
Abstract
Purpose:
The factors affecting anterior tibial subluxation (ATS) have not yet been well examined. To assess the factors affecting ATS in anterior cruciate ligament (ACL)-deficient knees.
Methods:
One hundred twenty-four patients with unilateral ACL injuries were included. True lateral views of the ACL-deficient knee and contralateral normal knee were obtained during maximum extension using fluoroscopy under general anesthesia, and ATS was calculated as the side-to-side difference in the tibial position relative to the femur. Patients were divided into four groups according to the time from injury to surgery. To identify the factors affecting ATS, the following possible factors were assessed: (1) the time from injury to surgery, (2) presence of a medial meniscal injury, and (3) posterior tibial slope angle.
Results:
There was a positive correlation between the ATS ratio and the time from injury to surgery (r = 0.52). The ratio of the presence of a medial meniscus injury was significantly higher in patients who underwent anterior tibial subluxation reconstruction (ACL-R) more than 12 months after an injury than in other patients who underwent ACL-R within 12 months after an injury. The ATS ratio was significantly higher in patients with a medial meniscus injury than in those without a medial meniscus injury (5.6% vs. 4.1%).
Conclusions:
Our results suggested that ACL-R should be performed within 6 months after injury if surgeons prefer to avoid an increase in ATS in maximum knee extension and at the latest within 12 months to avoid medial meniscal injury at the time of ACL-R.
Keywords
Introduction
The anterior cruciate ligament (ACL) is a primary restraint in knee joint stability. Additionally, ACL rupture is a common injury associated with permanent sequelae that affects knee stability and function. Symptoms of instability resulting from increased anterior-posterior motion of the tibia relative to the femur often limit the activities of a patient who has an untreated-ACL rupture. 1 It has been proven that an ACL deficiency causes abnormal tibiofemoral relationships in the sagittal plane 2,3 and abnormal tibiofemoral relationships alter stress distributions in knee cartilage, predisposing the knee to degenerative changes including osteoarthritis. 4 –7
Vahey et al. reported that anterior tibial subluxation (ATS) occurred in the knee-extended position without external force in ACL-deficient knees on sagittal magnetic resonance imaging (MRI) scans. 3 Mishima et al. also reported on ATS at maximum knee extension in ACL-deficient knees. In addition, they reported that ATS increased over time between injury and surgery, and it was positively correlated with anterior instability of the knee. 8 Further, Almekinders et al. reported that the tibia subluxates anteriorly with respect to the femur even after anterior tibial subluxation reconstruction (ACL-R) despite the reduction of total tibial translation. 9 Thus, an abnormal tibiofemoral relationship was found to be an irreducible fixed anterior subluxation of the tibia relative to the femur.
Although ACL is the primary restraint for anterior tibial translation (ATT), several other structures have been reported to contribute to ATT. Previous biomechanical studies have shown that medial meniscus is a secondary restraint for ATT in ACL-deficient knees. 10,11 Besides, it has been reported that the posterior tibial slope (PTS) has a direct effect on sagittal plane laxity and contributes to the loading behavior of the ACL. 12 –16 Biomechanical studies have also shown that the PTS produces an anteriorly directed shear force component when a compressive tibiofemoral load or a quadriceps muscle force is applied to the knee joint, resulting in an ATT relative to the femur. 12,14,17 Accordingly, the medial meniscus and tibial slope are important structures in controlling anterior-posterior tibial translation and may affect ATS.
As aforementioned, ACL deficiency causes ATS. However, the factors affecting ATS have not yet been well examined; therefore, the purpose of the current study was to assess the factors affecting ATS in ACL-deficient knees. In the present study, ATS was quantified using a fluoroscopy device under general anesthesia. It was hypothesized that ATS would increase in patients who had a longer time from injury to surgery, those with a medial meniscus injury, and patients with a steeper PTS.
Patients and methods patient information
One hundred twenty-four patients who underwent ACL-R for ACL deficiency were enrolled in this study. Sixty male patients and 63 female patients were included, with a mean age of 27.2 ± 11.2 years (range: 13–59 years). Patients who met any of the following criteria were excluded from this study: (1) a history of trauma, (2) the presence of a symptom in the contralateral knee, (3) an extension deficit of either knee, and and other ligamentous injuries. All patients had complete rupture of the ACL, which was confirmed during surgery. ATT was measured using the KT-1000 arthrometer (MedMetric, San Diego, California, USA) with a manual maximum force at 30° of knee flexion in all patients. Anterior-posterior knee laxity was assessed by the side-to-side difference of ATT.
