
Abstract
Background:
Proximal end of the humerus is a common site for both primary and metastatic bone tumors. Limb salvage with endoprosthetic replacement is the most common means of reconstruction, but it has been proved that cement spacer are more beneficial for inferior shoulder function. Thus, limb salvage can be replaced by cheaper spacers especially in poor societies.
Patients and methods:
This study included 20 patients, of whom 14 were female, with a mean age of 40.4 years (range 12–60). Among the study population, six were diagnosed with osteosarcomas, two chondrosarcomas, two myeloma, two lymphoma, four metastatic carcinoma in the breast, two giant cell tumor, and two recurrent chondroplastoma. Limb salvage was successfully done in all patients: Tikhoff–Linberg type I in 12 cases and type V in 8. Endoprosthetic replacement was done in eight cases. An on-table fabricated cement spacer was used in 12 cases.
Results:
Follow-up ranged from 12 to 75 months, with a mean of 25.9 months. Functional outcome was almost comparable in both types of reconstruction, especially patient’s satisfaction, with a mean function of 65%.
Conclusion:
A relatively expensive endoprosthesis could be replaced by a much cheaper cement spacer if their function is comparable.
Introduction
The proximal humerus is a relatively common site for primary and metastatic tumors of bone. 1 Multiple treatment options have been reported in recent years. In most cases, surgery comprises an essential element of therapy. 2 Patient acceptance for limb-preserving treatments is high. Therefore, amputation of the shoulder girdle should be avoided if possible. 3
The increasing and often unpredictable longevity of patients with metastatic disease, 1,4 coupled with higher-than-expected failure rates after internal fixation with or without intralesional treatment and radiotherapy, 5,6 has led to renewed interest in more aggressive local control efforts through proximal humeral resection and reconstruction. 7
Reconstruction of the defects that result after resection of the proximal humerus could be performed by different comparable methods. The most commonly used reconstructive techniques after proximal humeral resection are osteoarticular allografts (OAs), allograft–prosthesis composite (APC), and autograft–prosthesis composite. 7
Risks vary depending on the choice of reconstruction. Biological reconstruction can be complicated by fracture, infection, and subchondral collapse, leading to implant revision or removal. Difficulties with endoprosthetic reconstruction (EP) involve consequences of surgical resection of deltoid and rotator cuff, which include proximal subluxation, instability, and a reduction in functional range of motion. 2,3,8,9
Aim of the work
The aim of this work was to evaluate the outcome of (endoprosthetic vs. cement spacer replacements) reconstructions of the proximal humerus after tumor resection.
Patients and methods
This study included 20 patients presented with proximal humeral lesions, with a mean age of 40.4 years (range: 12–60 years), of whom 14 (70%) were female and 6 (30%) were male. Among the study population, six (30%) were diagnosed with lesions of osteosarcomas, two (10%) chondrosarcomas, two (10%) lymphomas, two (10%) myeloma, two (10%) giant cell tumor, two (10%) recurrent chondroblastoma, and four (20%) metastatic breast carcinoma.
In cases of primary bone sarcoma (the cases of osteosarcoma, chondrosarcoma, myeloma, and lymphoma), a wide resection of the tumor was carried out through an anterolateral approach, and based on the extension of the tumor in proximal part of the bone and its proximity to the joint capsule, the type of resection was preoperatively planned as either intra-articular (type I) or extra-articular (type V). In this study, type V resection was done in eight (40%) cases where the preoperative MRI showed tumor extension in the joint (all cases of osteosarcoma and cases of chondrosarcoma). This included resection of the proximal humerus, the shoulder joint, and the glenoid bone in bloc (extra-articular resection). Axillary nerve was sacrificed in three of those eight cases, according to the preoperative MRI study of the lesion.
In type I resection, the proximal humerus was resected through the joint line where the glenoid was saved, which was performed in the other 12 (60%) cases (of metastatic carcinoma, giant cell tumor, advanced chondroblastoma, lymphoma, and myeloma).
In benign aggressive lesions and metastatic lesions, an en bloc resection of the lesion was performed by preserving the soft tissues as much as possible.
