
Abstract
Study Design
Retrospective study.
Objective
The objective of this study is to investigate the association of waterpipe smoking with lumbar intervertebral disc degeneration (IVDD).
Methods
This is a retrospective chart review study. A total of 286 adults who underwent a lumbar magnetic resonance imaging (MRI) at a tertiary medical center were included and divided into three groups. Group 1 (n = 125) included non-smokers, group 2 (n = 80) smoked cigarettes only, and group 3 (n = 81) smoked waterpipe only. The intervertebral discs were graded using the Pfirmann disc degeneration grading system.
Results
The study showed higher lumbar disc degeneration scores for waterpipe and cigarette smokers compared to non-smokers at all spinal levels. Specifically, post hoc analysis showed that there was a significant difference at L1-L2 between cigarette smokers and non-smokers (P = 0.007) and between waterpipe smokers and non-smokers (P = 0.013), and a significant difference at L3-L4 and L4-L5 between non-smokers and cigarettes smokers (P < .001 and P = .029 respectively).
Conclusion
Waterpipe smoking is associated with lumbar intervertebral disc degeneration.
Keywords
Introduction
Intervertebral degenerative disc diseases of the lumbar spine are chronic diseases relatively common in occurrence.1,2 Different risk factors for intervertebral disc degeneration (IVDD) have been identified, varying according to the population studied. Large epidemiologic studies have shown cigarette smoking to be an independent risk for developing IVDD.3-5 In fact, the regulation of genes critical for the spine integrity is altered by cigarettes components. 1 On the other hand, nicotine promotes vasoconstriction which hinders the peripheral perfusion and damages the intervertebral discs. 6 Other toxic chemicals produce reactive oxygen species that promote atherosclerotic plaques formation.
Waterpipe smoking, also known as hubble bubble, hookah, narghile, argile, shisha or hookah, is a traditional form of smoking that originated in India. 7 It has become popular worldwide, including in the Eastern Mediterranean countries. For example, Lebanon has a high prevalence of waterpipe smoking reaching 32.7% among males and 46.2% among females.8,9 Waterpipe smoking is falsely considered less addictive and less harmful when compared to cigarette smoking despite increasing evidence showing the opposite. Similar to cigarettes, waterpipe smoke contains oxidants, carbon monoxide, nicotine, and other harmful substances, some of which is contributed to by the burning charcoal that lights the waterpipe. A number of health hazards have been associated with waterpipe smoking and these include cardiovascular, respiratory and other health effects. 8 One study of contributing factors to low back pain in Qatar recognized a significant association with cigarette or waterpipe smoking. 10 However, the effect of waterpipe on IVDD was not thoroughly assessed in this study. 10
To our knowledge, no studies have addressed the association between waterpipe smoking alone and IVDD. In the present study, we investigated this association of both waterpipe and cigarette smoking with the radiologic findings of IVDD on spine Magnetic Resonance Imaging (MRI).
Materials and Methods
Informed Consent
The study was exempt from informed consent by the Institutional Review Board (IRB) which granted a waiver of informed consent since the study consisted of analysis of deidentified data and didn’t pose greater than minimal risk to subjects.
Study Design
The study was conducted at the American University of Beirut Medical Center (AUBMC) between Nov 2018 and Nov 2019. The medical records of all patients who underwent a lumbar spine MRI at AUBMC during this period were reviewed. The data collected included age, gender, smoking status (Yes/No, cigarettes/waterpipe), weight, height, medical history, surgical history and problem list.
Only patients who were 18 years or older were included in the study. Patients with any history of diabetes, hypertension, coronary artery disease, rheumatologic disease, osteoporosis, spine tumors or prior spine procedures were excluded from the study since these health conditions were found to increase the risk of intravertebral disc degeneration.11-13 Patients who smoke cigarettes and waterpipe concurrently were excluded from the study.
Sample Size
In the absence of studies assessing changes in the degeneration of the intervertebral disc grades between non-smokers and waterpipe smokers, an effect size of 0.25 was assumed. Using a confidence interval of 0.95, α of 0.05, and a power of 80%, the minimum required sample size was 269.
