
Abstract
Purpose:
This study investigates the safety and accuracy of percutaneous pedicle screws placed using fluoroscopic guidance in the thoracolumbosacral spine among Asian patients.
Methods:
Computerized tomography scans of 128 patients who had surgery using fluoroscopic-guided percutaneous pedicle screws were selected. Medial, lateral, superior, and inferior screw perforations were classified into grade 0 (no violation), grade 1 (<2 mm perforation), grade 2 (2–4 mm perforation), and grade 3(>4 mm perforation). Anterior perforations were classified into grade 0 (no violation), grade 1 (<4 mm perforation), grade 2 (4–6 mm perforation), and grade 3(>6 mm perforation). Grade 2 and grade 3 perforation were considered as “critical” perforation.
Results:
In total, 1002 percutaneous pedicle screws from 128 patients were analyzed. The mean age was 52.7 ± 16.6. There were 70 male patients and 58 female patients. The total perforation rate was 11.3% (113) with 8.4% (84) grade 1, 2.6% (26) grade 2, and 0.3% (3) grade 3 perforations. The overall “critical” perforation rate was 2.9% (29 screws) and no complications were noted. The highest perforation rates were at T4 (21.6%), T2 (19.4%), and T6 (19.2%).
Conclusion:
The total perforation rate of 11.3% with the total “critical” perforation rate of 2.9% (2.6% grade 2 and 0.3% grade 3 perforations). The highest perforation rates were found over the upper to mid-thoracic region. Fluoroscopic-guided percutaneous pedicle screws insertion among Asians has the safety and accuracy comparable to the current reported percutaneous pedicle screws and open pedicle screws techniques.
Introduction
Minimal invasive techniques in spine surgery are expanding recently and indications for the usage of fluoroscopic-guided percutaneous pedicle screws had widened. The preference for percutaneous screws compared with the conventional open method of pedicle screw fixation was due to its advantages in reducing intraoperative bleeding, preserving muscular function, and lessening postoperative pain resulting in earlier recovery. 1 –4 Since its introduction, several studies had reported its perforation rates that vary from 0.4% to 23.0%. 5 –15 Majority of these studies were done on Caucasians. Only one publication reported exclusively on Asian patients 12 and three publications reported on mixed population which included Caucasian and Asian patients. 13 –15 In these studies, they evaluated on either less than 100 patients or less than 500 screws among Asian patients. None of them evaluated more than 1000 screws. Thoracic spine morphometric studies had documented the vertebral pedicle sizes in different populations in the world. 16 –25 The Caucasian population 16 –19,25 had been reported to have larger pedicle sizes when compared to the Asian population. 20 –24 This study aims to review the safety and accuracy of percutaneous pedicle screws among Malaysians which consist of a multiethnic Asian population.
Methods
Study design
This was a retrospective radiographic computerized tomography (CT) scan evaluation study. Subjects were chosen from consecutive patients who fulfilled the inclusion criteria from a single center. CT scans were routinely performed postoperatively to monitor treatment progression (e.g. tumor response to radiotherapy, bony fusion in spinal infection, and bony union in traumatic fractures). The study duration was between January 2008 and December 2014. The percutaneous screws used were the MANTIS system (Stryker Spine, Allendale, New Jersey, USA) and VIPER system (Depuy Synthes Spine, Raynham, Massachusetts, USA).
Technique of fluoroscopic percutaneous pedicle screw insertion
This technique can be used only if good visualization of the pedicle is obtained on the image intensifier. Relative contraindications for insertion of percutaneous pedicle screw were unclear fluoroscope images in obese patients, and sclerotic or poorly visualized pedicles in patients with metastatic spinal disease. A true anterior–posterior (AP) view of the corresponding vertebra was initially obtained. The trocar was positioned at the lateral border of the pedicle (right side at 3 o’clock or left side at 9 o’clock position) and should be in contact with bone. The trocar was then advanced medially parallel to the end plate. When the tip of the trocar approached the medial border of the pedicle on AP view, a lateral view was obtained. At this point, the trocar on lateral view should be at or slightly deeper than the posterior vertebral margin. The trocar was advanced until the middle of the vertebral body before a guide wire was inserted. The length of the screw was measured before the screw was inserted with caution not to allow the guide wire to advance any further. The screw size and length can be estimated based on preoperative radiographs or CT scan.
