
Abstract
Purpose:
Racial difference in the femoral geometry may exist. Asian femurs may be more externally rotated. If anatomical differences in distal femur had existed between Caucasians and Asians, the group with 5° external rotation of the femoral component should have shown better results than the group with 3° external rotation of the femoral component have.
Methods:
598 patients underwent total knee arthroplasty in our institution, among whom 83 patients (115 knees) who had postoperative computed tomography (CT) were studied retrospectively. Sixty-two knees were set in 5° of external rotation of femoral component relative to the posterior condylar axis (group A) while the others (53 knees) were set in 3° (group B). The femoral component rotation (FCR) was measured and compared using CT. The patellar tilting (PT) and the lateral patellar displacement (LPD) were measured to evaluate the patellar tracking using Merchant view. And postoperative clinical scores were compared.
Results:
The mean FCRs showed no significant difference between two groups (p > 0.05). The mean PT and LPD showed no statistically significant difference either (p > 0.05). There were no statistical differences in clinical scores.
Conclusion:
The difference in the patellar tracking between the two groups could not be demonstrated. There were no statistical differences in clinical scores either. We concluded there is no need to adhere to 5° external rotation.
Keywords
Introduction
The rotational alignment of femoral and tibial components during a total knee arthroplasty (TKA) is an important factor that affects the overall functions of knee joint, and especially, the femoral component rotational alignment is known to affect flexion stability, tibiofemoral and patellofemoral kinematics, and alignment in flexion. 1 Useful reference axes for the rotational alignment of the femoral component include the transepicondylar axis (TEA), 2 –4 the posterior condylar axis (PCA), 5 and the midtrochlear line (Whiteside’s line), 6 and many studies have also been conducted on the anatomical relationships among these reference axes. After Moreland et al. 7 reported that the transverse axis of the knee had a 3° varus orientation relative to the mechanical axis of the tibia, 3° external rotation of the femoral component relative to the PCA has been accepted to be reasonable to obtain rectangular flexion gaps.
However, in a study of the axial alignment of Chinese lower extremities, Tang et al. 8 reported that the Chinese had knee joint medial inclinations of approximately 5° arguing that, therefore, 5° external rotation of the femoral component was necessary. In an anatomical study of the distal femur conducted with younger healthy volunteers, Chang et al. 9 reported that the angle formed by a line perpendicular to the mechanical axis of the tibia and the PCA was 5.1° in men and 6.6° in women. As such, there are still controversies over the appropriate external rotation degrees of the femoral component. 8,10,11
Although many studies have compared the results of different degrees of femoral component rotation (FCR), most of the results came from the comparison between a group with an internally rotated femoral component and a group with an externally rotated femoral component, 12 –15 and no study has compared the differences in the effects of different external rotation of a femoral component. We assumed that if anatomical differences in the distal femur had existed between Caucasians and Asians, the group with 5° external rotation of the femoral component should have better results than the group with 3° external rotation of the femoral component.
The purpose of this study is to see (1) which group is closer to the surgical TEA through postoperative computed tomography (CT) images and to evaluate (2) patella tracking through postoperative merchant views and (3) clinical scores in the group with 5° external rotation of the femoral component and the group with 3° external rotation.
Materials and methods
Study design criteria
Between January 2011 and October 2013, TKAs were performed in 598 patients. Of them, 83 patients (115 knees) who agreed to undertake the postoperative CT were reviewed retrospectively. We studied only the patients with varus alignment who underwent TKA due to osteoarthritis. Patients with posttraumatic arthritis, rheumatoid arthritis, or valgus deformity were excluded from the study. The surgery was performed by one senior author using the same implant in all cases (LPS Nexgen; Zimmer Inc, Warsaw, Indiana, USA).
Distal femoral bone was resected using intramedullary guide, and AP cutting was performed using an anterior referencing system in 3° or 5° of external rotation relative to the PCA, which was confirmed by Whiteside’s line. Tibial preparation was then undertaken using an intramedullary tibial guide with a cutting block with 7° of posterior slope by the manufacturer’s recommendation. After stability was confirmed by ligament balancing using the trial components, the femoral and the tibial components were fixed with cement. The degree of external rotation was decided randomly. Sixty-two knees were set in 5° external rotation of femoral component relative to the PCA (group A), and others (53 knees) were set in 3° (group B).