A total of 286 patients were randomly selected from those who met the inclusion criteria mentioned above. They were divided into three groups. Group 1 (n = 125) included non-smokers, group 2 (n = 80) smoked cigarettes only, and group 3 (n = 81) smoked water -pipe only.
Ethical Approval: IRB approval number BIO-2020-0137
Approval for this study was obtained from the IRB at the American University of Beirut (IRB ID: BIO-2020-0137). Anonymity and confidentiality were maintained by not including the names of the patients or any other identifiers in the dataset. The results were analyzed and reported in aggregate form.
Imaging and Assessment
The lumbar MRI studies were performed using the 1.5 T Philips Ingenia device. Images through the lumbar intervertebral discs were obtained in the sagittal plane as turbo spin-echo T2-weighted acquisitions (time-to-repetition TR ms/time-to-echo TE ms: 2948/100, field-of-view FOV 160 × 295 mm and matrix 256 × 304 mm; 4-mm slice thickness and 1-mm intersection gap, for a total of about 15 sagittal images).
A radiologist and a senior radiology resident independently evaluated and graded the 286 MRI cases, including sequences of standard T2-weighted turbo spin-echo sagittal images. Both were blinded to the smoking status of the participants. About 10 % of the randomized sample read by the radiologist was re-read by the radiology resident (20 out of 199 cases) and 10% of the randomized sample read by the radiology resident was re-read by the radiologist (9 out of 87 cases). The intervertebral discs were graded using the Pfirmann disc degeneration grading system (grades 1-5); higher grades indicate more severe degeneration of the intervertebral disc. The Pfirrmann disc degeneration grading system ranges from Grade 1 to Grade 5, reflecting increasing severity of disc degeneration. Grade 1 represents a normal disc with a clear shape, no horizontal bands, and a distinct nucleus and annulus. Grade 2 shows a nonhomogeneous disc shape with horizontal bands and some blurring between the nucleus and annulus. Grade 3 has further nonhomogeneity with more pronounced blurring, though the annulus shape is still recognizable. Grade 4 indicates advanced degeneration with a nonhomogeneous shape, reduced signal intensity, an indistinct nucleus and annulus, and usually decreased disc height. Grade 5 is the most severe, similar to Grade 4 but with a collapsed disc space. 14
Statistical Analysis
Data were analyzed with SPSS version 27. Continuous variables are reported as mean ± standard deviation and categorical variables are presented as numbers and percentages. One way analysis of covariance (ANCOVA) was performed to compare the Pfirmann scores at different disc levels among non-smokers, cigarette smokers, and waterpipe smokers, with age and gender adjustments. Adjustment for the body mass index (BMI) was not done because of missing data. Post-hoc Bonferroni tests were performed for pair-wise comparison of Pfirmann scores among smoking categories. A P-value less than 0.05 was considered statistically significant.
Results
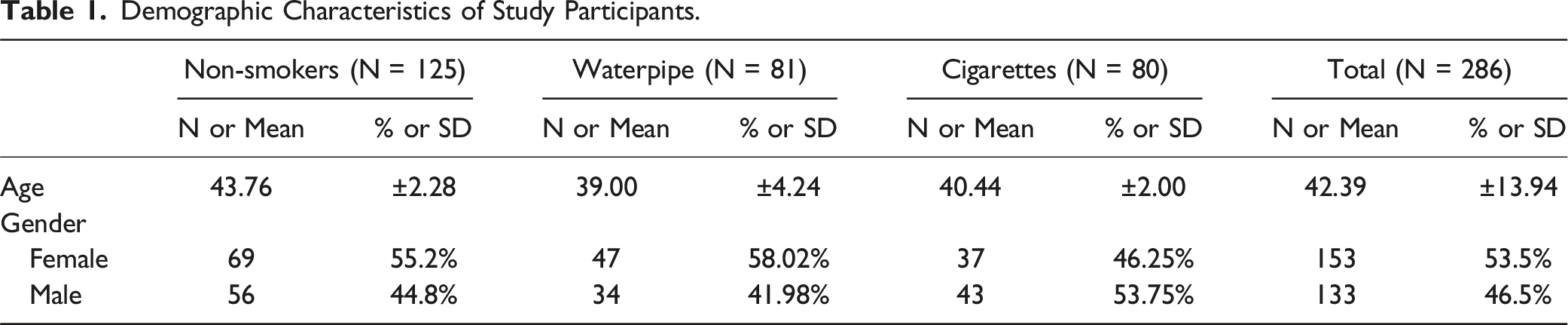
Demographic Characteristics of Study Participants.