Skin incisions were more lateral in the upper thoracic (T1, T2) and lumbar region due to the convergence of the pedicles or its angulation in the axial plane. Starting points in the mid-thoracic region were slightly higher at right side at 2 o’clock or left side at 10 o’clock position, as entry into the sloping transverse processes may be difficult and starting points above the transverse processes were chosen. Extrapedicular screws were inserted for very small pedicles in the mid-thoracic region. Longer screws were chosen in the thoracic region to leave the head of the screws floating, so that rod placement will not be interfered by the prominence of the transverse processes.
CT examination
Evaluation of screw perforation was performed on PACs system (Centricity PACs, version 5.0, GE Healthcare) with protocols for CT imaging of the screws using 3 mm slice, whereby axial, sagittal, and coronal scans were performed. The plane for axial scans was parallel to the end plate of the corresponding vertebrae. Sagittal cuts were performed along the pedicle trajectory of the corresponding vertebrae whereas coronal cuts were evaluated at the midpoint of the pedicle of the vertebrae. Evaluation was done by two assessors, namely, Chee Kidd Chiu (CKC) and Mun Keong Kwan (MKK).
Screws with perforations were classified into two types of grading systems. For medial, lateral, superior, and inferior perforations, the pedicle perforations were assessed using a classification initially described by Gertzbein and Robbins 26 with modification by Rao et al. 27 (grade 0: no violation; grade 1: less than 2 mm perforation; grade 2: 2 to 4 mm perforation; and grade 3: more than 4 mm perforation). For anterior perforations, the pedicle perforations were assessed using a modified grading system (grade 0: no violation; grade 1: less than 4 mm perforation; grade 2: 4 to 6 mm perforation; and grade 3: more than 6 mm perforation). Grade 2 perforations were considered perforations with possible complications. Grade 3 perforations were considered critical perforation with high risk of early or late complications. Therefore, both grade 2 and grade 3 perforation were considered as “critical” perforation.
Data collection
Data collected by the assessors were immediately entered into a computerized spreadsheet for comparison and analysis. The total number of stabilized levels was defined as the number of levels that the rods span between the most superior instrumented vertebras and the most inferior instrumented vertebras. Screw density was defined as the total number of percutaneous screws used divided by the total number of stabilized levels. Perforation rate was defined as the total number of screws with perforation divided by the total number of screws inserted multiplied by 100%.
Complications
Clinical complications related to percutaneous screws breach or perforations were documented as well as any remedial actions taken when it occurs.
Statistical analyses
Analyses were done with SPSS v.14 statistical software (SPSS, Chicago, Illinois, USA). The α level was set at 0.05 to declare significance. Statistical analyses were done with the t-test for quantitative variables and the χ 2-test for qualitative variables. Inter-rater reliability was assessed using Cohen’s κ statistics.
Results
CT scans from 128 patients who had underwent surgery using percutaneous pedicle screws were available to be reviewed. The inter-rater reliability between the two evaluators was adequate with a κ value of 0.83. CT scans from 128 patients were evaluated and analyzed. The CT scans were performed on average 3.2 ± 2.0 months postoperatively. The mean age was 52.7 ± 16.6. There were 70 male patients and 58 female patients. Total numbers of screws inserted were 1002 with mean screws per patient of 7.8 ± 2.1, mean stabilized levels of 6.8 ± 2.6, and screw density of 1.4 ± 0.9. Overall, the main etiology was neoplasia (46.9%). Other etiologies were infection, trauma, and osteoporotic fracture (Table 1).
Demographics of study population.a

aValues are mean ± SD.
bNumber of screws per stabilized vertebrae.
The total number of pedicle screws, total screws with perforations, and the screw perforation rate according to vertebral levels are listed in Table 2. Of the total of 1002 screws, the average screw perforation rate was 11.3%. The grade 1 perforation rate was 8.4%, grade 2 was 2.6%, and grade 3 was 0.3%. Highest number of screws was placed in L2 (98) and L3 (98) followed by T11 (93). The highest number of perforations was at L1 (13), followed by T11 (12) and T6 (10). The highest perforation rate was at T4 (21.6%), followed by T2 (19.4%) and T6 (19.2%). Figure 1 illustrates the pattern of perforation rate according to vertebral levels.
