secondary bone healing happened in the tibial osteotomy.
Change in flexion and extension gaps after correction of tibial deformity
By getting a rectangular flexion and extension gaps by intra-articular resection, we were dealing with ML soft tissue balancing in coronal plane. This could be maintained after deformity correction by osteotomy beyond the origins and insertions of collateral ligaments. However, in the sagittal plane, the tibial osteotomy was also distal to TT and posterior capsular attachment. After correction of 33° of tibial procurvatum deformity, TT was moved more distally and posterior articular edge moved more proximally. Anterior soft tissue tension became tight while the posterior tissue tension was loose. This led to tighter extension gap and looser flexion gap.
Fibular osteotomy
Aydogdu et al. 12 recommended that this should be performed at the middle to distal third junction to avoid peroneal nerve dysfunction after high tibial osteotomy. A short fibular fragment should be resected in case of a considerable degree of correction. We used the same method and found fibular impingement during the angular correction of tibia. The proximal fibula at the level of tibial osteotomy was fractured with sustained force.
We echoed the practice of fibular osteotomy at the same tibial level by Moyad et al. 8 This was important as in our case of 50° correction. Kirgis et al. 16 defined the proximal 65 mm of fibular head as safe zone. The dissection around the fibula had to be on the bone because the superficial peroneal nerve coursed 7–12 mm anteriorly to fibula in the proximal third. 12
Choice of TKA prosthesis
Moyad et al. 8 used NexGen CR knee system (Zimmer, Warsaw, IN, USA), by which femoral box cut was not necessary and intramedullary rod added to femoral and tibial components could fix the osteotomy. However, the use of cruciate-retaining TKA system was difficult in case of severely deformed knee as in our case. Medial pivot knee (Wright Medical Technology, Arlington, TN, USA) was advocated by Choi et al. 17 for treatment of distal femoral fractures with osteoarthritic knee. Posterior cruciate ligament could be sacrificed during soft tissue balancing without femoral box cutting. This provided the advantage of AP knee stability. Femoral bone stock was also preserved without risk of communicating with fracture or osteotomy site. The use of plate with bicortical screw fixation would also be easier. However, the stemmed medial pivot knee system was not available in Hong Kong. Therefore, the usual system, PFC sigma and TC3, was chosen. The risk of iatrogenic intercondylar femoral fracture was avoided by planning osteotomy site well proximal to box cut.
Conclusions
From the literature search, this is the first report of detailed analysis of deformity, planning, and surgical technique of TKA in a knee with triple deformity of femur, tibia, and extensor mechanism. Preoperative planning is important to allow the surgeon to have greater flexibility. With the advance of 3-D printing technology, the diseased bone model could have been generated for trial of osteotomy and correction in case of this severe deformity. Computer navigation can also be a useful tool in appropriate situation. 18
Combination of intra-articular and extra-articular correction of deformity, as shown in this report, is the key to achieve a well-aligned TKA with good soft tissue balancing in both coronal and sagittal planes. The combination of osteotomy fixation methods should be compatible with the principle of bone healing. Fibular osteotomy at the level of tibial osteotomy makes the deformity correction easier. Use of appropriate TKA prosthesis can enhance the osteotomy fixation while decreasing the complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.