Comparison of Pfirmann Scores at Different Levels Between Non-smokers, Waterpipe Smokers, and Cigarette Smoker Adjusted According to Age and Gender.
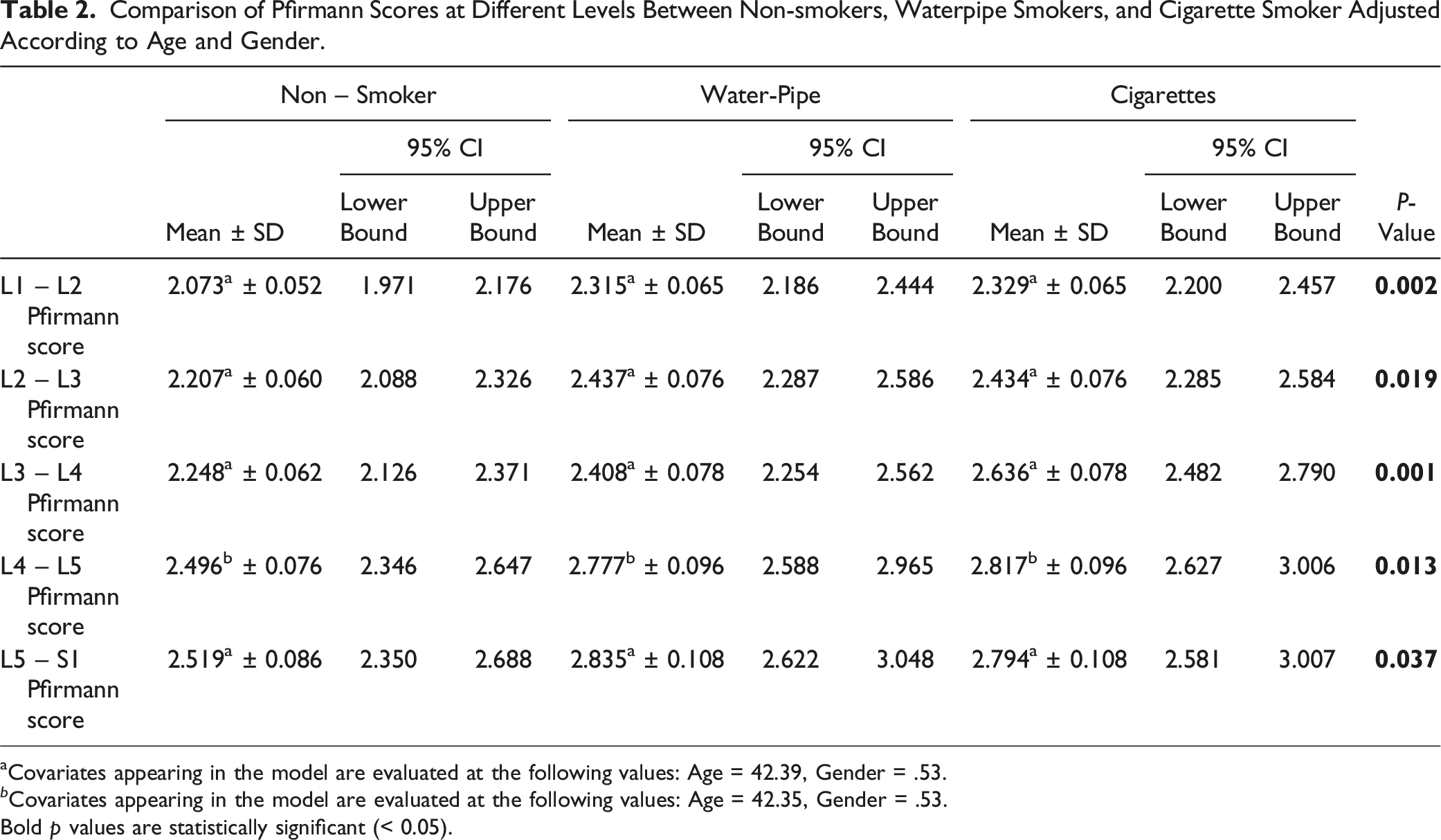
aCovariates appearing in the model are evaluated at the following values: Age = 42.39, Gender = .53.
b Covariates appearing in the model are evaluated at the following values: Age = 42.35, Gender = .53.