Patelloplasties were performed in all patients using the same method, but no patellar resurfacing was performed. After each patella lateral facetectomy, the hypertrophied synovium around the patella was removed using a Bovie and the osteophyte was removed using a rongeur. The no thumb test of patellar tracking was done during all surgeries in order to observe the reduced patella within the femoral trochlea during the knee motion before retinacular closure.
Radiological evaluation
FCR was evaluated by measuring the angle formed by the lines that connected the posterior margins of the femoral component and the surgical epicondylar axis (SEA) in the axial image from CT (Figure 1). The SEA was defined as a line that connects the tip of the lateral epicondyle and the medial epicondylar sulcus of the femur. 7,15 Cases where the femoral component was externally rotated relative to the SEA were indicated using positive values, and cases where the femoral component was internally rotated were indicated using negative values.
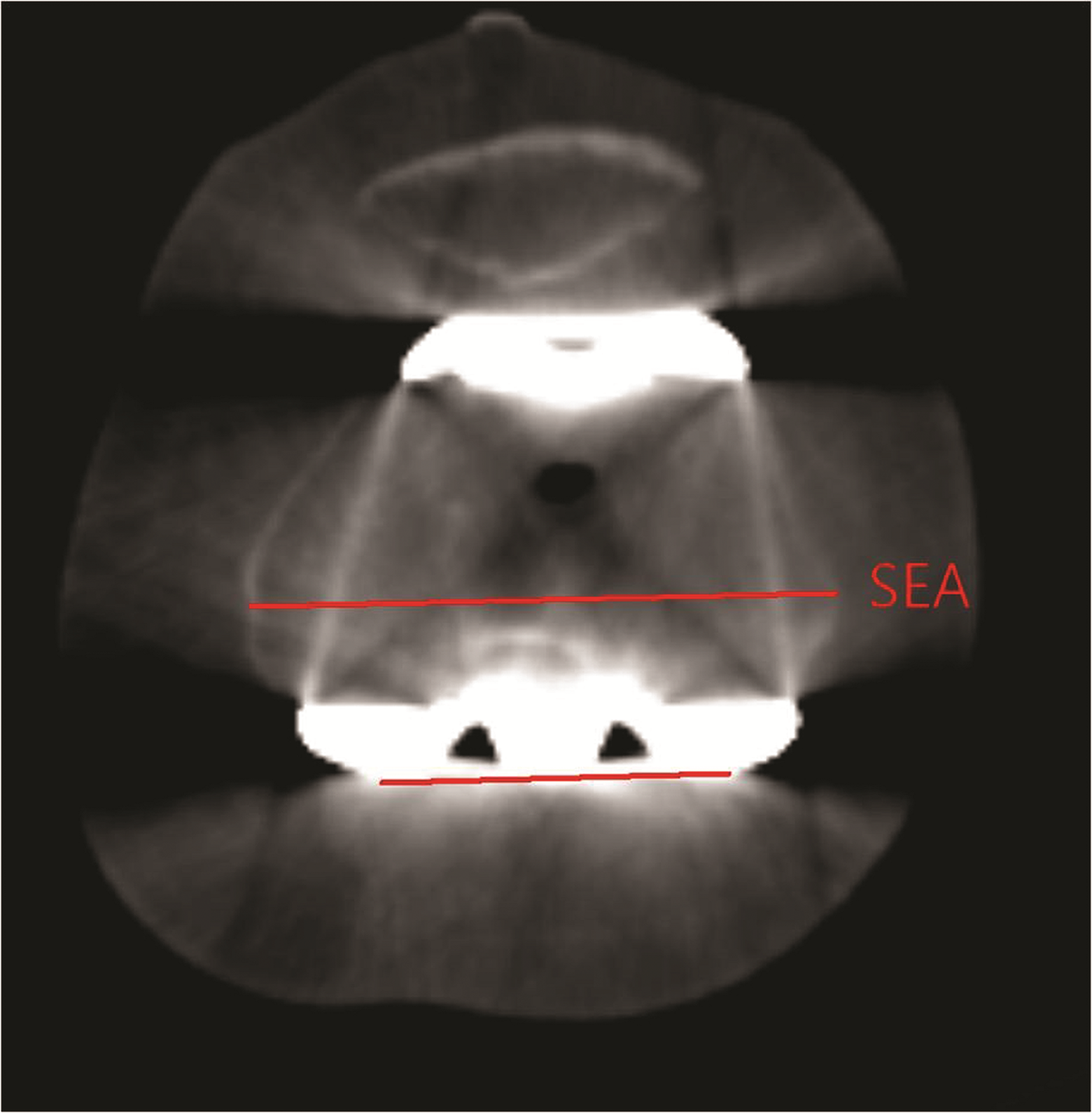
FCR was defined as the angle between the line that connected the posterior margins of the femoral component and the SEA. The SEA was defined as a line that connects the tip of the lateral epicondyle and the medial epicondylar sulcus of the femur. FCR: femoral component rotation; SEA: surgical epicondylar axis.
