
Abstract
Purpose:
To find out the factors suggesting lumbar segmental instability in patients with degenerative spondylolisthesis (DS) on conventional magnetic resonance imaging (MRI).
Methods:
Ninety-four patients with DS who underwent decompression surgery with or without fusion were selected. Patient demographics and findings on simple radiographs and MRI were analyzed. We divided patients into two groups by the presence of lumbar instability on simple standing plain radiographs and measured degeneration status of intervertebral discs and facet joints and distance of facet fluid signal on T2 axial MRI on each groups. The data were analyzed to find out the correlation between facet fluid signal and lumbar instability.
Results:
Sixty-three patients were confirmed to have lumbar instability (unstable group (UG), 67%), while 31 patients (stable group (SG), 33%) did not have instability on simple radiographs. The mean age was slightly older in SG (p < 0.05) and SG patients’ degeneration status of intervertebral discs and facet joints was advanced than UG patients. Fifty-five of 63 patients had high signal intensity on T2-weighted MR images in the UG, but only 4 of 31 patients had high signal intensity in the SG (p < 0.001) and UG patients have more larger facet joint distance than SG patients (p < 0.001).
Conclusion:
High signal in facet joints on T2 MR images can be a useful factor suggestive of lumbar instability. Thus, the identification of fluid signal in the facet joints on MRI should raise the suspicion for lumbar instability and prompt additional evaluations such as with stress radiographs.
Introduction
Lumbar degenerative spondylolisthesis (DS) is defined as the excessive translation of one vertebra over another due to degenerative change of supporting structures. 1 –5 DS is a degenerative disease that particularly affects the elderly. The importance of diagnosing and treating DS is increasing in an aging society. Theoretically, DS can develop in any segment of the spine, but most commonly involves L4/5, which may be due to the high degree of motion in this segment. 6,7
Lumbar segmental instability is an abnormal motion to physiologic loads, characterized by greater than normal range of motion. 8 –11 Recently, many studies have shown that intervertebral disc and facet joint degeneration are related with spinal instability. 12 –14 Mechanical Instability caused by degenerative changes in these structures can cause clinical symptoms such as low back pain or radiculopathy, in addition to various chemicals caused by disc or facet joint degeneration. 15,16 When these clinical symptoms are very severe, various surgical treatments can be considered, including segmental fusion in the setting of obvious segmental instability. Many authors including Herkowitz et al. have suggested that fusion surgery should be performed when lumbar spinal instability exists and have shown better outcomes for lumbar stability with spine fusion surgery than with decompression alone. 17 –19 Thus, it is important to determine the presence of lumbar instability because it can change the treatment plan and patient prognosis.
Standing lateral flexion–extension radiographs have been used as the gold standard for the diagnosis of lumbar instability. 20,21 However, magnetic resonance imaging (MRI) is almost routinely used to assess for the diagnosis of lumbar disease in elderly patients recently. 22 There have been a few studies assessing the usefulness of MRI for the detection of lumbar instability with stenosis, which may be due to the supine position resulting in vertebra repositioning with conventional MRI. In addition, various findings such as intervertebral disc herniation and ligament flavum hypertrophy may not be detected on supine images compared to images taken in the standing position. 23 –25 There are some imaging techniques that have been proposed to overcome this problem such as dynamic or weight-bearing MRI, 26,27 although their usefulness is limited to specific circumstances. Thus, it is important to determine the factors associated with spinal instability on conventional MR images.
In this study, we attempted to determine the factors visible on conventional MR images that are suggestive of lumbar segmental instability.
Materials and methods
All patients with DS who underwent decompression surgery with or without fusion in our hospital were retrospectively reviewed. Patients who had multilevel lumbar disease, other lumbar disease (e.g. infection, tumor-related conditions, and traumatic lesions), and who had previous lumbar surgery were excluded. Using this criteria, a total of 94 patients with DS were included in this study. These groups were analyzed for (1) age, (2) gender, (3) involved spinal level, (4) disc degeneration grade, (5) facet degeneration grade, and (6) the presence of a fluid signal.
The patients’ MRIs and simple standing plain radiographs (L-spine anterior–posterior, lateral, flexion, and extension view) were analyzed. Translation greater than 5 mm or changes in angulation greater than 10° on the lateral flexion and extension standing radiographs were considered to show segmental instability (Figure 1). 28 –31 Using these criteria, the study group was divided into UG and SG.
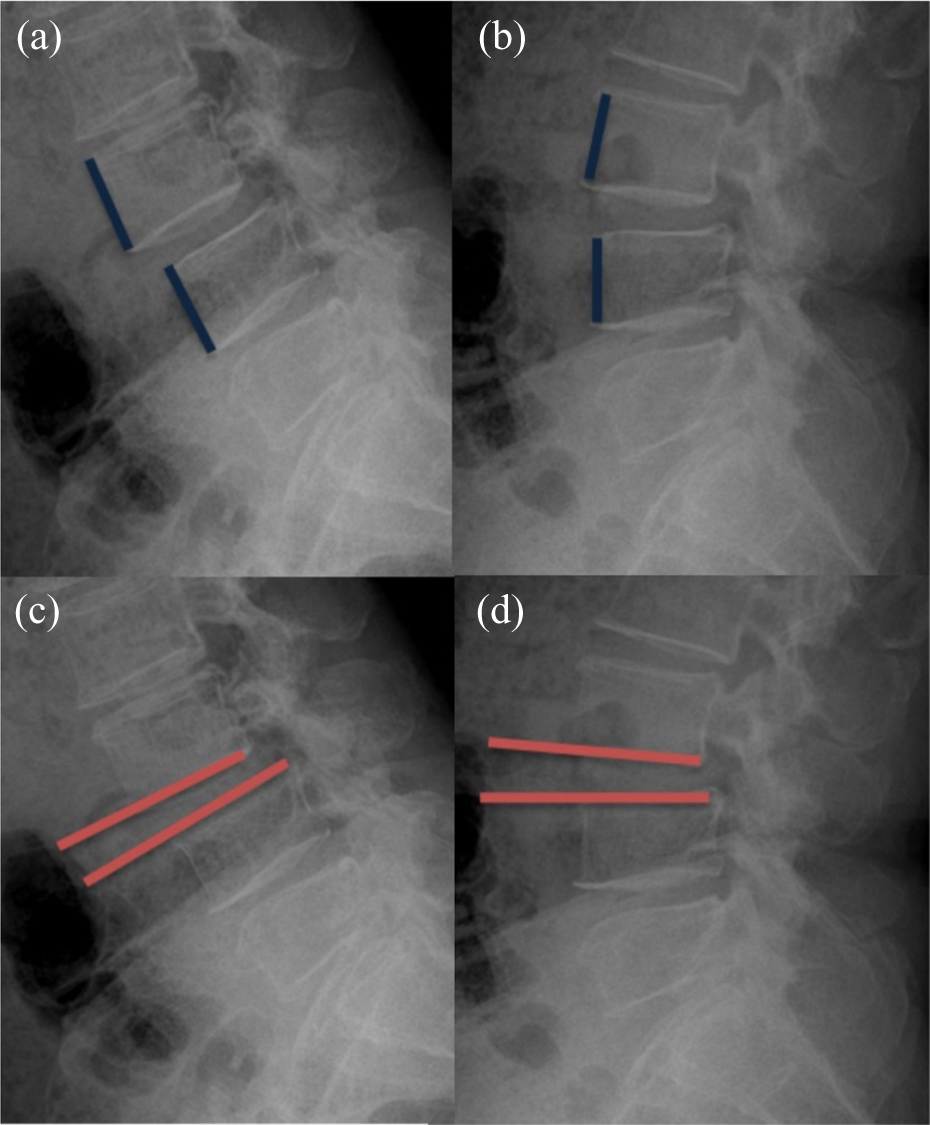
Translation greater than 5 mm (a and b) or changes in angulation greater than 10° (c and d) on the lateral flexion and extension.
Magnetic resonance sagittal and axial T2-weighted images were reviewed. All images were acquired on 1.5 Tesla Siemens MR machines. The MR images were evaluated to grade the degree of degeneration of the intervertebral disc and facet joints, the changes in signal, and the widening of the facet joint. Disc degeneration was divided into five grades using the Thompson criteria, 32,33 and facet joint arthritis was calculated by the sum of Grogan’s score. 32,34 We assessed for the presence of fluid signal in the facet joints on the axial T2-weighted images, as defined as high signal on the T2-weighted images. Facet joint distance was also measured by the largest value of perpendicular line to the facet joint (Figure 2). Each side of the facets (i.e. right or left) was independently reviewed.