Bold p values are statistically significant (< 0.05).
With lower spinal levels, the means of the Pfirmann scores for all smoking categories increased, with the highest recorded score at L5-S1 level (2.519 ± 0.086 for non-smokers, 2.835 ± 0.108 for waterpipe smokes, and 2.794 ± 0.108 for cigarette smokers).
Bonferroni Pair-wise Comparison of Pfirmann Mean Scores Between Cigarette Smoker, Waterpipe Smokers, and Non-Smokers.
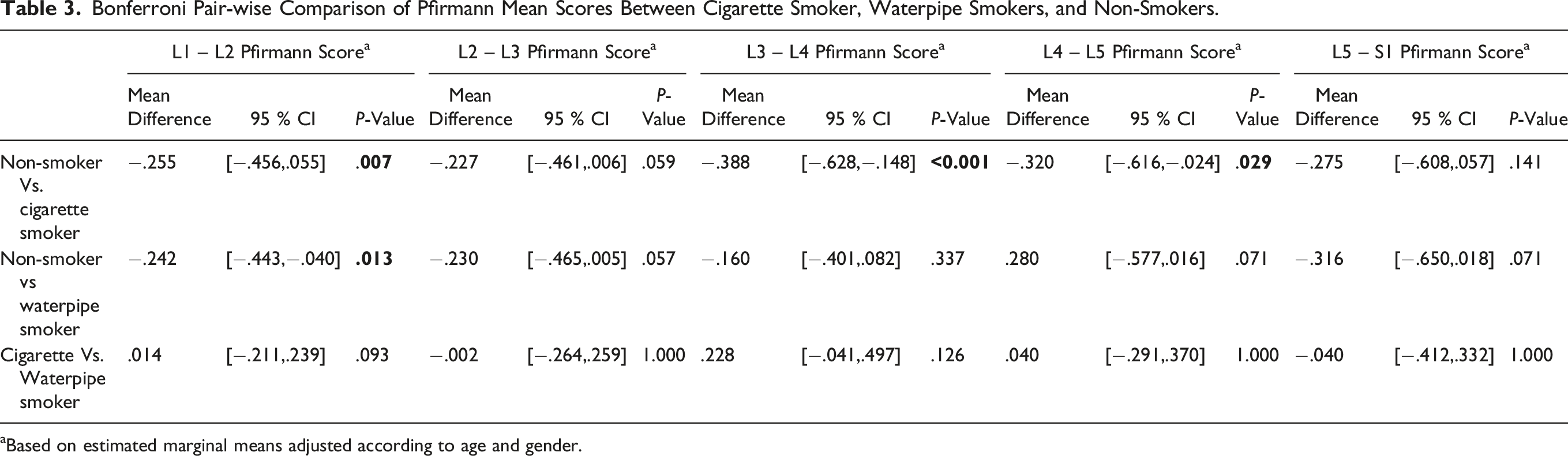
aBased on estimated marginal means adjusted according to age and gender.
Discussion
The study findings showed that the mean Pfirmann scores are significantly different among non-smokers, cigarette smokers, and waterpipe smokers, with higher lumbar disc degeneration scores for waterpipe and cigarette smokers compared to non-smokers. Specifically, after age and gender adjustment, there was a significant difference in the mean Pfirmnan scores at Levels L1-L2 between cigarette smokers and non-smokers and between waterpipe smokers and non-smokers, and a significant difference at L3-L4 and L4-L5 Pfirmann mean score between non-smokers and cigarettes smokers.
