
Abstract
Objective:
To determine whether supplementary tibial graft fixation with a staple is routinely necessary for anterior cruciate ligament (ACL) reconstructions.
Methods:
We retrospectively reviewed a series of consecutive patients who underwent ACL reconstruction at our institution from April 2012 to July 2013. Patients who fulfilled the inclusion and exclusion criteria were divided into two groups, of which one with tibial fixation of the graft with a biointerference screw alone (biointerference screw group) and the other with tibial fixation of the graft with a biointerference screw and supplementary extra tunnel staple fixation (biointerference screw and staple group). All the surgeries were performed by a single fellowship-trained sports surgeon, using a standardized transportal technique and rehabilitation protocol. Both well-matched groups were evaluated at 1-year follow-up objectively for ligament laxity using instrumented testing with KT-2000 arthrometer and clinical tests as well as subjectively with the validated International Knee Documentation Committee 2000 (IKDC) and Lysholm knee score. All complications were reported.
Results:
A total of 64 patients (31 in the only biointerference screw group and 33 in the biointerference screw and staple group) were included in the study. At 1 year, there was no significant difference in the objective and subjective outcome assessments between the two groups. However, four patients from the group with supplementary staple experienced symptomatic hardware on kneeling of which two necessitated removal of hardware.
Conclusion:
Our study showed that supplementary tibial graft fixation with a staple is not routinely necessary for ACL reconstructions. It confers no additional benefits when compared with the use of biointerference screw alone for tibial graft fixation but may increase the risks of symptomatic hardware.
Keywords
Introduction
Anterior cruciate ligament (ACL) reconstruction is one of the most common orthopedic procedures and has a good track record in restoring knee stability and function to allow an individual to return to his/her preinjury level of activity that would otherwise have not been possible. 1 –6
In recent years, the use of hamstring grafts has gained popularity. The benefits include less donor site morbidity and greater overall graft strength. 7 –11 Studies have shown that soft tissue only grafts without a bone plug like the hamstring graft require bone-to-tendon integration which takes a longer time to occur, unlike the bone-to-bone integration seen in the bone–patellar tendon–bone graft. 12 –17 Fixation of the graft in the femoral tunnel provides a greater biomechanical strength than fixation in the tibial tunnel. This is due to the increased bone mineral density of the distal femur. Also, the forces acting against the graft are more parallel to the tibial tunnel. 18 As such, the tibial fixation is considered the weakest point of the initial construct in an ACL reconstruction. 14 –17
An important determinant of the success of the procedure is an early and aggressive rehabilitation protocol, prior to bone integration of the graft. The emphasis is on immediate range of motion, early weight bearing, strengthening, and return to sports. It is therefore important that initial fixation, especially tibial fixation, is as secure as possible, in order to avoid early failure or loss of graft tension. 19
Given that the tibial fixation is the initial weakest link of a reconstructed ACL, 14 –17 it is important to provide an adequate initial fixation to allow for aggressive rehabilitation before graft-bone integration occurs. Some authors have recommended supplementary fixation with a staple for soft tissue interference screw fixation to improve strength and stiffness of the fixation. 20 However, with staple supplemental fixation, there is a risk for symptomatic hardware, which may necessitate a second surgery for removal of hardware after the integration of the graft. 7
The aim of our study was to determine whether there is a significant difference in the clinical outcomes in patients undergoing ACL reconstruction using autologous hamstring tendons with tibial fixation using a bioabsorbable interference screw (biointerference screw group) and that of patients undergoing the same procedure with tibial fixation using a bioabsorbable interference screw and supplementary extra tunnel staple fixation (biointerference screw and staple group). This would give us a better understanding if supplementary tibial fixation is a necessary routine or if the proposed benefits are worth the risk.
Materials and methods
We retrospectively reviewed a series of consecutive patients who underwent ACL reconstruction, under a single surgeon at our institution from April 2012 to July 2013.
Inclusion and exclusion criteria
We identified 78 consecutive male and female patients between the ages of 18 and 35 years old who had undergone primary ACL reconstruction surgery using ipsilateral autologous hamstring tendon (HT) grafts, by a single surgeon, using the technique and postoperative rehabilitation described below, without meniscus repair and cartilage regeneration procedures at the same setting requiring postoperative bracing and prolonged protected weight bearing from April 2012 to July 2013, who had at least 1 year of follow-up postoperatively. Fourteen patients were excluded from the study. The exclusion criteria were patients with previous ipsilateral knee meniscus repair or menisectomy (n = 3), previous contralateral ACL reconstruction (n = 0), graft length shorter than 22 cm or inadequate length for a four-strand hamstring graft (n = 6), concomitant knee osteotomy (n = 2), and multiligament knee injuries (n = 3).
