
Abstract
Background
Hong Kong Chinese exhibits a greater varus lower limb mechanical axis and coronal bowing when compared to Caucasians. This anatomical difference may affect the accuracy of bone cuts in total knee arthroplasty (TKA) using western anatomy-based intramedullary TKA cutting jigs. Use of computer navigation may avoid suboptimal cuts due to altered anatomy. This is the first study evaluating clinical function, radiological alignment and long-term survival of computer-assisted TKA amongst Hong Kong Chinese patients.
Methods
Retrospective study comparing articular surface mounting computer-assisted TKA (ASM-CATKA) and conventional TKA performed in a single centre from 2008 to 2010. Patients were followed up for assessment of clinical parameters including range of motion, Knee Society Knee score, and radiological parameters such as limb alignment, component alignment, and survival.
Results
Seventy-five patients were included in this study. Baseline clinical and radiological data were similar between groups. The computer-navigated group had superior radiological mechanical alignment (p < 0.001), tibial component alignment (p = 0.016) and femoral component alignment (p < 0.01) when compared to conventional TKA. There were no differences in knee scores (p = 0.488), range of motion (p = 0.432) and survival at 117 months (p = 0.986) between the two groups.
Conclusion
This retrospective study showed that ASM-CATKA was more accurate in achieving neutral mechanical axis and component alignment amongst Hong Kong Chinese. Clinical outcomes and implant survival were comparable.
Keywords
Introduction
Total knee arthroplasty (TKA) aims to restore limb alignment and achieve a neutral mechanical axis which passes from the centre of the hip, through the centre of the knee to the centre of the ankle. In a landmark study by Jeffrey in 1991 with a median follow-up of 8 years, it was shown that the rate of implant loosening was significantly lower when the postoperative mechanical axis was within 3° of neutral (3% loosening) when compared to knees outside this range (27% loosening). 1 In addition, coronal and axial plane malalignment of implants have been shown to result in less favourable clinical outcomes in terms of pain, stiffness, instability, and incidence of patellofemoral joint maltracking together with higher rates of revision.2–6 Several prospective studies favoured computer-assisted TKA over conventional total knee arthroplasty in terms of achieving superior coronal limb alignment.7–10 However, there were other studies which failed to show any clinical or radiological differences between the two groups.11–13
Hong Kong Chinese had different femoral and tibial osteology when compared to Caucasians with the medial inclination of the tibial plateau significantly greater in Hong Kong Chinese, and the mechanical axes of the limb in Hong Kong women were in significantly more varus when compared to Caucasians. 14 The clinical significance of such anatomical variations was that conventional intramedullary systems based on western osteology may not be accurate. As such, the use of computer-navigated systems on Hong Kong Chinese may avoid suboptimal bone cuts due to altered anatomy.
The current study aims to compare clinical, radiological and survival outcomes between articular surface mounting computer-assisted TKA (ASM CATKA) and conventional intramedullary-guided TKA in a single centre in Hong Kong with a follow-up of 10 years. It is hypothesized that the use of computer-assisted TKA, when compared to conventional techniques would result in better implant component alignment and restoration of limb mechanical axis which ultimately would lead to improved functional outcomes and implant survival. With regards to the published literature, this is the first study evaluating long-term survival outcomes of ASM CATKA amongst Hong Kong Chinese patients.
Methods
All Hong Kong Chinese patients who underwent TKA with the Triathlon Total Knee System (Stryker) in a district hospital in Hong Kong from January 2008 to December 2010 were included. Exclusion criteria included revision procedure for septic or aseptic loosening, TKA performed for intraarticular fractures, TKA with varus-valgus constrained implant or rotating hinge implants, or bilateral procedures. The Triathlon Total Knee System was chosen in this study because it supported both navigated and conventional techniques. Computer navigation used was Stryker Articular Surface Mounting (ASM) technology, which was an image-less navigation system which only required intraoperative registration of anatomical landmarks without the need of preoperative CT images.