To evaluate patellar tracking, patellar tilting angle (PTA) and lateral patellar displacement (LPD) in Merchant view were used. PTA and LPD were measured from Merchant views obtained at 1 month after the surgery. PTA was defined as the angle between the anterior intercondylar line and the transverse axis of the patella (Figure 2). 16,17 The transverse axis of the patella is a line that connects the medial and lateral corners, which has been reported to be independent from the morphology of the patella. 16 PTA was defined to have positive values in cases where the transverse axis of the patella was laterally tilted relative to the anterior intercondylar line, and negative values in cases where the transverse axis of the patella was medially tilted. LPD was defined as the distance between the intercondylar sulcus and the median ridge of the patella. The intercondylar sulcus was defined as the lowest point of the femoral component relative to the anterior intercondylar line in Merchant views and the median ridge of the patella was defined as the deepest point of the patella relative to the transverse axis of the patella (Figure 3). The median ridge of the patella was defined to have positive values when it was located laterally to the intercondylar sulcus and to have negative values when it was located medially to the intercondylar sulcus.

PTA was defined as the angle between the anterior intercondylar line and the transverse axis of the patella. PTA: patellar tilting angle.
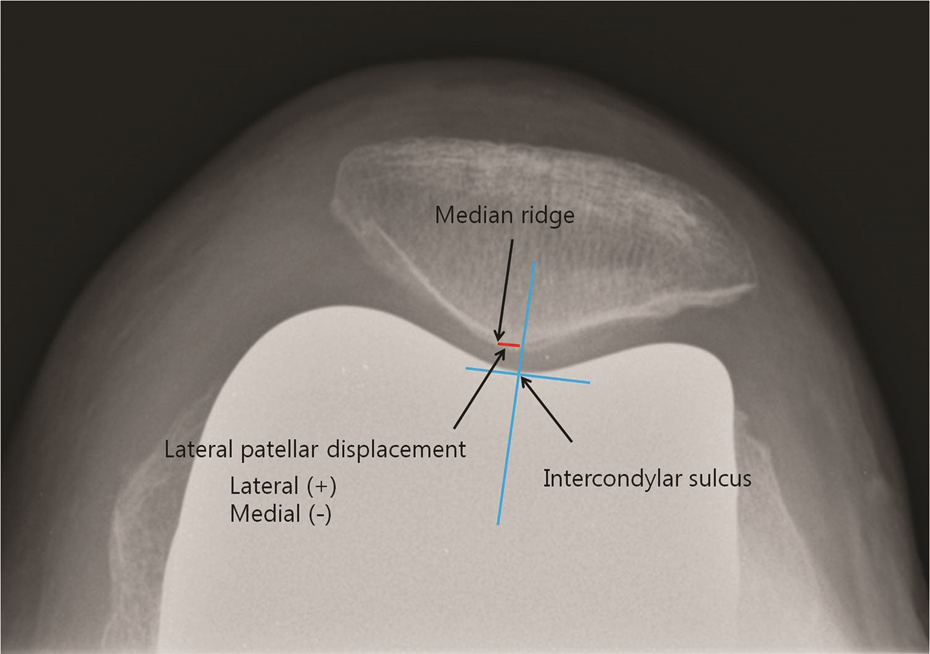
LPD was defined as the distance between the intercondylar sulcus and the median ridge of the patella. LPD: lateral patellar displacement.
FCR, PTA, and LPD were measured two times each by two independent orthopedists and the average values were used in the study.
Clinical evaluation
The knee society score (KSS), knee society function score (KSS-function), and hospital for special surgery score (HSS) were recorded by one author in outpatient department preoperatively. We also compared the KSS, KSS-function, and HSS between two groups at postoperative 6 months.
Statistical analysis
IBM SPSS statistics version 19.0 (SPSS, Inc, an IBM Company, Chicago, Illinois, USA) was used for the statistical analyses. Mann–Whitney U-tests were used for comparison of FCR between groups A and B and Student t-tests were used for comparison of PT and LPD between the two groups.