Standard surgical technique
The ACL reconstruction surgery was performed by a single surgeon, using a minimally invasive arthroscopically assisted transportal technique, with four-strand, autologous hamstring graft.
The choice of whether to use a supplementary staple was determined preoperatively. This reflects a change in practice of the primary surgeon. The primary surgeon had previously used interference screw and supplementary staples for the tibial fixation of the hamstring graft. However, as there was no evidence to suggest benefits of its routine use, 1 he had decided to change his practice to omit the use of staples. The patients selected for the study were consecutive cases of ACL reconstructions with or without supplementary staple tibial fixation even though there was a change in the practice of the surgeon.
The grafts were fixed on the femoral side with a continuous loop Endobutton (Endobutton CL) with 15 mm loop (Smith & Nephew Endoscopy, Andover, MA). Tibial fixation was achieved using a 25 mm long bioabsorbable polyethylene interference screw or with the same bioabsorbable polyethylene interference screw and supplementary staple fixation, with the diameter of the screw dependent on the size of the tunnel.
Under general anesthesia, examination of the knee was performed. If examination findings were congruent with a deficient ACL, harvesting of the hamstring graft was performed.
With a thigh tourniquet in place and inflated, a 2.5 cm longitudinal incision was made medial to the tibial tubercle, halfway between the anterior and posterior cortex of the tibia and 2 cm below the joint line. The semitendinosus and gracilis tendons were harvested using an open tendon stripper. The tendons were stripped of any adherent muscle and fashioned into a four-strand graft. The tendon strands were equally tensioned and the free ends of the graft were sutured for a distance of 30 mm using a No. 5 Ethibond (Ethicon, Edinburgh, Scotland) suture. A four-strand graft was created by folding both tendons into two. The graft diameter was measured by combining both grafts and folding it into two and passing it through a sizing block in 0.5 mm increments, and this measurement was used to select the appropriate router size for the tibial and femoral tunnels.
High anterolateral and low anteromedial portals were made and a diagnostic arthroscopy was performed. Meniscal lesions found were appropriately treated. The remnant ACL stump was removed and the intercondylar notch cleared. Care was taken to achieve anatomical placement of the femoral and tibial tunnels. The femoral tunnel was drilled using a transportal technique, with the knee positioned in maximum flexion, the position of the tunnel was placed in the middle of the ACL femoral footprint. A 2.4 mm guide wire was inserted followed by a drill over with a 4.5 mm cannulated drill. The length of the 4.5 mm tunnel was measured directly and the tunnel was further overdrilled from within the joint using the appropriate sized router, leaving a 5 mm rim of the outer femoral cortex. The folded end of the graft was passed into the loop of the Endobutton. Two markings were made, the proximal marking was the measured length of the tunnel, and was measured from the Endobutton to the appropriate position on the tendon. The distal marking was made 10 mm distal to the proximal marking. A heavy suture was threaded through the end of a Beath pin and pulled through the knee to emerge on the anterolateral surface of the distal thigh. The tibial tunnel location was identified in the posterior footprint of the ACL stump in line with the anterior horn of the lateral meniscus and the medial tibial spine. A 2.4 mm guide wire was inserted and overdrilled with the appropriate-sized router.
The hamstring tendon graft was delivered through the tibial and femoral tunnels using the pull-through suture and tensioned by traction on both ends. The graft was snugged into place in the femoral tunnel until the more distal marking was flush with the intraarticular femoral cortex. The Endobutton was flipped and the graft tensioned by pulling on the distal end. Tibial fixation was achieved with a cannulated biointerference screw over a guide wire and counter sunk 5 mm. The graft was tensioned manually and the screw was engaged in 30 degrees of knee flexion with a posterior drawer force applied to the knee. The length of the screw was constant at 25 mm and the width was the diameter of the tunnel rounded to the next size up. (i.e. an 8 mm screw for both 7 and 7.5 mm tunnels). In the patients who received supplementary fixation, an additional 7.94 mm × 23.22 mm regular fixation staple (Smith & Nephew Richards, Memphis, TN) was inserted distal to the screw to further secure the graft into the subcortical cancellous bone at the opening of the tibial tunnel.