On the contrary, conventional TKA involved the use of cutting jigs attached to intramedullary and extramedullary guides for distal femur and proximal tibia resections, respectively. The aim was to achieve a bone cut perpendicular to the mechanical axes of the femur and tibia. The entry site of the femoral IM guide was 1 cm anterior to the femoral attachment of the posterior cruciate ligament and slightly medial to the mid-line of the distal femur. The 5/16” Triathlon IM guide was inserted into the femoral canal and set to a 5°/ 6°/7° valgus cut angle. The valgus cut angle was determined by calculating the difference between the anatomical and mechanical femoral axes on standing lower limb long film. Extramedullary proximal tibia resection guide was utilized to achieve a cut perpendicular to the mechanical axis of the tibia.
All patients received cemented posterior stabilized prosthesis and patellar resurfacing. Patients were followed-up at postop 2 weeks for wound status, 1 month for lower limb weight-bearing long film and 3 months for knee scores. Afterwards, patients were followed at 6 months and then yearly with standing radiographs of the knees.
Bias is minimized by standardizing the technique of surgery with selective patella resurfacing for both groups, same implant model was used, and all operations were performed by specialists.
Outcome measures
Clinical parameters obtained included knee range of motion and Knee Society Score (KSS). Radiological parameters included limb alignment angle, coronal femoral component angle and coronal tibial component angles (Figure 1) on standing radiographs. The limb alignment angle was calculated by the angle subtended by the coronal mechanical axes of the femur and tibia at maximal extension. Preoperatively, the mechanical axis of the femur was defined as the line joining the centre of the femoral head and the intercondylar notch of the femur; the mechanical axis of the tibia was defined as the line joining the midpoint of the two tibial eminences and the dome of the talus. Postoperatively, the mechanical axis of the femur was defined as the line joining the centre of the femoral head and the centre of the femoral component; the mechanical axis of the tibia was defined as the line joining the midpoint of the tibial component and the centre of the dome of the talus. Ideal alignment of limb alignment angle was taken to be 180°. Coronal femoral and tibia component angles were calculated using an angle subtended between a line through the articulating surface of the component and the mechanical axis of the limb in the coronal plane. Ideal alignment was taken as the component being perpendicular to the mechanical axis of the limb, that is, 90°. All XR measurements were taken with varus specified as positive, in line with Berend et al. 2 who specified that +3° of varus alignment was shown to increase the odds of failure. Valgus was labelled as negative.
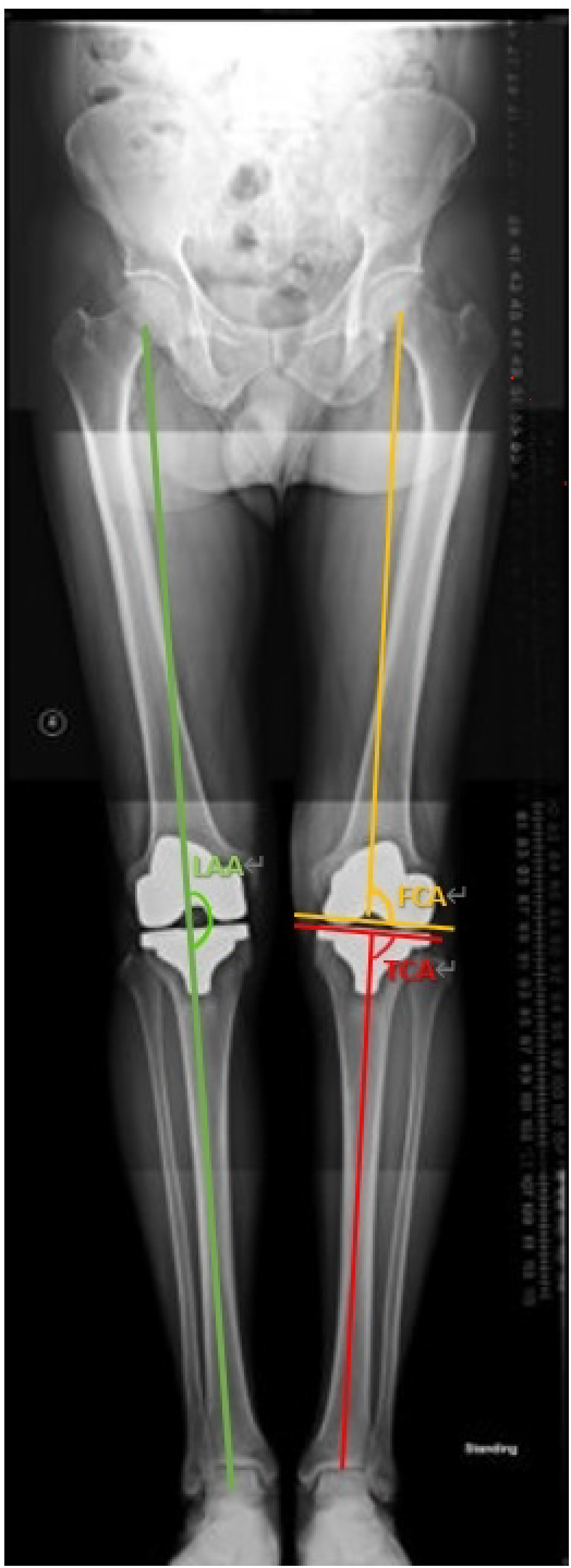
Limb alignment angle (green). Femoral component angle (yellow). Tibial component angle (red).
