
Abstract
Aim:
To investigate the accuracy of pedicle screw placement based on preoperative computed tomography in comparison with intraoperative data set acquisition for spinal navigation system.
Methods:
The PubMed (MEDLINE), EMBASE, and Web of Science were systematically searched for the literature published up to September 2015. This review followed the Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines. Statistical analysis was performed using the Review Manager 5.3. The dichotomous data for the pedicle violation rate was summarized using relative risk (RR) and 95% confidence intervals (CIs) with the fixed-effects model. The level of significance was set at p < 0.05.
Results:
For this meta-analysis, seven studies used a total of 579 patients and 2981 screws. The results revealed that the accuracy of intraoperative data set acquisition method is significantly higher than preoperative one using 2 mm grading criteria (RR: 1.82, 95% CI: 1.09, 3.04, I 2 = 0%, p = 0.02). However, there was no significant difference between two kinds of methods at the 0 mm grading criteria (RR: 1.13, 95% CI: 0.88, 1.46, I 2 = 17%, p = 0.34). Using the 2-mm grading criteria, there was a higher accuracy of pedicle screw insertion in O-arm-assisted navigation than CT-based navigation method (RR: 1.96, 95% CI: 1.05, 3.64, I 2 = 0%, p = 0.03). The accuracy between CT-based navigation and two-dimensional-based navigation showed no significant difference (RR: 1.02, 95% CI: 0.35-3.03, I 2 = 0%, p = 0.97).
Conclusions:
The intraoperative data set acquisition method may decrease the incidence of perforated screws over 2 mm but not increase the number of screws fully contained within the pedicle compared to preoperative CT-based navigation system. A significantly higher accuracy of intraoperative (O-arm) than preoperative CT-based navigation was revealed using 2 mm grading criteria.
Introduction
Pedicle screw fixation is widely used in spinal surgery for traumatic, degenerative, and oncological diseases because of its three-column stability and good fixation for the vertebral body. 1 –3 The placement of pedicle screws not only influence clinical efficacy but also relate to complications of surgical treatment. The malposition of pedicle screws may lead to severe complications, including dural tearing, neural damage, and vascular or visceral injury, especially in the cervical and thoracic spine due to their complex anatomy and pedicle dimensions. 4 –6 On account of it, surgeons try several methods to improve the accuracy of pedicle screw placement.
Conventional pedicle screw placement focused on the anatomical landmarks, entry point, and insertion angle with or without intraoperative two-dimensional (2D) imaging can be performed by experienced surgeons. With the development of computer-assisted technology, image navigation is applied to spinal operation as the latest surgical procedure. Some research demonstrate that operations with the assistance of navigation systems result in a higher accuracy of pedicle screw placement and less risk of neurovascular injuries than operations without navigation systems. 7 –11 Common navigation systems applied to assist pedicle screw insertion include computed tomography–based navigation (CT Nav), 2D fluoroscopy-based navigation (2D FluoroNav), 3D fluoroscropy-based navigation (3D FluoroNav), and O-arm-assisted navigation (O-arm Nav). The first one involves preoperative data set acquisition and the rest involve intraoperative data set acquisition. CT Nav conducts preoperative CT scan of the target vertebrae and the data are transferred to the navigational system. After matching and registration for the operation, the preoperative anatomical information is then used to assist pedicle screw insertion. 12 Conversely, 2D FluoroNav, 3D FluoroNav, and O-arm Nav acquire information during the operation. 2D FluoroNav uses the intraoperative 2D images and provides real-time intraoperative visualization of spinal anatomy. 13 The 3D FluoroNav uses real-time intraoperatively 3D visualization. 14 O-arm Nav uses a 3D CT-like navigation system through a computerized image-guidance system. 15,16
Up to now, the difference in various navigation methods does not lead to a consistent view. Few studies analyze the difference in the accuracy of pedicle screw placement using navigation-assisted methods to acquire information preoperatively or intraoperatively. In this study, we performed a systematic review and meta-analysis to investigate the accuracy of pedicle screw placement based on preoperative computed tomography in comparison with intraoperative data set acquisition for spinal navigation system.