Postoperative rehabilitation
All the patients had a standard postoperative rehabilitation, consisting of immediate weight bearing with the aid of crutches after surgery. No brace was used and the patients were encouraged to discard the crutches as soon as possible after surgery, usually within the first week. Patients attended physiotherapy sessions three times a week for the first 6 weeks after surgery, focusing on achieving full extension and contraction of the quadriceps and hamstring muscles. Jogging was commenced after 4 months, but return to competitive sport was restricted to at least 6 months after surgery.
Assessment
The patients were analyzed based on the type of tibial fixation used during the operation, whether a bioabsorbable interference screw was used alone (biointerference screw group) or a bioabsorbable interference screw and supplementary extra tunnel staple fixation was used (biointerference screw and staple group). Symptoms and signs of knee function were assessed to determine the International Knee Documentation Committee (IKDC) grade. The Lysholm knee score was also obtained by means of a questionnaire. Ligament stability was determined with an instrumented testing evaluation with the KT-2000 arthrometer (MEDmetric Corp, San Diego, CA) by measuring side to side differences at 20 lb. Inter limb differences were calculated by subtracting the laxity of uninjured knee from the laxity measurement of the injured knee. These were based on the 1-year assessment post-surgery.
Statistical analysis
All data were analyzed using Statistical Package for the Social Sciences (SPSS) software version 17.0 (SPSS Inc, Chicago, IL). The Student t-test was used for continuous data (KT-2000 arthrometer values, Lysholm and IKDC knee scores). Pearson’s χ 2 test was used to compare categorical data between the two groups. Statistical significance was assessed at the 5% level.
Results