Fluid signals in the facet joints on the axial T2-weighted images. Facet joint distance was also measured by largest value of perpendicular line to the facet joint (a) case with widened facet joint, (b) case with narrowed facet joint.
All measurements were carried out using computer-based digital radiographs on a picture-archiving computer system (PiViewSTAR; Infinitt, Seoul, Korea). Three well-trained orthopedic surgeons each measured the various parameters twice, with the second measurement performed 2 weeks after the first measurement. The interobserver and intra-observer differences were very low.
Statistical analyses
The mean and standard deviation of the demographic data of all patients was calculated. Statistical analyses were performed with SPSS (Windows, Version 15.0). Pearson’s correlation coefficient was calculated to analyze the association between facet fluid signal and lumbar instability. For all statistical comparisons, p-values <0.05 were considered statistically significant.
Results
Demographic results
The average age of the 94 patients was 63.8 years (63.8 ± 10.3). There were 41 men and 53 women (Table 1). The most commonly involved level was L4/5 (65 cases, 69%), followed by L3/4 (14 cases, 15%), L5/S1 (12 cases, 13%), and L2/3 (3 cases, 3%).
Demographic results.

Comparative results of the demographics and plain radiographs in patients
Sixty-three patients were confirmed to have DS with instability on simple lateral flexion–extension radiographs (UG, 63 cases, 67%), while 31 patients did not have instability on simple lateral flexion–extension radiographs (SG, 31 cases, 33%) (Table 1).
The mean age in the UG was 62.2 ± 9.4, while the mean age in the SG was 65.3 ± 10.9 (p < 0.05). No statistically significant differences were noted in the gender composition between the two groups. The average length of anterior translation on plain films was 6.9 ± 2.1 in the UG and 1.9 ± 1.2 in the SG. The average angulation was 7.8 ± 3.5 and 4.6 ± 2.3 in the UG and SG, respectively (Table 2).
Comparative results of the demographics and plain radiographs in patients.

