
Abstract
Purpose:
The aim of this study is to evaluate clinical and radiological results of simultaneous bilateral correction of genu varum with Smart frame.
Methods:
Between 2011 and 2015, a total of 25 patients (10 females, 15 males) who had bilateral genu varum deformity were operated bilaterally with tibial and fibular osteotomy in the same session, using Smart frame. The mean follow-up period was 28.7 (range, 13–45) months. All patients had bilateral tibial varus deformity. Femoral deformity was corrected in an earlier session in nine patients. Mechanical axis deviation (MAD), mechanical lateral distal femoral angle, mechanical medial proximal tibial angle (mMPTA) and posterior proximal tibial angle (PPTA) were measured preoperatively and postoperatively. Short Form-36 questionnaire was filled by the patients preoperatively and during the last follow-up.
Results:
The mean preoperative MAD was 37.6 mm (range, 9–98 mm), which improved to 8.4 mm (range, 3–44 mm) postoperatively (p < 0.05). The mean preoperative mMPTA was 76°, which improved to 89° (p < 0.05). The mean preoperative PPTA was 75.5°, which improved to 80.3 (p < 0.05). Ten problems (20%), two obstacles (4%) and no sequelae occurred in 50 legs of 25 patients.
Conclusions:
In conclusion, Smart frame is an accurate and reliable method for performing bilateral simultaneous deformity correction in patients with bilateral genu varum deformity. It can be applied for various childhood-induced severe tibial deformities such as achondroplasia, rickets, skeletal dysplasia and Blount’s disease.
Keywords
Introduction
Genu varum leads to a pathological mechanical load that may cause early degeneration of the knee joint. Therefore, correction of the deformity is essential in order to prevent gonarthrosis which causes functional disability. 1,2 Childhood disorders such as achondroplasia, rickets, skeletal dysplasia and Blount’s disease may cause deformity in tibia and genu varum. 3,4 The goals of surgical treatment are to correct the tibial deformity, restore the mechanical axis and lengthen the extremity if there is shortening. In adolescents and adults, surgical treatment options for genu varum deformity are acute correction with internal or external fixation and gradual correction with an external fixator. 5
In recent years, various spatial fixators have been introduced with advantages such as application through smaller incisions, minimal soft tissue stripping, correction of complex deformities in all planes, early weight bearing and faster learning curve. Smart correction frame, in short Smart frame (Response Ortho LLC, Edgewater, New Jersey, USA), is a kind of hexapod and computer-aided spatial fixator which also allows ease of application and planning. 6 Hexapod design of Taylor’s spatial frame (TSF) enables simultaneous angular, rotational and translational correction of tibial deformities. 7 In literature, successful results with TSF are reported in the treatment of genu varum deformity in adolescents and adults. 8 –13
The aim of this study is to evaluate clinical and radiological results of simultaneous bilateral correction of tibial varus deformity with Smart frame.
Materials and methods
Twenty-five patients (10 females, 15 males, mean age 19.4 ± 6.9 (range,14–39) years) with bilateral genu varum deformity (50 extremities) were operated bilaterally on the tibial deformity in the same session, using Smart frame (Response Ortho LLC) between 2011 and 2015. Aetiologies of the deformities are listed in Table 1.
Aetiologies of genu varum deformities.

All patients had bilateral genu varum deformity. The patients in whom simultaneous femoral deformity correction was performed, the patients with leg length discrepancy and the patients in whom two-level osteotomy was performed to correct tibial deformity were excluded from the study. Deformity was corrected with osteotomies applied one-third proximal of the tibia diaphysis and diaphysis of fibula. Femoral deformity was corrected in an earlier session in nine patients (due to rickets in seven and osteomalacia in two patients). Preoperative standing anteroposterior and lateral orthoroentgenograms were obtained in all patients, and deformity analysis was performed as suggested by Paley. 14 Preoperative and last control deformity analysis were performed by the same author in all patients, preoperatively and during the last follow-up. Mechanical axis deviation (MAD), mechanical lateral distal femoral angle (mLDFA) and mechanical medial proximal tibial angle (mMPTA) were measured in frontal plane; posterior proximal tibial angle (PPTA) was measured in sagittal plane (Figure 1).