Measurement of ATS
Before ACL-R, true lateral views of both knees at maximum extension were captured using a fluoroscopy device (BV-29; Philips, Best, The Netherlands) in the operating room under general anesthesia. 18,19 During fluoroscopy, the patient’s heel was held by an examiner (Figure 1). The captured views were imported to a personal computer, and ATS was analyzed using a custom-made software 19 as follows. First, a line was drawn from the peak anterior point (A) to the posterior point (B) of the medial tibial plateau. Second, the point on the line A-B perpendicular from the anterior point of the Blumensaat line was defined as point C. (A−C)/(A−B)×100% was calculated to evaluate the relative tibial position to the femur, and the side-to-side difference (the value in the ACL-deficient knee—the value in the contralateral normal knee) was defined as the ATS ratio (Figure 2).
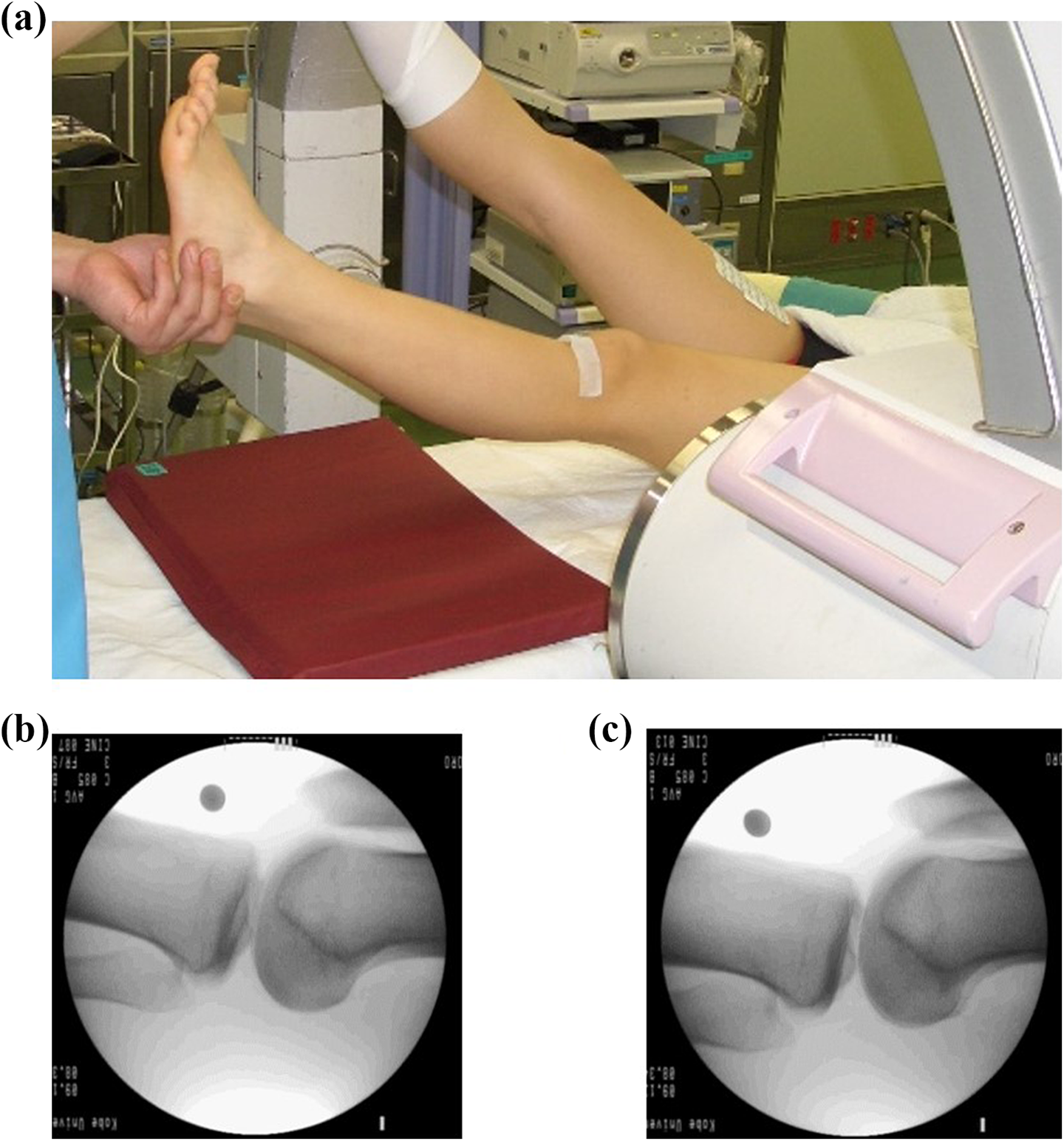
Fluoroscopic images. (a) The methods and position of the imaging. True lateral view of the ACL-deficient knee (b) and contralateral normal side (c). ACL: anterior cruciate ligament.