T-test was used to compare between two groups at baseline values in all clinical scores which include KSS knee score, KSS function score, and HSS. Analysis of covariance was used to determine whether significant differences existed between pre- and postoperative scores of two different groups with baseline measurements used as covariates in the analysis. The results were defined to be statistically significant when the p value was less than 0.05.
Results
The mean age of the patients was 70.3 years old (range: 49–86) and the patients consisted of 80 females (112 knees) and 3 males (3 knees). The average FCR of group A was 1.8° ± 1.9° and that of group B was 1.1° ± 1.3°, and the difference was not statistically significant (p > 0.05). PTA and LPD in group A were 9.7° ± 6.2° and −2.8 mm ± 2.6 mm, respectively, and those in group B were 10.1° ± 4.7° and −3.0 mm ± 2.2 mm, respectively, and none of PTA and LPD showed any statistically significant difference between groups A and B (p > 0.05). There were no differences in clinical scores between two groups statistically (p > 0.05; Table 1).
Comparison of femoral component rotation, patellar tilting, LPD, and pre- and postoperative clinical scores between groups A and B.a
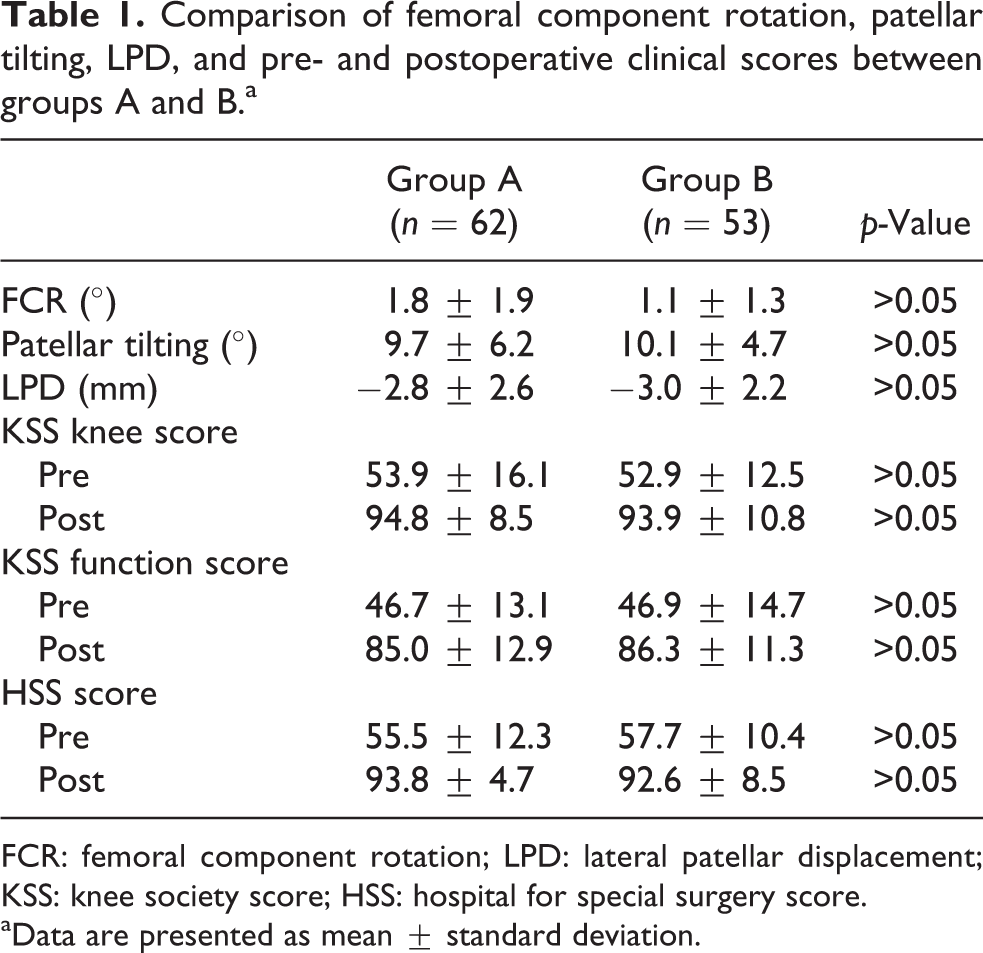
FCR: femoral component rotation; LPD: lateral patellar displacement; KSS: knee society score; HSS: hospital for special surgery score.
aData are presented as mean ± standard deviation.