Methods
Search strategy
PubMed (MEDLINE), EMBASE, and Web of Science were searched for the literature published up to September 2015 based on the combination of the following key words: navigation, navigated, computer assisted, computer assistance, computer aided, image guided, image guiding, image guidance, neuronavigation, and pedicle screw. Reference lists of included studies were reviewed for additional relevant studies. No language or publication date restrictions were applied. Two reviewers (HL and WKC) independently screened all citations and abstracts identified to identify potential eligible studies.
Inclusion/exclusion criteria
Studies were included in the current meta-analysis if they met the following criteria: (1) the article must include navigated pedicle screw insertion based on preoperative computed tomography and intraoperative data set acquisition technique, (2) randomized-controlled trials or comparative studies (prospective and retrospective), and (3) accuracy of pedicle screw placement evaluated by postoperative computed tomography scans. Exclusion criteria were (1) the pedicle screw inserted without navigation, (2) no postoperative accuracy assessment done, (3) cadaveric and animal studies as well as studies that used spine models and morphologic articles, and (4) repetitive studies.
Data extraction
Data abstraction was conducted independently by two reviewers (HL and WKC), with any discrepancies resolved by discussion and consensus. Information extracted on each eligible study included authors, year of publication, type of study, patient characteristics, indications of surgery, methods of pedicle screw insertion (CT-based navigation, 2D/3D fluoro-based navigation, and O-arm-assisted navigation), number of pedicle screws inserted, outcome measurements (number of misplaced screws, pedicle screw violation), and screw-related complications.
Statistical analysis
Review Manager 5.3 (Nordic Cochrane Centre, Cochrane Collaboration, Copenhagen, Sweden) was used for meta-analysis. The dichotomous data for the pedicle violation rate were summarized using relative risk (RR) and 95% confidence intervals (CIs). The level of significance was set at p < 0.05. Heterogeneity was evaluated by χ2 test and I 2 statistics. If heterogeneity was significant (p < 0.10 and I 2 > 50%), the random-effects model was used. Alternately, the fixed-effects model was used. Funnel plots were examined for evidence of publication bias if sufficient studies were included for meta-analysis (n ≥ 10). 17
Results
Study inclusion and characteristics
The results of the search criteria and selection of trials for inclusion are expressed in a flow diagram of study selection as recommended by Preferred Reporting Items for Systematic Reviews and Meta-analysis. Figure 1 shows a summary of the study identification and selection process. After screening the title and reading the abstracts and the full text, we identified seven published retrospective comparative studies 6,12,18 –22 that met all inclusion criteria.

Flow diagram of the study identification and selection process.
A total of 579 patients and 2981 screws were included in the seven studies. All pedicle screws were inserted using the spinal navigation system. CT-based navigation and 2D fluoroscopy-based navigation were compared in three studies. 18 –20 CT-based navigation and 3D fluoroscopy-based navigation were compared in two studies. 18,21 And three studies 6,12,22 compared CT-based navigation with O-arm-assisted navigation (Table 1). The number of pedicle screws in different grades according to the postoperative CT assessment and screw-related complications of the respective studies are shown in Table 2.
Characteristics of included studies.

Pre: preoperative data set acquisition; CT Nav: computed tomography–based navigation; intra: intraoperative data set acquisition; 2D FluoroNav: 2D fluoroscopy-based navigation; 3D FluoroNav: 3D fluoroscopy-based navigation; O-arm: O-arm-assisted navigation.
Grade of screw and screw-related complications of included studies.

Pre: preoperative data set acquisition; intra: intraoperative data set acquisition. I, II, III, and IV are grades of pedicle screws.
Meta-analysis results
The comparison of accuracy of pedicle screw insertion between preoperative and intraoperative data set acquisition methods according to 2 mm grading criteria in six articles is shown in Figure 2. Meta-analysis revealed that accuracy of intraoperative data set acquisition method is significantly higher than preoperative one (RR: 1.82, 95% CI: 1.09-3.04, I 2 = 0%, p = 0.02). However, data analyzed in five articles with the 0 mm grading criteria (Figure 3) revealed no significant difference between the two kinds of methods (RR: 1.13, 95% CI: 0.88-1.46, I 2 = 17%, p = 0.34).