Patient characteristics
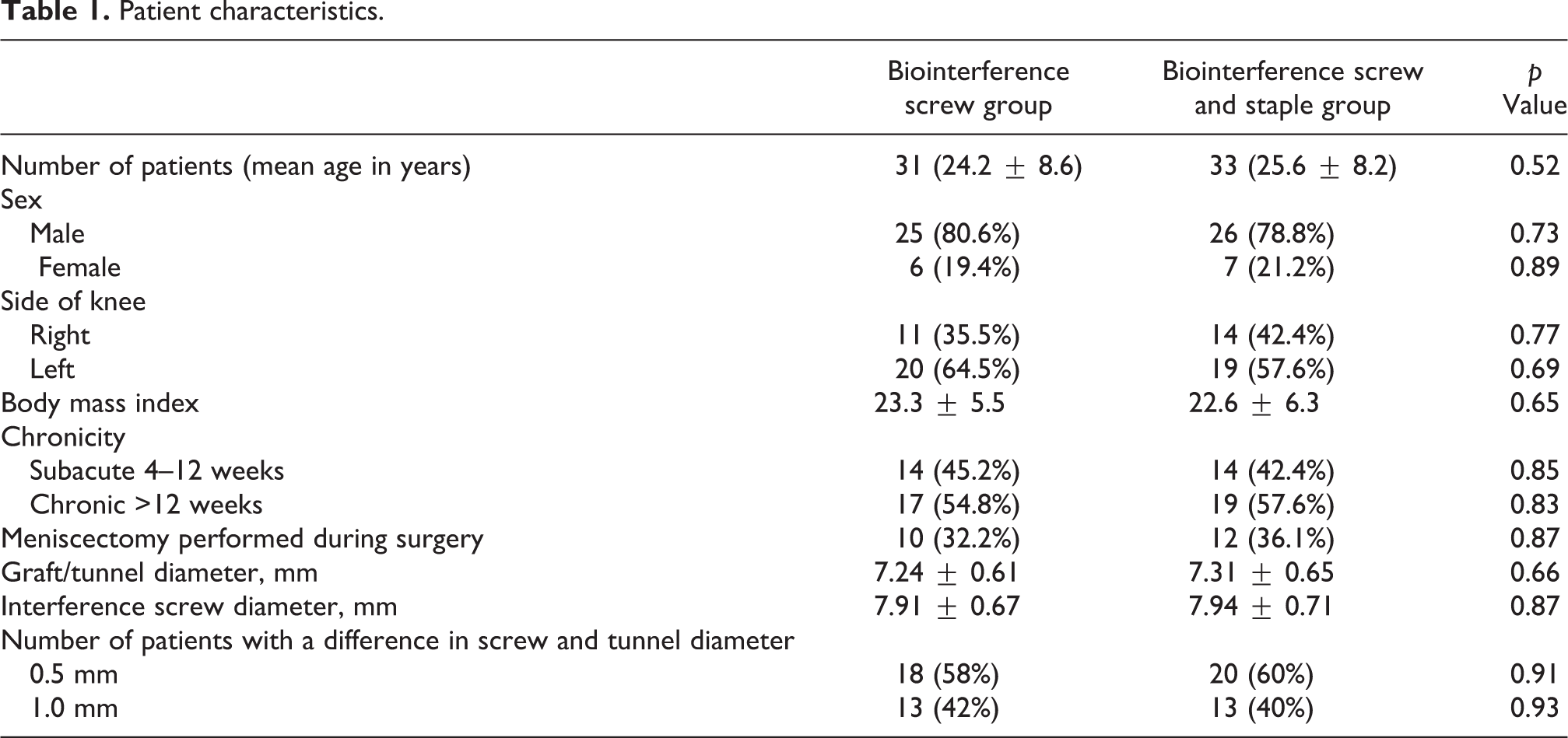
Sixty-four patients were evaluated in total: 31 patients in the group with tibial fixation of the graft with a biointerference screw alone (biointerference screw group) and 33 patients in the group with tibial fixation of the graft with a biointerference screw and supplementary extra tunnel staple fixation (biointerference screw and staple group). There were no significant differences between the two groups for age, gender, body mass index, tunnel diameter, or the laterality of the operated knee. A summary of the patient characteristics is shown in Table 1.
Patient characteristics.
Ligament laxity evaluation with KT-2000 arthrometer
The KT-2000 arthrometer is an instrumented device developed to measure translation of the tibia relative to the femur in a clinical setting. It only differs from its predecessor the KT-1000 arthrometer in its ability to graphically record output data 21 The side-to-side difference is a more accurate predictor of ACL deficiency as compared to the absolute translation. A side-to-side difference of >3 mm with test load of 20 lb is widely used in literature to be diagnostic of ACL deficiency, 22 with a sensitivity of 96%. 23
The results of instrumented testing are shown in Table 2. There was no significant difference between the two groups in terms of side-to-side comparison with arthrometer testing with a 20 lb load at 1 year. The mean side-to-side difference in the biointerference screw group was 1.65 mm compared to 1.72 mm in the biointerference screw and staple group.
Side-to-side difference on 20 lb load test with KT-2000 arthrometer at 1 year after surgery.
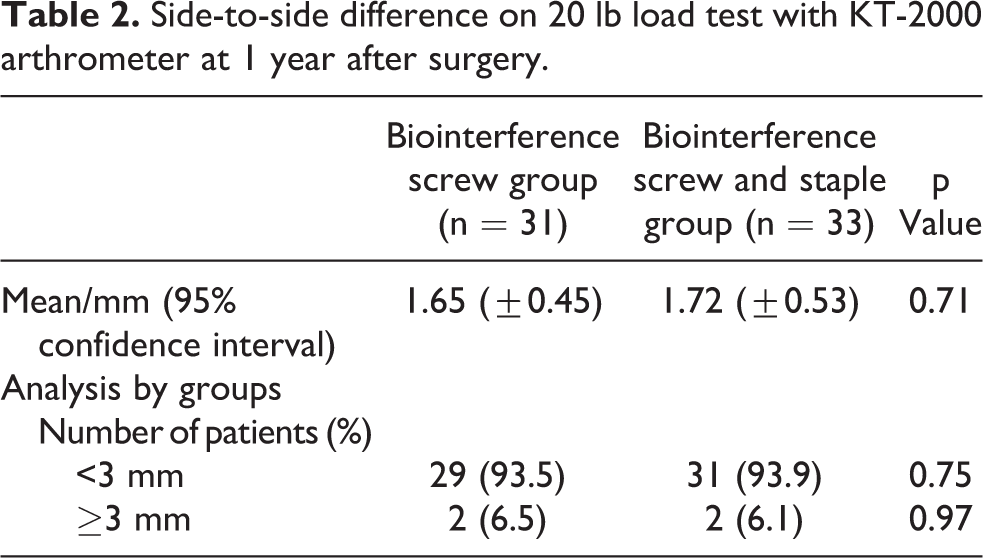
Analyzing the two groups based on whether arthrometer displacement was less than 3 mm or greater than or equal to 3 mm displacement also revealed no significant difference in the number of patients in both groups.