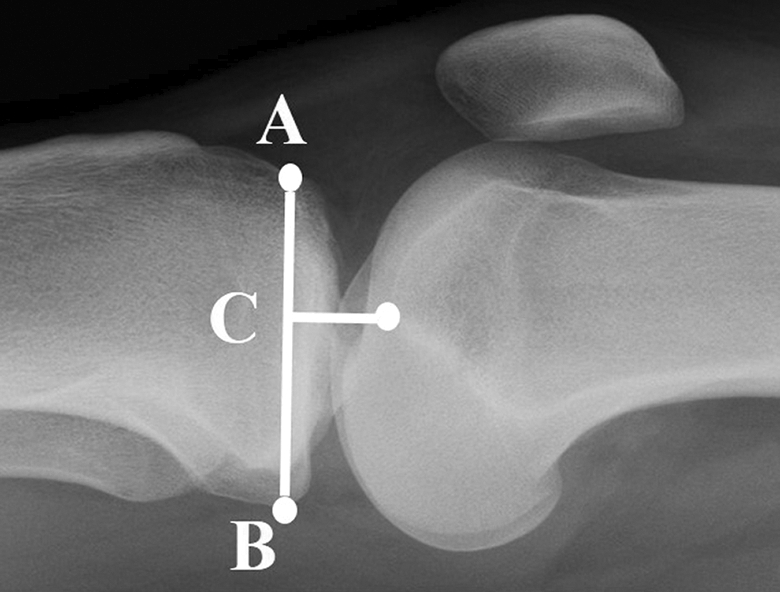
The definition of ATS in this study. A: The peak anterior point of the medial tibial plateau. B: The posterior point of the medial tibial plateau. C: The point on the line A-B perpendicular from the anterior point of the Blumensaat’s line. The ratio of A-C (in respect) to A-B was defined as the ratio of ATS to the femur, and the side-to-side difference was evaluated. ATS: anterior tibial subluxation.
Measurement of the PTS angle
The PTS angle was measured on radiographs in the lateral view, and it was defined as the angle between the tangent to the medial tibial plateau and the perpendicular direction to the tibial proximal anatomical axis. 20,21
The presence of meniscus injury
The presence of meniscal injuries was examined arthroscopically during ACL-R. Medial and lateral menisci were evaluated, and if the meniscal tear was judged as unstable by probing, partial meniscectomy or meniscal repair was performed. Unstable meniscal tears that needed partial meniscectomy or meniscal repair were defined as a meniscal tear, and stable meniscal tears were not included as a meniscal tear. In this study, the presence of a medial meniscal tear was analyzed as a factor of ATS.
Grouping by the time from injury to surgery
Patients were divided into four groups according to the time from injury to surgery: group 1, within 3 months after injury; group 2, between 3 and 6 months after injury; group 3, between 6 and 12 months after injury; and group 4, more than 12 months after injury. To identify the factors affecting ATS, relationships between ATS and (1) the time from injury to surgery, (2) presence of a medial meniscal injury, and (3) PTS angle were assessed among the groups.
Statistical analysis
All values are expressed as a mean ± standard deviation. Results were analyzed using a statistical software package (Ekuseru-Toukei 2012; Social Survey Research Information Co., Ltd., Tokyo, Japan). Statistical differences in sex, age, time from injury to surgery, PTS, and side-to-side difference of anteroposterior translation according to the KT-1000 arthrometer among the groups were compared using one-way analysis of variance (ANOVA). Post hoc testing was performed using the Tukey–Kramer methods to assess the data considered significant by ANOVA. The ratio of concomitant medial meniscus injury and the time from injury to surgery was compared using the Fisher exact test. The side-to-side difference of the ATS ratio was compared between patients with and without a medial meniscal injury using the Student t test. p < 0.05 was considered statistically significant. A post hoc power analysis was performed to assess the differences using G*Power 3 (Universität Kiel, Kiel, Germany). 22 The power of each analysis was calculated as follows: 0.99, relationships between ATS and the time from injury to surgery; 0.98, relationships between ATS and the time from injury to surgery in patients who had a medial meniscus injury; and 0.86, relationships between ATS and the time from injury to surgery without medial meniscus injury.