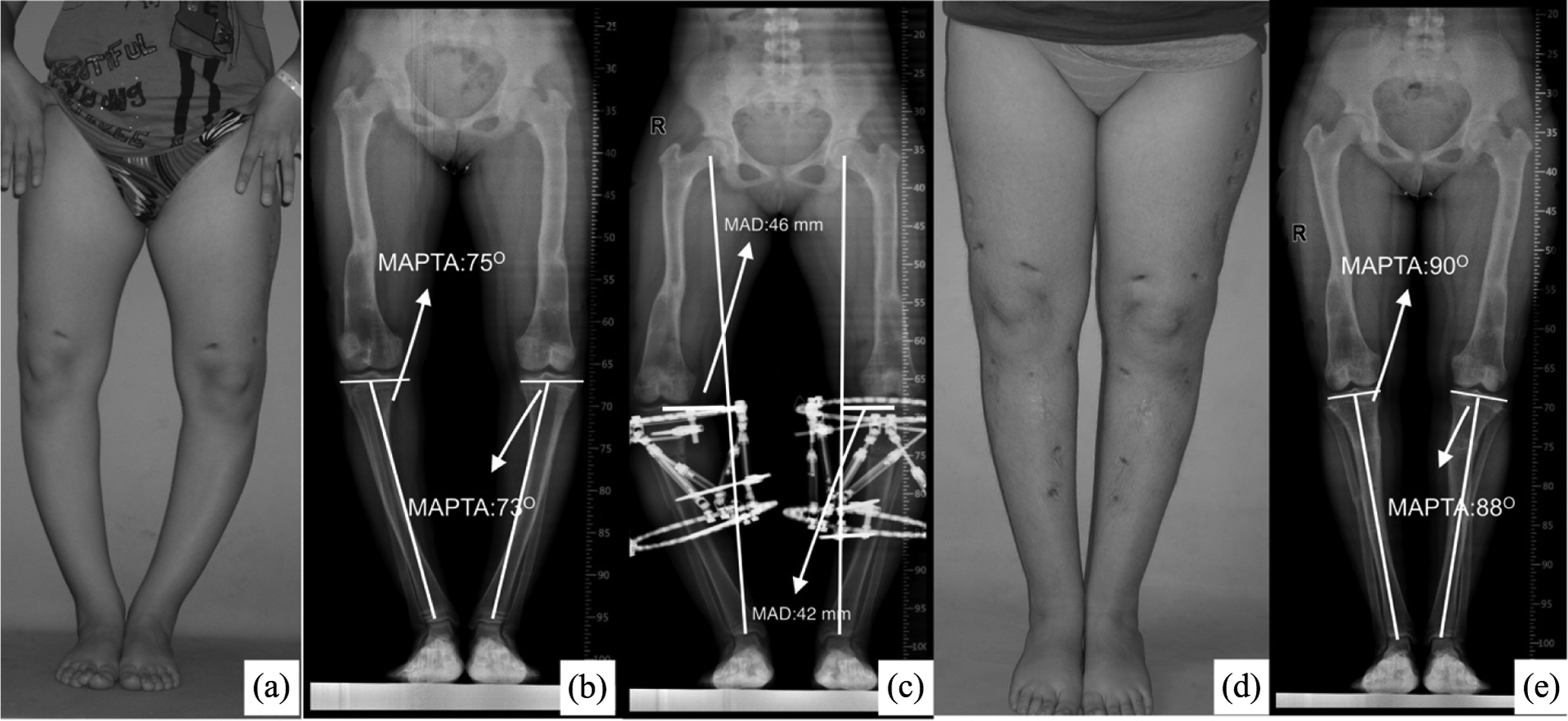
A 17 years old girl with rickets who had previous femoral correction surgery. (a) Preoperative photo, (b) preoperative standing anteroposterior orthoroentgenogram, (c) early postoperative photo, (d) last follow-up photo and (e) last postoperative standing anteroposterior orthoroentgenogram of the patient.