Pedicle screw insertion accuracy (2 mm): Preoperative versus intraoperative. Preoperative: computed tomography-based navigation. Intraoperative: two-dimensional (2D) fluoroscopy-based navigation, 3D fluoroscopy-based navigation, and O-arm-assisted navigation.

Pedicle screw insertion accuracy (0 mm): Preoperative versus intraoperative. Preoperative: computed tomography–based navigation. Intraoperative: two-dimensional (2D) fluoroscopy-based navigation, 3D fluoroscopy-based navigation, and O-arm-assisted navigation.
As a respective comparison, there was a higher accuracy of pedicle screw placement in O-arm-assisted navigation than CT-based navigation method, which was analyzed at the 2 mm grading criteria in Figure 4 (RR: 1.96, 95% CI: 1.05-3.64, I 2 = 0%, p = 0.03). Using the same 2-mm grading criteria, the accuracy of CT-based navigation and 2D-based navigation showed no significant difference, as shown in Figure 5 (RR: 1.02, 95% CI: 0.35-3.03, I 2 = 0%, p = 0.97). The difference between CT-based navigation and 3D-based navigation was not analyzed because of the different grading criteria in two studies 18,21 (0 mm and 2 mm).
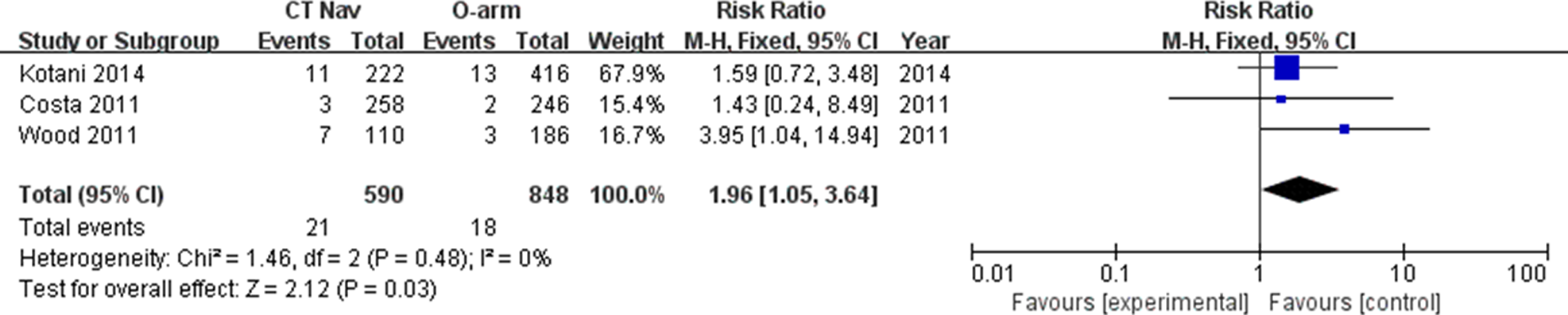
Pedicle screw insertion accuracy (2 mm): CT Nav versus O-arm. CT Nav: computed tomography–based navigation, O-arm: O-arm-assisted navigation.

Pedicle screw insertion accuracy (2 mm): CT Nav versus two-dimensional (2D) FluoroNav. CT Nav: computed tomography–based navigation; 2D FluoroNav: 2D fluoroscopy-based navigation.
Discussion
Several studies have reported that CT-based navigation system may provide higher accuracy of pedicle screw placement than conventional nonnavigated techniques. 9 However, the disadvantages such as the steep learning curve, the excessive operative preparation, and the intraoperative registration compared with other navigation systems are concerned raised by surgeons. What’s more, the main limitation of the CT-based navigation the variation in the patient position from that in the preoperative CT scan (which was obtained in a supine position preoperatively, but intraoperatively in prone position). For spinal instability resulting from trauma or isthmic spondylolisthesis, the position variation may change the intersegmental relationships between the adjacent vertebral levels, resulting in potential navigational inaccuracy. In the recent year, intraoperative data set acquisition navigation techniques are used to improve the accuracy of pedicle screw placement and solve the above problems, especially the position-dependent problem. 12 Moreover, intraoperative navigations offer the possibility of timely revision surgery for misplaced screws during the surgical procedure to decrease the incidence of postoperative complications.