Cigarette smoking was found to be significantly associated with higher lumbar disc degeneration scores compared to non-smokers. The latter finding is consistent with the results of previous studies showing that lumbar disc degeneration increased significantly with cigarette smoking.4,15 The study by Chen et al also showed that the impact of smoking on the lower cervical discs is greater than the upper cervical discs, in line with our results, where the means of the Pfirmann scores for all smoking categories increased as we descend among the spinal levels. 16 Another study assessing the role of nicotine on the pathogenesis of disc degeneration showed an overall detrimental effect on disc cells through inhibition of cell proliferation and extracellular matrix synthesis. 17
Our findings showed a significant association between waterpipe smoking and disc degeneration. Waterpipe smoking is another form of tobacco use that is falsely believed to have no or less harmful effects on health despite producing high levels of nicotine. Compared to cigarette smoking, waterpipe usage is linked to higher carbon monoxide levels, similar nicotine levels, and significantly more smoke exposure. 18 Consequently, both tobacco-smoking practices are likely to share relatively similar health hazards. Multiple studies have demonstrated the hazardous consequences of waterpipe smoking, however most of those studies discussed the potential adverse effects on the cardiovascular and respiratory system as well as the risk of cancer development.19,20 Only few studies mentioned a possible association between cigarette and water pipe smoking with low back pain,21,22 while no studies to date have addressed the effect of waterpipe smoking alone on intervertebral disc degeneration. This study also found that waterpipe smoking is associated with disc degeneration specifically at level L1-L2 and L2-L3. The mechanism through which waterpipe smoking causes disc degeneration is likely to be similar to that of cigarettes, 6 however future studies are needed to provide more evidence on the exact mechanism with a focus on the upper spinal levels.
Strength and Limitations
To our knowledge, this study is the first to explore the impact of water pipe smoking on lumbar intervertebral disc degeneration (IVDD). However, it has several limitations. First, the utilization of chart reviews led to a shortfall in data for several confounding variables, such as body mass index (BMI) and occupational exposure to lumbar strain. However, the lack of BMI data is not anticipated to have an impact on the association between smoking and IVDD. To illustrate, smoking has been associated with a reduction in appetite and an increase in metabolic rate. 23 This can lead to weight loss, and, in the long term, smokers often have lower body mass index (BMI) compared to non-smokers. 24 In addition, individuals with lower BMI may experience less mechanical strain on their spinal discs, potentially reducing the risk of degeneration. 25 Therefore, it is anticipated that individuals who smoke cigarettes or water pipes within our sample will likely exhibit lower BMIs compared to non-smokers, and thus have lower risks of disc degeneration. However, such assumption should be cautiously evaluated and addressed in subsequent studies. Additionally, the study did not assess the dose-response effects of smoking on disc degeneration, as risk factors were coded as binary variables (yes/no). Information on smoking quantity and duration was lacking, limiting the exploration of the nuanced relationship between smoking and disc degeneration. Due to resource constraints, only 10% of the cases were double-read (29 out of 286 total cases). This limited sample size, combined with the use of an ordinal scale, resulted in unreliable inter-rater reliability estimates and an increased risk of underestimating the true level of agreement between the radiologist and the resident. Lastly, this study offers a snapshot of the waterpipe smoking-disc degeneration association. Larger, longitudinal studies are necessary for establishing a causal link and understanding the dose-response relationship.
Conclusion
The current pilot study suggests a potential link between waterpipe and cigarette smoking and lumbar disc degeneration. However, further research is needed to validate these findings and establish a causal relationship, particularly regarding waterpipe use. Unlike cigarettes, which have a well-established connection with lumbar disc degeneration, waterpipe’s impact is still in early stages of exploration. A thorough prospective study, accounting for confounding factors, is crucial for a comprehensive understanding of the association between waterpipe use and lumbar disc degeneration. Such studies not only contribute to refining our knowledge but also heightens public awareness regarding the adverse effects associated with waterpipe use and lumbar disc degeneration.
Footnotes
Author Contributions
All Authors made substantial contributions to the following: conception and design of the study, data acquisition analysis and interpretation, article drafting and revision, final approval of the submitted version. HI: conceptualization, data curation, analysis, investigation, methodology, writing. TS: conceptualization, data analysis, investigation, methodology, writing. SA: data curation, analysis, methodology, writing. HB: data curation, analysis, methodology, writing. RK: data curation, analysis, investigation, methodology. ZW: methodology, data analysis, writing. GZ: methodology, data analysis, writing. DR: conceptualization, analysis, investigation, writing. CJS: conceptualization, analysis, project administration, methodology, writing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.