Clinical evaluation
At 1 year, the Lachman and pivot shift tests did not reveal any significant difference between the two groups: 93.5% of the patients in the biointerference screw group had a grade zero pivot shift test as compared to 93.9% in the biointerference screw and staple group. While 90.3% of patients in the biointerference screw group had a grade zero Lachman test as compared to 87.8% of the patients in the biointerference screw and staple group. The results are summarized in Table 3.
Clinical findings for patients with biointerference screw fixation and supplementary staple fixation 1 year after surgery.

Subjective outcomes (IKDC and Lysholm knee score)
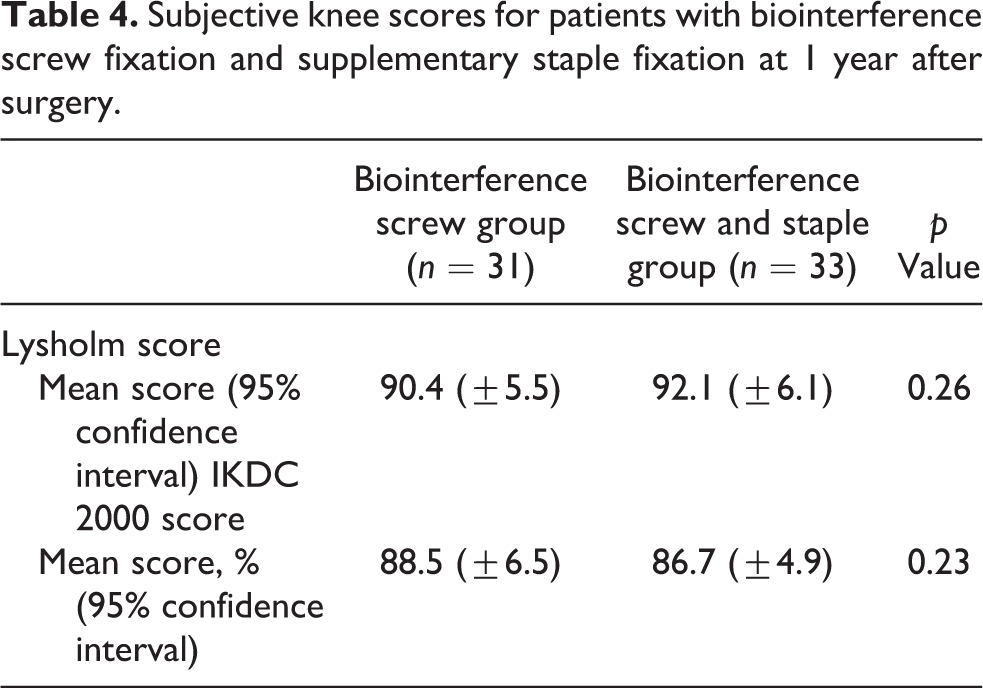
The Lysholm knee score has been considered the gold standard in the evaluation of knee in ACL injuries. It is a validated outcome measure of patient’s perception of their own disability, primarily focused on the assessment of knee instability. 24 –27 The International Knee Documentation Committee 2000 (IKDC 2000) subjective knee assessment is also a commonly used patient-oriented validated knee outcome measure used widely in literature. 27 –30 Comparing the patients in the biointerference screw group with the patients in the biointerference screw and staple group, there was no significant difference in the 1 year Lysholm and IKDC scores. The results are tabulated in Table 4.
Subjective knee scores for patients with biointerference screw fixation and supplementary staple fixation at 1 year after surgery.
However, it was noted that four patients in the biointerference screw and staple group found it moderately or extremely difficult to kneel on the front of their knees. This was attributed by all four of the patients to pain and irritation caused by prominence of the staple distal to the end of the tibial tunnel. There were no patients with similar complaints in the biointerference screw group (p = 0.039). Of these four patients with symptomatic hardware, two patients underwent a second procedure for removal of the staple (p = 0.21). The two patients who underwent surgery reported an improvement in pain on kneeling after removal of the symptomatic hardware.