Discussion
The most important finding of the present study is that there was no significant difference in the patellar tracking according to the different FCR with 3° and 5°. Although there are controversies over which reference axis is the most reliable and reproducible, the PCA is one of useful references used in many TKA systems. 5 Through the results of many previous studies on the rotational alignment of the femoral component, it can be observed that the PCA is internally rotated by 3° on average relative to the surgical TEA and by 5° on average relative to the clinical TEA. 1,5 Therefore, 3° external rotation of the femoral component relative to the PCA is generally recommended. 1,5 The femoral component can be located parallel to the TEA so that it corresponds to the functional flexion–extension axis and the patellar tracking. 18
An in vivo study using a biplanar image-matching technique demonstrated that the functional flexion–extension axis of the knee corresponds to the SEA. 18 Practically, however, the use of this axis is limited because it is not easy to localize the sulcus of the medial epicondyle precisely during surgery. 18
The effects of femoral component malrotation on the outcomes after TKAs have been reported in many studies. 12 –15,19 Akagi et al. 12 compared a group having the femoral component implanted with neutral alignment relative to the PCA and a group having the femoral component implanted with 3–5° external rotation and reported that the externally rotated group showed better postoperative patellar tracking. In a study conducted with patients with isolated patellofemoral complications, Berger et al. 20 reported that whereas patients having the femoral component internally rotated relative to the epicondylar axis had patellofemoral complications such as lateral tracking, subluxation, dislocation, and patellar prosthesis failure, patients having the femoral component externally rotated relative to the epicondylar axis had no patellofemoral problems. In addition, Kawahara et al. 19 reported that the score of functional activities and the score of satisfaction decreased in patients with the femoral component internally rotated relative to the SEA. Given these study results, preventing the internal rotation of the femoral component is important.
Several studies showed that there are racial differences in knee joint obliquity and the anatomical structure of the distal femur. 8 –10,14 Some authors reported that femoral cutting with 5° external rotation relative to the PCA is better in Asian. 8,10
In this study, the femoral component was externally rotated by 1.1° relative to the SEA in the 3° external rotation group and by 1.8° in the 5° external rotation group although the difference was not statistically significant. Although the TEA is considered to be a useful reference axis for obtaining balanced flexion gaps, it includes the surgical TEA and the clinical or anatomic TEA, 15,21,22 and approximately 2–3° differences are reported between them. 1 Since there are still controversies over which of them are more optimal, 4,18,22 –25 it is difficult to evaluate which of the two groups has femoral components more appropriately located. There should be a 2° difference on average in FCR between the two groups theoretically but our study showed there was a difference of only 0.7° on average. This is considered attributable to the small number of cases, anatomical differences in the distal femur among individuals, and asymmetrical cartilage losses.
In our study, only one case (1.6%) in the 5° external rotation group showed internal rotation of the femoral component in relation to the surgical TEA, whereas five cases (9.4%) in the 3° external rotation group showed such internal rotation. This indicates that if the femoral component is externally rotated uniformly by 3° in relation to the PCA during TKA, the possibility of internal rotation of the femoral component in relation to the SEA may increase. In addition, there was no significant difference in PTAs and LPD evaluated based on Merchant views between the two groups. This is considered attributable to the fact that there was no significant difference in the rotational alignment of femoral component between the two groups.
The hypothesis that 5° external rotation of the femoral component would be better than 3° external rotation for FCR and patellar tracking taking into account racial anatomical differences in the distal femur has been dismissed. This is considered to be attributable to the fact that many factors such as anatomical differences among individuals, the degree of progress of osteoarthritis, and differences in the sites and amounts of cartilage loss affect the relationship between the reference axes of the femur. Although it is said to be advantageous to have 5° external rotation for Asian patients without posterior condyle wear, we concluded there is no need to adhere to 5° external rotation which might increase the risk of notching as there is no big difference in clinical results even when the degree is 3°.
This study has several limitations. First, this study was retrospective in design and included 115 knees of 598 patients, causing selection bias. Second, patellar tracking during deep flexion could not be accurately evaluated because patellar tracking was evaluated based on only Merchant views and clinical scores. In addition, statistically significant results could not be easily obtained because the number of study subjects was small and the calculation of sample size was not performed so we do not know about the statistical power.
Conclusions
No statistically significant difference in the patellar tracking between FCR by 3° and 5° could be demonstrated. We concluded there is no need to adhere to 5°external rotation as there is no statistical difference in clinical and radiological results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.