Results
Patients’ demographic characteristics
Patients’ demographic data are summarized in Table 1. There were no significant differences in sex, age, the PTS angle, and side-to-side difference of ATT among the groups.
Demographic data for all patients based on the duration of the ACL deficiency.a

PTS: posterior tibial slope; n.s: not significant; M: male; F: female; ACL: anterior cruciate ligament.
aValues are expressed as a mean ± standard deviation.
bSignificant difference between group 4 and the other three groups
Relationships between the time from injury to surgery and ATS
The mean time from injury to surgery was 8.8 ± 17.8 months (range, 18 days to 61 months). The mean side-to-side differences of the ATS ratio were 2.4 ± 2.4% in group 1, 3.6 ± 2.7% in group 2, 6.0 ± 3.9% in group 3, and 8.5 ± 2.7% in group 4 (Figure 3). Although there were no significant differences between group 1 and group 2 (p = 0.29), there were significant differences between group 1 and group 3 (p < 0.01), group 1 and group 4 (p < 0.01), group 2 and group 3 (p < 0.01), group 2 and group 4 (p < 0.01), and group 3 and group 4 (p = 0.03). There was a positive correlation between the side-to-side difference of the ATS ratio and the time from injury to surgery (r = 0.52, p < 0.01) (Figure 4).

The relationship between ATS ratio and time from injury to surgery. ATS: anterior tibial subluxation.

The relationship between ATS ratio and time from injury to surgery. There was a positive correlation between the side-to-side difference of the ATS ratio and the time from injury to surgery (r = 0.52, p < 0.01). ATS: anterior tibial subluxation.
Relationships between the presence of a meniscus injury and ATS
The prevalence ratios of concomitant medial meniscal injury were 29.0% (9/31) in group 1, 23.9% (11/46) in group 2, 29.6% (8/27) in group 3, and 55.0% (11/20) in group 4. The prevalence ratio of a medial meniscal injury was significantly higher in group 4 compared with the other 3 groups (p = 0.049; Table 1). The side-to-side difference of the ATS ratio was significantly higher in patients with a medial meniscal injury than in those without a medial meniscus injury (p < 0.01; Table 2). The side-to-side difference of the ATS ratio in patients with or without medial meniscal injury was also compared among all 4 groups. The mean side-to-side difference of the ATS ratio tended to be higher in patients with a medial meniscus injury in groups 1 and 2. In group 3, the mean side-to-side difference of the ATS ratio was significantly higher in patients with a medial meniscus injury than in those without a medial meniscal injury (Table 2). There was a positive correlation between the side-to-side difference of the ATS ratio and the time from injury to surgery in patients with and without a medial meniscal injury, although the correlation was slightly stronger in patients without medial meniscal injury than in those with a medial meniscal injury (r = 0.56, p < 0.01 and r = 0.40, p < 0.01, respectively; Figure 5).
ATS according to the duration of the ACL deficiency and the presence or absence of a medial meniscus injury.a
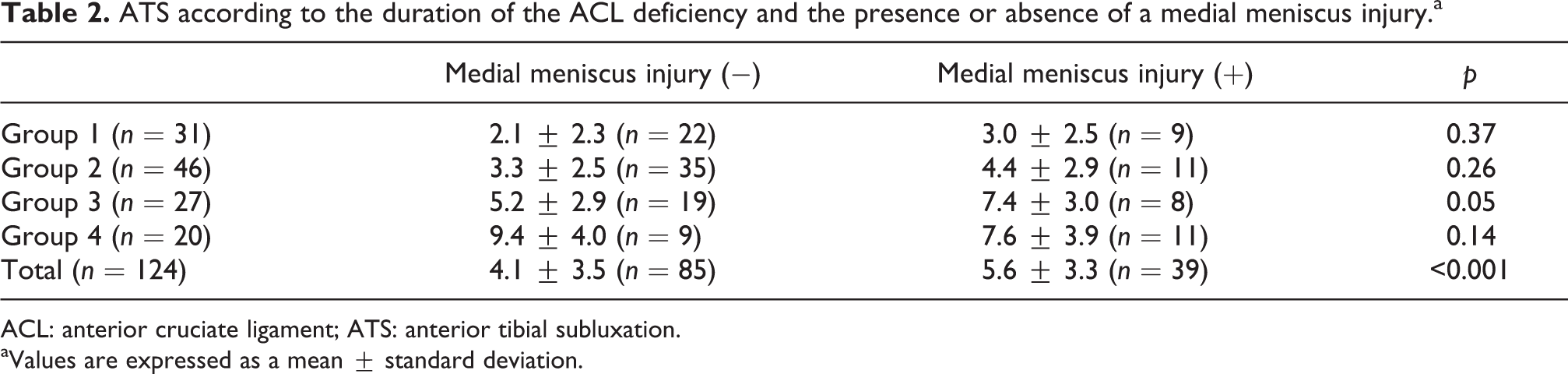
ACL: anterior cruciate ligament; ATS: anterior tibial subluxation.