Study size calculation
Prestudy power analysis was used to calculate an appropriate sample size using an alpha value (probability of type 1 error) of 0.05 and beta value (probability of type 2 error) of 0.2. Based on data regarding allowable difference and population variance from a previous study of computer-navigated TKA amongst Hong Kong Chinese, 15 a significant difference in mechanical alignment can be detected with a sample size n = 52.
Statistical analyses
All analyses were conducted with Statistical Package for the Social Sciences (SPSS Inc, Chicago, IL, USA). Basic data were presented as the mean ± SD for continuous variables and as percentages for categorical variables. Tests for data normality were performed for continuous data. Independent sample t-test or Mann–Whitney U test was used to compare continuous variables between computer-navigated group and conventional TKA group. Chi-square test or Fisher's exact test was used to compare categorical variables between the two groups. Kaplan–Meier survival analysis was used to determine implant survival for the two groups. Log-rank test was used to calculate any significant differences in implant survival. A p-value of <0.05 was considered statistically significant, and all tests were two-tailed.
Results
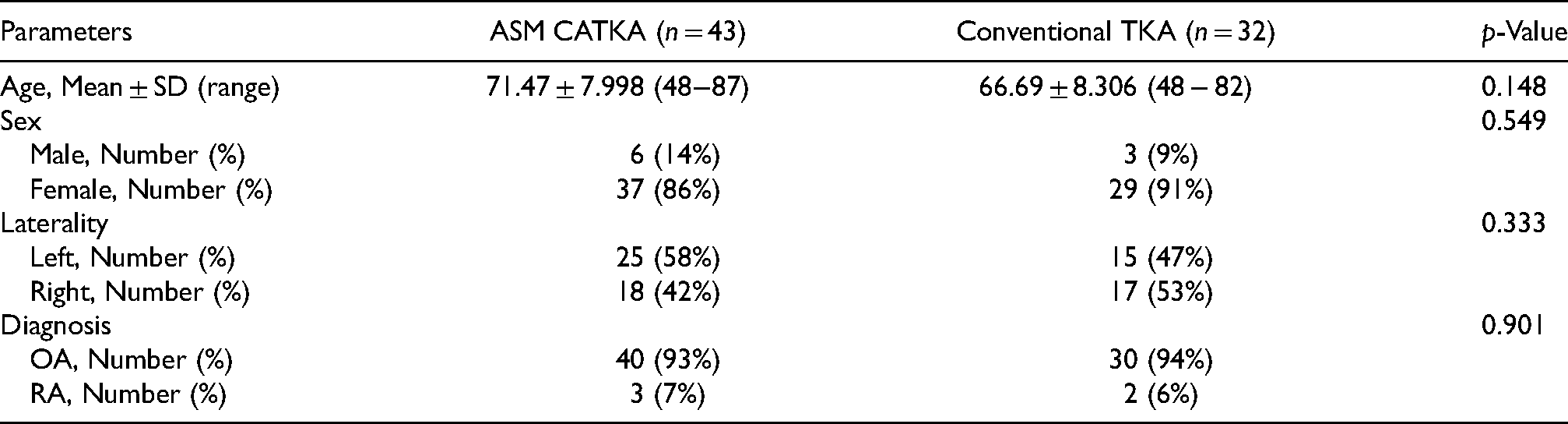
Seventy-five TKAs were performed using Triathlon Total Knee System within the period from 2008 to 2010. Forty-three underwent ASM computer navigation and 32 underwent conventional TKA with intramedullary femoral and extramedullary tibial cutting guides. Baseline characteristics are summarized in Table 1. There were no baseline differences between groups in age, sex, laterality of operation and preoperative diagnosis. There were no baseline differences in clinical parameters between the ASM group and the conventional group, detailed in Table 2.