Reconstruction of the skeletal defect was done by special type of tumor megaprosthesis (of all cases, eight (40%) had type I resection)—trial of improving the shoulder function by reattaching the rotator cuff muscles to the prosthesis through a special type of mesh wrapped around the prosthesis to allow soft tissue attachment (Figure 1).

Endoprosthetic replacement of the proximal humerus after resection of malignant bone tumor.
Twelve (60%) were reconstructed by an on-table fabricated cement spacer made using bone cement with metal rods inside, which was inserted into the medulla of the distal fragment of the humerus and fixed by bone cement. To get stability of this construct, it was hanged by nonabsorbable suture to the acromion (Figure 2).
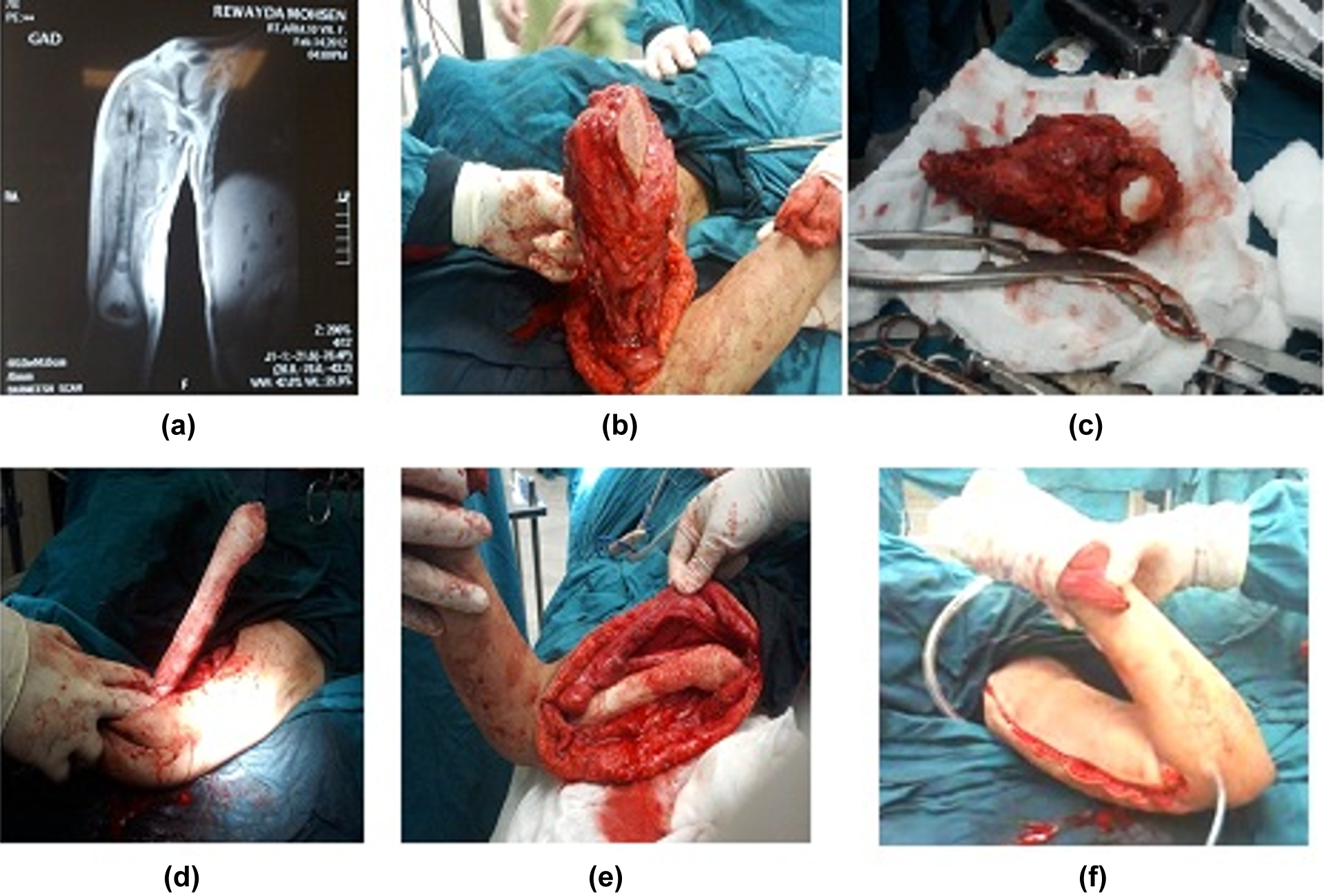
(a) Magnetic resonance imaging of osteosarcoma of proximal humerus in a 12-year-old girl. (b) Almost complete wide resection of the tumor just before distal humeral cut. (c) Resection specimen showing the humeral head. (d) Insertion of the hand made on side table cement spacer and fixation of it to the distal segment by cemented Kirschner wires. (e) Reduction in the cement spacer and attaching it to the acromion by nonabsorbable suture. (f) After soft tissue reconstruction and closure, the elbow fully flexed.