Total number of percutaneous pedicle screws, screws with perforations, and the perforation rate according to vertebral levels.


Perforation rates distribution according to vertebral levels.
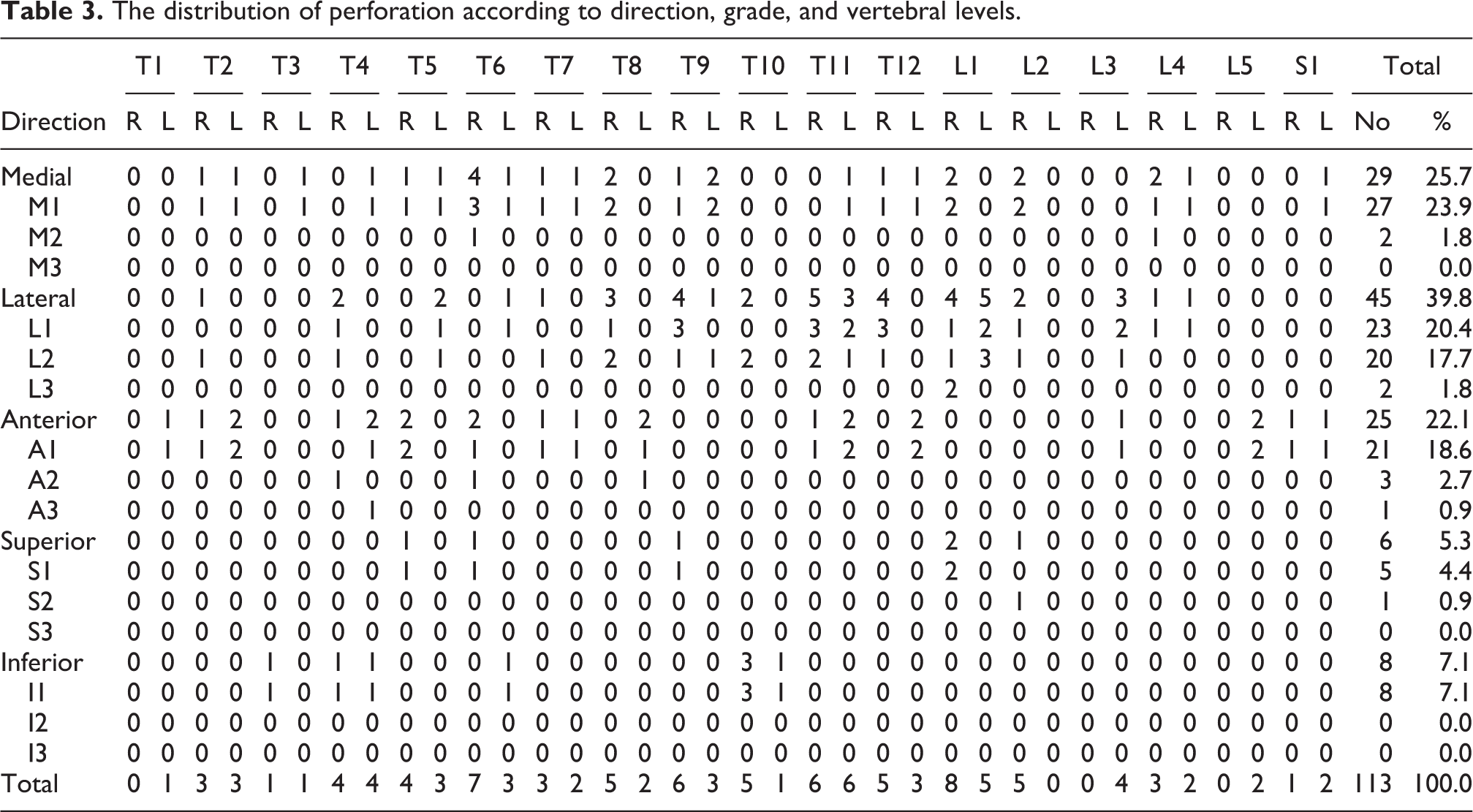
The distribution of perforation according to direction, grade, and vertebral levels was illustrated in Table 3. The highest perforations were directed laterally (45, 39.8%), followed by medially (29, 25.7%), anteriorly (25, 22.1%), inferiorly (8, 7.1%), and superiorly (6, 5.3%). Majority of these perforations were grade 1 perforations (84, 74.3%) with 27 (23.9%) directed medially, 23 (20.3%) laterally, 21 (18.6%) anteriorly, 5 (4.4%) superiorly, and 8 (7.1%) inferiorly. There were 26 (23.0%) grade 2 perforations with 2 (1.8%) directed medially, 20 (17.7%) laterally, 3 (2.7%) anteriorly, and 1 (0.9%) superiorly. There were 3 (2.7%) grade 3 perforations with 2 (1.8%) directed laterally at L1 level and 1 (0.9%) directed anteriorly at T4 level (Figure 2). There were no screw-related complications. Even though there were less right-sided pedicles screws placed compared to left (R: 499, L: 503), there were more right-sided perforations (R: 66, L: 47) with a higher right-sided perforation rate (R: 13.2%, L: 9.3%) (Table 3). However, when compared statistically, it was not significant (p = 0.052).