Baseline characteristics.
Preoperative clinical parameters.

Clinical outcomes
Postoperative data are shown in Table 3. Postoperative range of motion of the ASM group and conventional TKA group were 95.98 ± 7.68 and 97.5 ± 8.52° (Mean, SD), respectively. There was no statistically significant difference (p = 0.432) between the groups. Postoperative knee society knee scores of the ASM group and conventional TKA were 86.23 ± 5.35 and 85.38 ± 5.17, respectively; there was no statistically significant difference between the groups (p = 0.488). Postoperative knee society functional scores of the ASM group and conventional TKA group were 63.26 ± 8.44 and 59.69 ± 8.32, respectively; there was no statistically significant difference between groups (p = 0.073).
Postoperative clinical parameters.

Radiological outcomes
The ASM navigation group achieved postoperative mean limb alignment of 0.93 ± 2.03° while the conventional group had a mean postoperative limb alignment of 2.81 ± 1.77°. This difference was statistically significant (p < 0.001). The ASM navigation group had postoperative mean coronal femoral component angle of 1.05 ± 1.80° while the conventional group had a mean coronal femoral component angle of 2.16 ± 1.48°. This difference was also statistically significant (p < 0.01). The ASM navigation group achieved postoperative mean tibial coronal component angle of 1.05 ± 1.40° while the conventional group had a mean tibial coronal component angle of 2.06 ± 1.97°. This difference was statistically significant (p = 0.016). Overall, the results revealed a significant difference between the two groups in favour of knees undergoing ASM computer navigation. The radiological results were shown in Table 4.
Radiological parameters.
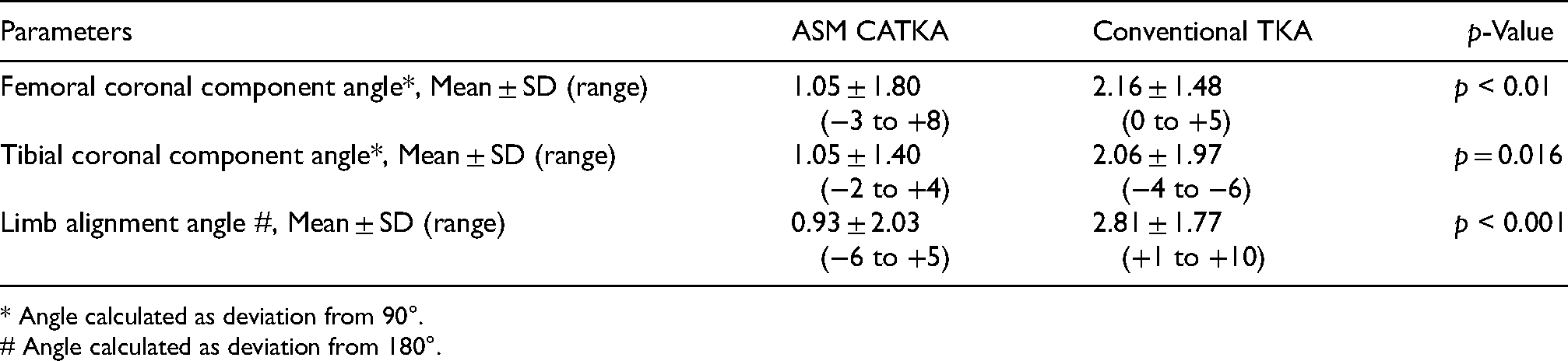
* Angle calculated as deviation from 90°.