aValues are expressed as a mean ± standard deviation.
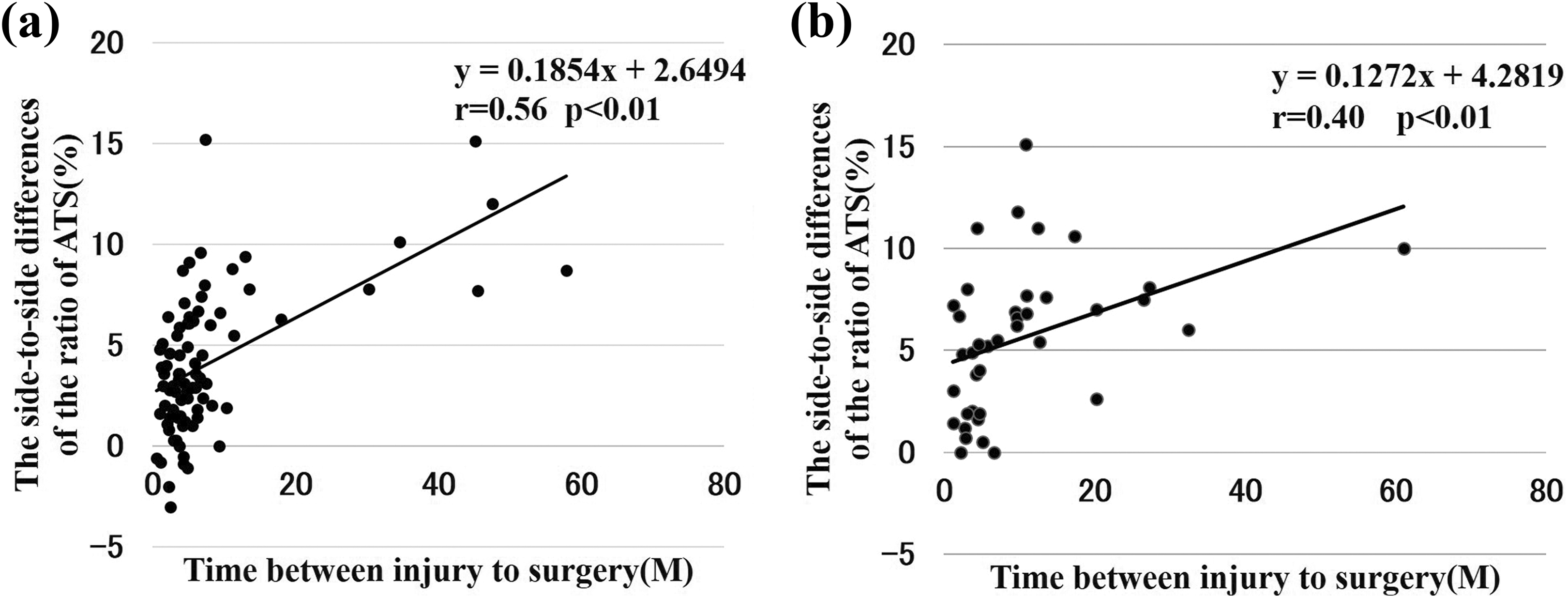
The correlation between ATS and time from injury to surgery in patients without medial meniscus injury (a) and in patients with a medial meniscal injury (b). There was a positive correlation between the side-to-side difference of the ATS ratio and the time from injury to surgery in both patients without medial meniscal injury and with a medial meniscal injury. The correlation was slightly stronger in the patients without medial meniscal injury than that in the patients with a medial meniscal injury (r = 0.56, p < 0.01, r = 0.40, p < 0.01). ATS: anterior tibial subluxation.