Operative technique and postoperative period
All surgeries were performed by two surgeons using the same technique. Patients were placed in supine position on a radiolucent table. Firstly, the proximal ring was fixed parallel to ‘knee joint line’ by two 6-mm half pins and one 1.8-mm Ilizarov wire. Then, the distal ring was fixed by three 6-mm half pins under fluoroscopic guidance. After the fixation of rings and installation of six struts, tibial osteotomy was performed through ‘centre of rotation of angulation’ (CORA) and fibula osteotomy was performed through proximal one-third diaphysis or diaphysis–metaphysis of the fibula. However, CORA of the tibial deformities located at the knee joint level (in four patients, due to Blount in two and skeletal dysplasia in two) or diaphysis–metaphysis level (in 11 patients, due to rickets in eight and osteomalacia in three), an osteotomy was performed in one-third proximal of the tibia diaphysis in accordance with osteotomy rule 2 principle. 14 Thus, correction was achieved in these patients with avoiding iatrogenic translation deformity. Osteotomy was performed as a corticotomy by drilling multiple cortical holes and connecting the holes with the help of an osteotome, with attention to protect intramedullar blood circulation. Patients were allowed weight bearing in the first postoperative day, and correction procedure was started in the seventh postoperative day. After the patients were discharged, they received a correction schedule which was determined with Smart frame software after computerized analysis of deformity correction and were called for follow-up weekly. Radiographs were obtained weekly during the correction process and then obtained monthly during the consolidation process. Fixators were removed once anteroposterior and lateral radiographs revealed unification of the osteotomy after the dynamization process (this was performed by loosening the struts and half pins). Standing anteroposterior and lateral orthoroentgenograms were obtained, and MAD, mMPTA, mLDFA and PPTA were measured during the last follow-up. Short Form-36 (SF-36) Health Survey questionnaire was filled by the patients preoperatively and during the last follow-up to evaluate quality of life. All complications were recorded.
Statistical analysis
Statistical analysis was performed with SPSS 20.0 (SPSS Inc., Chicago, Illinois, USA) software. Mann–Whitney U test was used to compare preoperative and last control measurements of MAD, mMPTA, mLDFA, PPTA and SF-36 score. The significance level was set at p < 0.05.
Results
Mean follow-up time of the patients was 28.7 ± 9.6 months (range, 13–45). The mean duration of the treatment with the frame was 20 ± 4 weeks (range, 15–29). MAD, mMPTA and PPTA improved significantly (p < 0.05; Table 2). Different aetiologies of genu varum were included in our study because of which MAD values varied from 9 to 98 mm. Wide ranges of MAD values were present in all diagnostic groups so there was no need to compare the results according to aetiologies. There was a statistically significant improvement in all components of SF-36 scores (p < 0.05; Table 3).
Preoperative and postoperative deformity analysis and p values.

MAD: mechanical axis deviation; mLDFA: mechanical lateral distal femoral angle; mMPTA: mechanical medial proximal tibial angle; PPTA: posterior proximal tibial angle.
aMean millimetre ± standard deviation.
bMean degree ± standard deviation.
Mean preoperative and postoperative SF-36 scores.

SF-36: Short Form-36.
Complications
One patient had anterior compartment syndrome postoperatively because of unknown aetiology, and fasciotomy was performed in the second postoperative day. Deep peroneal nerve palsy occurred in this patient which resolved in the second postoperative month. During the follow-up, one patient had deep peroneal palsy, which was resolved 3 months after the initial diagnosis; one patient had bilateral equinus deformity which was treated by bilateral percutaneous partial achillotomy. In 6 (12%) of 50 extremities, there was superficial pin site infection and all were treated with oral antibiotics. There was no cases of premature consolidation of tibial and fibular osteotomies. A walking cast was applied in two patients bilaterally after fixator removal due to delayed union.
Discussion
Bilateral genu varum deformity in adolescents and young adults may be due to various pathologic conditions such as congenital bowing, Blount’s disease, rickets and skeletal dysplasias. 15 Gradual correction of tibial deformity with external fixators reduces the complications associated with acute correction (peroneal palsy, compartment syndrome, delayed union, etc.) and provides better correction especially in multiplanar deformities. 16 Moreover, as weight bearing is not allowed after an acute correction, it is not possible to detect an implicit postoperative loss of correction, whereas loss of correction may be detected earlier in gradual correction as it allows obtaining standing radiographies. 5 The main indication for bilateral deformity correction with external fixation is the possibility of ambulation with early weight bearing as well as avoiding the complications of acute correction.