Ideal pedicle screw should have a maximum diameter and length without breaching the cortical layer of the pedicle or the vertebral body. 23 According to the degree of cortex violation, most research consider pedicle violation as a safe zone of pedicle perforation of smaller than 2 mm. 24,25 The grade of pedicle screw violation based on Gertzbein classification 26 is defined into four groups: screws fully contained within the pedicle (grade I), perforated screws with up to 2 mm of displacement (grade II), perforated screws with 2–4 mm of displacement (grade III), and perforated screws with greater than 4 mm of displacement (grade IV). However, the grading criteria evaluating the accuracy of pedicle screw placement often varies in different studies. The seven articles enrolled in our study followed three kinds of grading criteria. We statistically analyzed these articles using the two criteria (0 and 2 mm). The results revealed significant difference using 2 mm criteria and no significant difference using 0 mm criteria, comparing the accuracy of pedicle screw insertion between preoperative and intraoperative data set acquisition methods. The intraoperative data set acquisition method may decrease the incidence of perforated screws over 2 mm but not increase the number of screws fully contained within the pedicle compared to the preoperative CT-based navigation system. The decreased number of perforated screws over 2 mm in intraoperatively real-time navigated methods may lead to lower incidence rate of severe complications. No statistical difference in 0 mm criteria implies that there is still the necessity to improve the computer-assisted navigation system for more accurate placement of pedicle screws and achieve more number of screws fully contained within the pedicle.
Tian et al. 27 revealed a higher median placement accuracy with a CT-based navigation system (90.7% vs. 85.5%) than with the 2D fluoroscopy-based navigation on 7533 lumbar pedicle screws. However, in our study, there was no significant difference in pedicle screw insertion accuracy (2 mm), with no consideration of screw violation directions between CT-based and 2D fluoroscopy-based navigation systems. Their own advantages and disadvantages of the two navigated methods may lead to the statistical result. 2D guidance is intraoperative real-time navigation but does not provide any axial images and the quality of the images is directly dependent on the resolution of the acquired fluoroscopic projections so that image interpretation may be difficult and navigation affected adversely. 12 CT-based navigation system provides axial, coronal, and sagittal images and decreases the reliance on intraoperative imaging and reduces the use of intraoperative ionizing radiation.
The O-arm navigation, one of the latest intraoperative imaging platforms, has been well acknowledged for its superiorities in surgeries for trauma or degenerative spinal diseases. 16,25,28 A higher accuracy of intraoperative than preoperative CT-based navigation was revealed in our meta-analysis results. The main reason may be the position changes (from supine to prone) of the patients. In addition, the automatic recognition and merging of intraoperative images with surgical anatomy and real-time registration minimize the range of error.
A cortex violation, in many cases, does not correlate with neurologic, vascular, and/or visceral complication. 29 In our study, only one article 21 reported two cases of nerve root injuries but no motor deficit, and other six articles reported no screw-related complications. Some studies suggest an association between the degree of cortex violation and the frequency of neurological symptoms. 30 The actual tendency is a continuous research to obtain better results minimizing surgical risks.
Several limitations should be interpreted in this meta-analysis. First, the types of studies enrolled in this meta-analysis were only retrospective comparative studies, of which the data included in the present study were reported from nonrandomized-controlled trials. A meta-analysis of such data leads to less powerful results compared to those obtained purely from randomized studies. However, a prospective randomized trial is difficult due to poor patient compliance and complex demographic characteristics of patients. Second, only seven articles were enrolled in this study. And there are not enough references to statistically analyze the difference between CT-based navigation and 3D-based navigation. More high-quality articles should be searched in other database systems to strengthen the quality of evidence.
Conclusion
The present systematic review provides a comprehensive evaluation of the available evidence on the accuracy of pedicle screw placement based on preoperative computed tomography in comparison with intraoperative data set acquisition for spinal navigation system. This meta-analysis found an overall significantly higher accuracy of pedicle screw placement with intraoperative data set acquisition than preoperative method using 2 mm grading criteria. However, there was no statistical difference in the number of screws fully contained within the pedicle between preoperative and intraoperative data set acquisition methods. A significantly higher accuracy of intraoperative (O-arm) than preoperative CT-based navigation was revealed using 2 mm grading criteria.
Footnotes
Authors’ Note
Hao Liu and Weikai Chen these authors are contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.