Postoperatively the upper limb was put in an arm sling with abduction splint for 6 weeks. Then a range of motion exercises were done to initiate the of shoulder function. In all cases, excellent elbow and hand function were observed.
Statistical analysis was done using the statistical program for social sciences version 20. The t test was used to determine the relations between the obtained results and the different variables. Five percent level of significance was chosen.
Results
All patients in this study were followed up for a duration of 12–75 months (mean 25.9 months). They were evaluated both clinically according to the musculoskeletal tumor society system (MSTS) 10 and radioghraphically at the end of follow-up. The overall functional outcome of both the groups was 65% (range 55–70%; Figure 3). Although three cases of cement spacer group had type V resection (Tikhoff–Linberg), 11 the axillary nerve was sacrificed. There was no significant difference in functional results between the groups (p = 0.213). No statistically significant relation were observed between the age, sex, type of the lesion, type of resection, and axillary nerve affection and the overall functional outcome (p = 0.100, p = 0.510, p = 0.235, p = 0.220, and p = 0.331). Four (20%) cases had complications, including three with chest metastasis and one with local recurrence, and one case of the endoprosthetic group had subluxation.

(a) and (b) X-ray and magnetic resonance imaging showing an advanced recurrent chondroblstoma of proximal humerus in a 14-year-old girl. (c) X-ray at the end of follow-up of this patient showing the cement spacer. (d) Left upper limb function (MSTS = 65%). MSTS: musculoskeletal tumor society system.
Discussion
The shoulder girdle is the third most frequent site for high-grade extremity sarcomas, and the proximal humerus is the most commonly affected bone. Osteosarcoma, chondrosarcoma, and Ewing’s sarcoma are the most common primary tumors arising in this location. 12 In this study, six cases (30%) had osteosarcoma and two (10%) had chondrosarcoma.
Before 1970, most patients with high-grade sarcomas involving the proximal humerus were treated with a forequarter amputation. 12 Marcove et al. 13 are the first to report limb-sparing treatment for high-grade sarcomas arising in this location. These authors reported performing an en bloc extra-articular resection of the proximal humerus, glenoid, overlying rotator cuff, lateral two-thirds of the clavicle, deltoid, coracobrachialis, and proximal biceps (long head). Local tumor control and survival rates were similar to those achieved with forequarter amputation. Resection, however, preserved a functional hand and elbow. These early oncologic results were confirmed by other surgeons, and limb-sparing surgery for high-grade sarcomas of the proximal humerus became a standard treatment.
The optimal reconstructive technique after proximal humerus resection is controversial. There are also different methods such as OAs, APC or autograft–prosthesis composite and EP. 7 In this study, we performed a new reconstruction method after resection using a cement spacer augmented by a metal rod inside it to act as a stem. The new reversed shoulder prosthesis was not used in this work due to the following reasons: (1) some cases carried general poor prognosis and the reversed prosthesis was costly, and also it was a relatively big surgery, (2) some cases had resection of the glenoid so there was no bone stock for reversed prosthesis, and (3) in some cases, the axillary nerve was sacrificed so the deltoid function was compromised. In this study, all cases of extra-articular resection were reconstructed by cement spacer, and some of the intra-articular resection cases were also reconstructed by spacer as either the prosthesis was not available (financial issues) or in cases where the axillary nerve was sacrificed.