In the literature, there are some studies comparing circular external fixators with monolateral fixators in severe varus deformities with multiplanar deformities. 17,18 Kim et al. reported their results in skeletal dysplasia patients (96 extremities), wherein a mean correction of 9.3 mm in MAD was achieved with Ilizarov technique. 19 Park et al. performed gradual correction in patients with idiopathic genu varum using Ilizarov technique, and they reported that the mean MAD improved from 28.3 to 5.8 mm. 20
Gradual correction of tibia vara with spatial fixators was first described by Feldman et al. 8 They performed correction in 19 patients (22 extremities) with TSF and corrected the mean MAD from 53.9 to 1.4 mm, the mean mMPTA from 71.4° to 87.9° and the mean PPTA from 71.8° to 80.9°. Li et al. reported their results in 14 morbid obese patients with tibia vara. The mean MAD improved from 90 to 10 mm, the mean mMPTA from 66° to 88° and the mean PPTA from 80° to 81°. 5
In Blount and rickets, which are accompanied by severe varus and rotational deformities, it is essential to determine the number and localization of the osteotomies. 21,22 In the cases in which osteotomy could not be performed through CORA, Smart frame may be useful in avoiding iatrogenical translation deformity with its ability to the angulation correction axis (ACA) 14 through desired localization. Moreover, the big dimension of hexapod systems used in two-level osteotomy and correction procedures may affect the patient’s comfort negatively. Hence, we do not perform two-level osteotomies in bilateral simultaneous tibia deformity correction procedures.
There are a limited number of studies on correction of genu varum in patients with rickets. Petje et al. performed TSF in 13 segments, 21 and Küçükkaya et al. performed TSF in six patients. 12 Both reported successful results and deformity correction in all cases. Our study is the first report about the correction of genu varum and proximal tibial deformity bilaterally and simultaneously with Smart frame. In our study, we also achieved successful deformity correction in patients with Blount disease, rickets and skeletal dysplasia. The mean MAD improved from 28.3 to 5.8 mm.
Fibular osteotomy is a controversial issue in the correction of tibia vara because of some potential complications such as neurovascular complications, infection and non-union. In a study, authors compared the results of treatment of tibia vara with and without fibular osteotomy. 23 They reported delayed union and superficial pin tract infections in each groups and recommended correction of tibia vara without fibular osteotomy. Feldman et al. performed fibular osteotomy in 17 of 22 patients with tibia vara and no nerve palsy was reported. 8 We performed fibular proximal one-third shaft osteotomy in 50 extremities of 25 patients and encountered two (8%) deep peroneal nerve palsy. Deep peroneal palsies were both resolved in the follow-up, which proved that there was no nerve damage and it was not related to fibular osteotomy
Complications related to acute correction of genu varum deformity were previously reported in various studies. 9 Spatial fixators are safe devices with lower complication rates when compared with other external fixators. Dammerer et al. compared TSF with monolateral and Ilizarov fixators and reported significantly lower complication rates in TSF despite pin site infections and reduced knee range of motion. 24 Eren et al. reported that they encountered 46 problems, 11 obstacles and 7 sequelae with Smart frame in 77 extremities of 57 patients. 6 In our study, we encountered 10 problems (six pin tract infection, two delayed union, two deep peroneal palsy), 2 obstacles (bilateral equinus deformity) and no sequelae in 50 legs of 25 patients.
Different from TSF, Smart frame system is based on the matching of the X-ray image with the three-axial frame constructed by the software. Furthermore, the attachment sites of the six struts are defined optionally by the surgeon, and neither a mounting parameter nor a reference ring is required. Thus, the system becomes more practical in the fixation process. Ashfaq et al. compared monolateral frame with TSF and it was found that SF-36 scores improved in all categories except for general health in both groups. 17 They claimed that patients who had monolateral fixator in one leg and spatial frame in the other reported increased ease and comfort in the monolateral fixator side. However, authors reported that ‘same patients felt more secure and confident with spatial frame leg during mobilization and weight bearing’. In our study, SF-36 scores improved in all categories and no patients had reported discomfort during mobilization.
In conclusion, we achieved efficient and statistically significant bilateral simultaneous deformity correction with Smart frame in patients with bilateral genu varum deformities due to miscellaneous aetiologies. Hexapod external fixator is an effective and reliable system in the correction of isolated tibial varus deformity in these patients.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Each author certifies that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.