The distribution of perforation according to direction, grade, and vertebral levels.

Grade 3 perforations: (a) anterior left T4, (b) lateral right L1, and (c) lateral right L1.
Discussion
The accuracy, safety, and perforation of pedicle screws inserted with the conventional open method had been extensively studied. The perforation rates for the conventional open method had been found to vary from 1.5% up to 25% 26,28 –43 in clinical studies and similar variability from 1.6% to 29% 44 –52 were documented in cadaveric studies. A meta-analysis on 130 studies with 37,337 pedicle screws implanted had reported pedicle screw placement accuracy of 95.2% with navigation assistance and a lower accuracy of 90.3% without navigation. 53 Computer-assisted navigation percutaneous pedicle screw placement is a newer alternative to fluoroscopic-guided percutaneous pedicle screw placement. Several reports had documented screw perforations rates from 3.0% to 7.3% with computer-assisted percutaneous screws placement. 54,55 Despite the advantages of less radiation exposure, fluoroscopic-guided screws placement may still remain as the main feasible technique in many centers due to the cost and availability of computer-assisted navigation devices.
Fluoroscopic-guided percutaneous pedicle screw accuracy, safety, and perforation/breach rates had been reported in the literature (Table 4). Wiesner et al. 5 had reported a perforation rate of 6.6% for 408 percutaneous L1 to S1 screws placed in 30 cadaveric specimens, and Holly et al. 6 had reported a perforation rate of 5.3% (8.0% thoracic and 0% lumbosacral) in 94 fluoroscopy-guided percutaneous pedicle screws in the thoracic and lumbar vertebrae of three cadaveric specimens. Powers et al. 7 was the first to report in patients. He had pedicular breach of 0.39% in 287 thoracic and lumbosacral percutaneous screws for 67 patients. Ringel et al. 8 had reported pedicular breach of 13.0% in 488 thoracic and lumbar percutaneous screws for 104 patients. Schizas et al. 9 had reported screw perforation of 23.0% in 60 lumbosacral percutaneous screws for 15 patients. Smith et al. 10 reported pedicular breach of 6.2% in 601 lumbosacral percutaneous screws for 151 patients. Heintel et al. 11 evaluated 502 thoracic and lumbar percutaneous screws for 111 patients who sustained spinal injury and reported an accuracy rate of 98%.
Review of studies evaluating the accuracy of percutaneous pedicle screw placement.

? = Unknown or not mentioned in study.
For the Asian population, Oh et al. 12 compared the accuracy between 558 open pedicle screws in 126 patients and 498 percutaneous pedicle screws in 111 patients from L3 to S1 segments and found that the pedicle wall penetration was 13.4% and 14.3%, respectively. Chiu et al. 13 reported perforation rate of 9.9% in 880 lumbosacral screws for 203 Caucasian and Asian patients with perforation rate of 8.6% in 266 lumbosacral screws for 59 Asian patients. Kwan et al. 14 reported perforation rate of 9.7% in 880 thoracic screws in 148 Caucasian and Asian patients with perforation rate of 10.2% in 440 thoracic screws for 75 Asian patients. Hansen-Algenstaedt et al. 15 reported perforation rate of 9.4% (8.9% thoracic, 9.9% lumbosacral) in 2000 thoracic and lumbosacral screws for 273 Caucasian and Asian patients with perforation rate of 9.3% in 710 thoracic and lumbosacral screws for 90 Asian patients.