Function after limb salvage procedures is multifactorial, and the anticipated result will vary widely, depending on the nature and amount of any preoperative adjuvant treatment, the tumor size and grade, the resection techniques, the stability of the reconstruction, the type and intensity of postoperative rehabilitation, and patient’s cooperation. 14 The overall functional outcome (65%) in this work was comparable with the functional results reported by other authors. The function of the upper limb and shoulder reported in most of the literature ranged from 40% to 83% according to MSTS score. O’Connor et al. 15 reported the functional results for five different reconstructions after resection of tumors of the shoulder girdle. Their MSTS functional rating for proximal humeral replacements was 61% compared to 65% of the overall results of both the groups in this study and 58.5% of cement spacer group. The main idea of this study was to show a much cheaper method of reconstruction but not on the expense of the function.
In this study, we did not find any difference in pain relief between the two groups as some of cement spacer cases had this surgery as a temporary step preparing for prosthesis, but they were happy and needed no further surgeries; for example, the case of recurrent chondroblastoma (Figure 3) had a recurrent lesion three times after curettage; the treatment was in the form of en bloc resection of the proximal humerus, because at that time the prosthesis was not ready due to financial and technical reasons. Hence, we decided to reconstruct using an on-table made cement spacer, and the patient was satisfied and she refused further surgery.
Courpied et al. 16 reported the functional results of 46 patients who had limb salvage procedures of tumors in the proximal humerus, excluding arthrodesis or massive allografts. According to the type of reconstructions, an endoprosthesis was used in 25 patients and a nail spacer in 9 patients, but 12 patients did not undergo any reconstruction procedure. The functional evaluation according to the MSTS classification revealed a rating of excellent for 1, good for 7, fair for 15, and poor for 23. Eighteen of the 23 patients with poor functional results had abductor mechanism resection. Eleven (24%) mechanical complications were reported in this series, with a second operation needed in eight.
In this study, all patients had a near normal elbow, forearm, and hand function, and this was comparable with Asavamongkolkul et al. 17 who reported that all of the patients in their study had normal manual dexterity of the elbow, forearm, and hand; each patient could get his or her hand to his or her face at a minimal level for activities of daily living.
In this study, four (20%) cases reported complications including chest metastasis in three cases and local recurrence in one, but one case of the endoprosthetic group had subluxation. Asavamongkolkul et al. 17 reported 6 of the 59 patients had subluxation or dislocation of the shoulder and 2 had infections. Local recurrence after limb salvage has been reported to range from 0% to 12%. 11,15,18
We found the rate of complications was comparable with the other methods of reconstructions. Benjamin et al. 7 in retrospective study included 49 patients who underwent glenoid-preserving segmental OA, APCs, or EP of the proximal humerus for the treatment of primary bone tumors or metastatic disease, wherein the implant survival estimates were 56%, 91%, and 100% for the OA, APC, and EP, respectively. They reported complications leading to reoperation in eight patients (47%) of the OA group compared with only four patients each (25%) in the APC and EP groups. Five patients (29%) experienced multiple complications after OA reconstruction. Specifically, allograft fracture occurred in nine patients (53%) in the OA group. One patient in the APC group had an allograft fracture, and no patient in the EP group experienced prosthesis or periprosthetic fracture. We did not report any periprosthetic or cement spacer fractures. Nonunion developed in one patient in both APC and OA groups. 7 Subluxation occurred in three patients in the OA (18%) and APC (19%) groups versus two patients in the EP group (13%), with three additional patients (19%) in the EP group requiring reoperation for overt dislocation. 7
Conclusion
Although the endoprosthetic replacement of proximal humerus is a durable method of reconstruction, the actual shoulder function is limited. A well-fabricated cement spacer with metal rods inside to act as a stem and give rigidity to the cement can give comparable results with significant reduction in the cost. Larger number of cases and longer follow-up are needed to verify these results and to asses survival of the cement spacer.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.