Discussion
The principal findings in our study demonstrated that the use of supplementary staple fixation in addition to a biointerference screw for tibial graft fixation, in patients undergoing ACL reconstruction with an autologous four-strand HT tendon graft, had no significant difference in laxity on arthrometer testing when compared to using a biointerference screw alone. There was also no significant difference between the two groups in terms of clinical laxity testing with the Lachman and pivot shift tests. Moreover, the subjective patient outcomes on the Lysholm score and the IKDC 2000 score were comparable for both groups.
Nonetheless, the study showed that the use of a supplementary staple was associated with a significant increase in pain on kneeling for some patients (p = 0.039). It was also noted that there was a greater incidence of implant removal surgery with the use of the supplementary staple fixation. However, this was not statistically significant.
A previous study by Hill et al. 20 reported that female patients undergoing ACL reconstruction with a four-strand hamstring tendon autograft showed a statistically significant reduction in clinical laxity as measured with the Lachman test, with the use of a supplementary tibial staple together with a metal interference screw as compared to a metal interference screw alone. However, when the patients were analyzed using a side-to-side difference on arthrometer testing, this difference was not significant. They postulated that this could be due to the decreased bone density in the female proximal tibial metaphysis. This study also showed that the use of a supplementary staple fixation was also associated with a significant increase in incidence of kneeling pain. This suggests that a supplementary staple fixation should not be routinely used but could be considered as an adjunct to interference screw for selected cases, in patients with decreased bone density or with decreased insertion torque of the interference screw.
In our study, all the procedures were performed by a single fellowship-trained experienced sports surgeon, using the standardized transportal surgical technique. The femur fixation method, the length and type of interference screw were kept constant, and the tunnel sizes were drilled to the same diameter as the graft diameter in both groups. The biointerference screws were all inserted using a press-fit technique 0.5 mm or 1 mm larger than the tunnel diameter depending on whether the tunnel was a half-size. With the elimination of these known confounding factors, we believe that the direct effects of the supplementary staple fixation on graft laxity and outcomes can be assessed accurately.
Although our study is a retrospective study and the patients included are based on the change in practice of the senior author, the cases selected are consecutive cases and the patient characteristics as shown in Table 1 are relatively well matched, with no significant difference between the groups in key patient demographics. This helps to further decrease any confounding factors that might affect the results. Although the postoperative clinical evaluation of laxity was performed by the surgical team and prone to reporting bias, the arthrometer testing was performed by a different independent team. Despite this, the two results showed congruity.
The follow-up of 1 year is another limitation of the study. The ideal follow-up should be 2 years or more. However, Pinczewski et al. 31 reported that in humans, there is well-developed microscopic and macroscopic graft integration of the hamstring autograft at the graft–bone interface by 15 weeks, following which failure of the graft is at the midsubstance region. In an earlier animal study, Rodeo et al. 32 also found substantial collagen bone connections between tendon and the tibial tunnel and that failure by tendon pullout from the tunnel occurred up to 8 weeks after surgery. By 12 weeks, there were no failures from tendon pullout at the tibial bone–tendon interface. Although the study only has follow-up of up to 1 year, there is more than enough time for biological integration of the graft to have taken place. Our study aimed to study the effect of the supplementary staple at the early postoperative stage during unprotected aggressive rehabilitation before bone integration of the graft. By 1 year, bony integration of the graft should have taken place and tibial graft fixation is no longer the limiting factor for graft laxity or failure. Moreover, other large profile clinical arthrometer studies on ACL reconstruction have also reported on outcomes up to 1 year. 33
Conclusion
The use of the biointerference screw for tibial graft fixation in ACL reconstruction, using a 4-strand hamstring graft, showed adequate fixation strength to withstand the rigors of early aggressive rehabilitation. The use of a staple as a supplementary fixation in addition to the biointerference screw did not show any difference in terms of objective arthrometer measurements comparing side-to-side differences in anterior displacement of the tibia, as well as subjective clinical assessment and patient reported outcomes. There was, however, a significant increase in the risk of symptomatic hardware causing pain on kneeling. This may necessitate a second surgery for removal of the symptomatic hardware in some patients with the supplementary staple, though this was not statistically significant. Although our study is retrospective in nature, our groups are relatively well matched in terms of patient demographics, with a single surgeon using a standard surgical technique, with identical rehabilitation protocols. We believe that the use of a staple to supplement tibial graft fixation with a biointerference screw should not be used routinely, as this does not confer any significant benefit, and would result in potential complications of symptomatic hardware.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.