Thoracic spine morphometric studies had documented the vertebral pedicle sizes in different populations around the world 16 –25 and found that the Caucasian population 16 –19,25 has larger pedicle sizes when compared to the Asian population. 20 –24 Choi et al. 23 had identified that the pedicles were generally smaller in Koreans compared to Caucasians. Chan et al. 24 had reported similar findings in the Malaysian population. In this study, we recruited Malaysian patients who had surgery with fluoroscopic-guided percutaneous pedicle screws and found that the perforation rate was 11.3% (12.9% thoracic, 8.6% lumbosacral) in 1002 thoracic and lumbosacral screws for 128 patients which was comparable to the perforation rates among Caucasians.
Our findings revealed that there were generally higher rate of perforations in the upper and mid-thoracic region (T2 and T6). Several published literatures had noted a higher perforation rate at the upper and mid-thoracic region. 14,15 There are several possible explanations to this. Fluoroscopic images may be obstructed by the patient’s shoulder joint, scapula, and humerus in the upper thoracic region (T1 to T4). In a thin subject who is placed on a skull tong or a Mayfield skull clamp, with shoulders taped downward toward the foot end, lateral images of T1 or even T2 may be visualized. But this may not be possible in larger sized subjects or obese subjects. The convergence of the pedicles increases as one move up the thoracic spine. T1 pedicles have the highest angulation in the axial plane, followed by T2 pedicles among other thoracic vertebrae. 56,57 The mid-thoracic region has narrower pedicles when compared with the lower thoracic region. There are reports that documented that the narrowest thoracic pedicles were located at T4 22,23,58 or at T5. 24,25,59 These pedicles have a higher risk of perforations. Therefore, percutaneous pedicle screw under fluoroscopic guidance in the upper and mid-thoracic region carries a higher risk of perforation compared to the lower thoracic and the lumbar region.
We found that most perforations were directed laterally (45, 39.8%), followed by medially (29, 25.7%), anteriorly (25, 22.1%), inferiorly (8, 7.1%), and superiorly (6, 5.3%). There were a high number of grade 2 lateral perforations (20, 17.7%) with most of them in the thoracic region (14, 12.4%) compared to the lumbar region (6, 5.3%). This may be due to the usage of extrapedicular technique in cases with difficult transpedicular insertion. Extrapedicular technique can be used safely in the thoracic region because the rib-head may act as the barrier to protect the screws from injuring nearby structures or organs (e.g. lung).
Despite a total perforation rate of 11.3%, majority of the perforations were grade 1 (8.4%). The perforation rate for grade 2 was 2.6% and for grade 3 was only 0.3%. There were only three grade 3 perforations among a total of 1002 screws inserted percutaneously (Table 2). Two of these grade 3 perforations were directed laterally at L1 and one anteriorly at T4 (Table 3). None of the perforations led to any screw-related complications. These findings correspond with the current perforation rates in the literature (Table 4). However, further prospective studies may be needed to validate this assumption.
The limitations of this study were as follows: (1) no analysis was done to compare the effect of the type of etiology on the perforation rates of percutaneous screws; (2) there was also no evaluation on the amount of radiation that surgeons and operation theatre personnel were exposed to; (3) the CT scan slices were 3 mm width and the detection of perforation and estimation of the grade of perforation may be underestimated; (4) the comparison between ethic was not analyzed, and (5) the complications that were to be recorded in this study were complications directly caused by a perforated screws, not other perioperative or intraoperative complications.
Conclusions
The implantation of percutaneous pedicle screws insertion using fluoroscopic guidance among Asian population has the safety and accuracy comparable to the current perforation rates of percutaneous pedicle screws and open techniques of pedicle screws insertion. The usage of these minimally invasive percutaneous pedicle screws offers new alternative surgical approaches in treating patients with spinal disorders.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.