Ns: not significant.
Comparative results of the MRI findings in patients
The mean disc degeneration grade according to the Thompson grade system was 3.0 ± 0.77 in the UG and 3.96 ± 0.88 in the SG (p < 0.05). The mean facet degeneration score (calculated by the sum of Grogan’s scores) was 4.94 ± 2.23 and 9.32 ± 1.83, respectively (p < 0.001). Fifty-five of 63 patients had high signal intensity on T2-weighted MR images in the UG, but only 4 of 31 patients had high signal intensity in the SG (p < 0.001). The mean facet joint distance was 1.68 ± 0.74 in the UG and 0.81 ± 0.4 in the SG (Table 3, p < 0.001). Of total 63 patients in the UG, 48 patients (76%) had over 1 mm of facet distance on MRI, but only 3 patients in the SG (10%, 3/31) had over 1 mm of facet distance. Forty-six patients (73%, 46/63) had combination of high signal intensity on facet joints and larger facet distance than 1 mm in UG (Figure 3).
Comparative results of MRI findings in patients.

MRI: magnetic resonance imaging.
aThompson grade of disc degeneration on MRI.
bSum of Grogan’s score of facet degeneration on MRI.

Of total 63 patients in the UG, 48 patients (76%) had over 1 mm of facet distance on MRI, but only three patients in the SG (10%, 3/31) had over 1 mm of facet distance. Forty-six patients (73%, 46/63) had combination of high signal intensity on facet joints and larger facet distance than 1 mm in UG. UG: unstable group; SG: stable group; MRI: magnetic resonance imaging.
Discussion
This study shows a positive association between the presence of lumbar facet fluid signal on conventional MRI and the presence of segmental instability detected on the simple lateral flexion–extension radiograph. The facet fluid signal on MRI is a factor indicating lumbar instability with a relatively high positive predictive value (93.22%). Thus, a MRI showing facet fluid signal should raise the suspicion for lumbar instability. However, MRI alone is insufficient for the diagnosis of lumbar instability as 17% (8/63) of patients who have instability on simple lateral radiograph did not have fluid signal on MRI and 7% (4/59) patients who had a facet fluid signal on MRI did not have instability on simple lateral radiograph in our study. So all findings on simple radiographs and MRI should be considered when making the diagnosis of lumbar instability.
Our study also shows that the mean disc degeneration and facet joint degeneration was higher in the SG than the UG. The intervertebral disc and facet joints are important to maintain lumbar stability. In a study by Fujisawa et al., the greatest amount of motion was observed with axial rotation, flexion, and extension in patients with grade IV degenerative discs and with lateral bending in patients with grade III degenerative discs. 32 Motion was decreased in patients with grade V degenerative discs. 32 In addition, facet joint mobility was increased in patients with grade III cartilage degeneration and decreased in patients with grade IV cartilage degeneration due to subchondral sclerosis. 32 Kirkaldy-Willis et al. divided the process of lumbar degeneration into three phases: dysfunction, instability, and stabilization. 35 During the first phase, affected segments of lumbar spine do not function normally, but anatomical changes are minimal. In the second phase, reduced disc height, loosened facet capsules and ligaments, and degenerated articular changes are observed, resulting in instability. In the final phase, fibrosis around facet joints and osteophytes produce stiffness and restabilization. 35 Chaput et al. said as the degenerative process passes from the dysfunction phase to the stabilization phase, facet joint effusions should be decreased. 36 Our study supports this hypothesis as the UG had relatively milder disc degeneration and facet joint degeneration than the SG.
Lumbar instability could be an important indication for spine fusion surgery because decompression surgery alone could cause more severe instability. There have only been a few studies evaluating the relationship between lumbar instability and facet fluid signal on MRI. Chaput et al. found that a clinically measurable facet effusion (≥1 mm) suggests the need for simple lateral flexion extension radiograph to diagnose lumbar instability. 36 According to Rihn et al., there is a close association between the facet fluid signal on MRI and the amount of instability at L4/5 on plain radiographs. 37 However, their studies were limited to only the L4/5 segment. One of the strengths of our study is that it includes other lumbar segments beyond L4/5. In addition, this is the first study demonstrating the relationship between lumbar facet fluid and segmental instability in Asian patients. One of the limitations of our study is its retrospective design. However, this study identified risk factors suggestive of lumbar instability on conventional supine MRI.
Conclusion
High signal in facet joints on T2 MR images can be a useful factor suggestive of lumbar instability. Thus, the identification of fluid signal in the facet joints on MRI should raise the suspicion for lumbar instability and prompt additional evaluations such as with stress radiographs.
Footnotes
Author contributions
All authors took part in writing the manuscript, and all agreed to accept equal responsibility for the accuracy of the content of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant from the Korea University R&D project (K1132311).