# Angle calculated as deviation from 180°.
Survivorship
The median follow-up in this study was 117 months. The median follow-up duration for the ASM navigation group was 113.3 months and the conventional group was 126 months. There was no statistically significant difference in duration of follow-up between the two groups (p = 0.986). A total of two revision TKAs were performed, and they both occurred in patients receiving ASM computer navigation. Both cases were revised due to infection. One case occurred 18 months after the index operation and the other case occurred 41 months after the index operation. There were no revision knee arthroplasties performed for the conventional group. There were no revisions performed for wear or aseptic loosening. The survival rate for the ASM group was 95%, and the conventional group was 100%. Log-rank test showed that there was no statistically significant difference regarding survival between the two groups (p = 0.311).
Discussion
The current study showed that ASM navigated total knee resulted in superior postoperative mechanical limb alignment, and better coronal tibial and femoral component alignments when compared to conventional methods. Despite the superior radiological results, there were no significant differences in terms of ROM, KSS and implant survivorship at more than 9 years. This study represented the first study to evaluate TKA long-term survival using computer navigation amongst Hong Kong Chinese, a group which is unique with more angulated and bowed lower limbs when compared to Caucasians14, 16 and established the efficacy of computer navigation in achieving satisfactory radiological alignment in such patients.
This study echoed that of Decking et al. who showed that significantly more patients with computer navigation system achieved the desired postoperative straight mechanical axis when compared to conventional methods. 8 The current study employed the Stryker ASM navigation system and concurred with the study by Sparmann et al. who showed that Stryker ASM navigation significantly improved the postoperative mechanical limb axis, and the coronal axis of femoral and tibial components 9 when compared to conventional techniques. While the superiority of computer navigation in terms of alignment was well established in the literature, whether such better alignment translated into better functional or clinical outcomes remained controversial. In 2007, the meta-analysis by Bauwens et al. 17 could not conclude whether there were any significant differences in functional results between navigated knees and conventional knees. More recently in 2018, a randomized controlled study by Kim et al. 18 with 12 years of follow-up did not show any clinical differences in patients who received bilateral TKA with one side navigated and the other side conventionally performed.
In the current study, there was no significant survival difference between ASM navigated knees and conventional knees at more than 9 years. At the beginning of this study, it was hypothesized that ASM-navigated knees would have better survival due to less aseptic loosening and wear due to an improved postoperative alignment. This assumption was based on previous studies which showed that malalignment resulted in loosening and early failure.1,2,4 Moreover, in a recent United States Medicare registry study, 19 it was shown that patients who were less than 65 years of age and received computer navigation had lower risk of 5-year revision when compared to conventional techniques. However, the current study suggested otherwise: a finding supported by the study by Parratte et al. 20 in 2010 which showed that there were no 15-year survival differences between knees within and out of the postoperative mechanical alignment of ±3°. The conflicting results in the literature could be because registry studies better reflect the average performance of various surgeons in different centres, thus better reflecting the benefit of computer navigation while centre-based studies reflected expertise in high-volume centres and were not generalizable.
Limitations
There were several limitations to this study. This was a retrospective review of patients undergoing TKA using computer-navigated and conventional methods. The decision to perform navigated or conventional TKA was completely arbitrary and subject to the operating surgeon's choice. Whether the operating surgeon may tend to choose navigation for seemingly more difficult knees was uncertain. In addition, for patients with excess lateral bowing receiving conventional intramedullary guide TKA, the instrumentation was unable to produce a valgus cut angle of more than 7° and would result in a residual varus cut. This would produce an unfavourable postoperative varus coronal femoral component angle and limb alignment angle. Furthermore, this study included navigated TKA cases which were performed early after the first introduction of this system into the hospital. Surgeons may not be entirely familiar with this system, which may be unfavourable to perioperative outcomes including operating time. Lastly, although there were long-term data regarding survival, there were no objective knee score assessments upon long-term follow-up.
Conclusion
In conclusion, this was the first study evaluating clinical outcomes, radiological alignment as well as the long-term survival of computer-navigated TKA in Hong Kong Chinese patients. This study established that computer navigation with articular surface mounting technology was more accurate in achieving neutral mechanical axes when compared to a conventional intramedullary guide. Clinical outcomes and implant survival were similar between patients with computer-navigated TKA and conventional TKA. In the future, prospective studies with the inclusion of patients with significant preoperative deformity could be undertaken to compare the two methods.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article