Correlation between the side-to-side difference of ATS
There was no correlation between the side-to-side difference of the ATS ratio and the PTS angle (r = 0.07, not significant; Figure 6).

The correlation between ATS and posterior tibial slope. There was no correlation between the side-to-side difference of the ATS ratio and the PTS angle (r = 0.07, n.s). ATS: anterior tibial subluxation.
Discussion
The present study exhibited two important findings regarding the factor affecting ATS in maximum knee extension in ACL-deficient knees. First, ATS in maximum extension increases over time in ACL-deficient knees, and the time from injury to surgery was the most significant factor affecting ATS. Second, medial meniscal injuries exacerbated ATS associated with an ACL deficiency.
Dejour et al. described anterior translation of the tibia in ACL-deficient knees on lateral radiographs for the first time. 23 They concluded that rupture of the ACL-enabled active subluxation of the tibia and that this technique is useful in diagnosis. In our study, ATS was measured using fluoroscopy. This measurement method using the fluoroscopy device was proposed by Banks et al., 18 and they reported that sagittal plane translations could be measured with an accuracy of approximately 0.5 mm. We previously followed their method to measure anterior/posterior translation during the Lachman test. 19 In the present study, we modified the measurement of ATS in maximum extension of the knee.
Almekinders et al. measured the position of the tibia relative to the femur on a lateral radiograph obtained with the knee in full extension and weight bearing. 24 They found that anterior tibial displacement was increased in patients with an ACL deficiency compared with that in those without an ACL deficiency. However, ATS in these individual patients was not clarified since they did not compare the anterior tibial position between the ACL-deficient knee and the contralateral healthy knee in each patient. Fukuta et al. compared the difference in the anterior tibial position relative to the femur in extension without external force on lateral radiographs between ACL-deficient knees and contralateral normal knees. 25 They found that ACL-deficient knees had ATS, and the extent was positively correlated with the duration of the ACL deficiency. Mishima et al. used MRI to measure the tibial position and reported ATS in ACL-deficient knees. In addition, they reported that ATS increased over time in ACL-deficient knees. 8 Consistent with these previous reports, we found increased ATS in maximum extension of the knees in ACL-deficient knees using fluoroscopy, and the extent of ATS was positively correlated with the duration of an ACL deficiency. To provide information for surgical timing of ACL-R, patients were divided into four groups depending on the time since injury to surgery. The ATS ratio in patients who had more than 6 months of an ACL deficiency was significantly higher than in those who had 6 months of an ACL deficiency. Based on these findings, it may be advisable to perform ACL-R within 6 months after an injury to avoid an increased tibiofemoral relationship in the sagittal plane since excess laxity may cause an increase in mechanical stress on the graft.
In the present study, the incidence ratio of medial meniscal injury was significantly higher in patients who underwent ACL-R more than 12 months after ACL injury (more than 50% of the patients) than in those who underwent ACL-R within 12 months after injury (about 25%). These results are consistent with those of previous reports. 26,27 Levy et al. reported that the incidence of medial meniscal injury combined with ACL injury ranged from 15% to 40%, and the incidence was higher with a long-term ACL deficiency. 26 Chhadia et al. also reported that increased time from injury to surgery was a risk factor increasing a concomitant meniscal injury after ACL injury. 27 Based on the high incidence of the medial meniscal injury and the significant increase in ATS 12 months after injury, surgeons should consider performing ACL-R within 12 months at the latest. Fithian et al. advocated that the incidence of medial meniscal injury is higher in patients with an ACL-deficient knee than in those without an ACL-deficient knee, and the ratio of a medial meniscus injury is reduced by ACL-R. 28
The role of the meniscus concerning knee kinematics becomes more relevant in the ACL-deficient knee. 10,11,29 Previous biomechanical studies have demonstrated that the medial meniscus is a secondary restraint to anterior-posterior displacement in the ACL-deficient knee. 11,30
The side-to-side difference of the ATS ratio was significantly higher in patients with a medial meniscal injury than in those without a medial meniscal injury in the current study. This finding suggests that the medial meniscus is an important structure to restrain ATT at maximum knee extension in ACL-deficient knees, which is consistent with previous reports. 11
To further assess the effect of medial meniscal injuries on ATS, the ATS ratio was compared between the patients with a medial meniscal injury and those without a medial meniscal injury among all four groups. However, the ATS ratio was not significantly different between the patients with a medial meniscal injury and those without a medial meniscal injury in any of the four groups. Therefore, these observations suggest that increased laxity of other structures, such as a medial collateral ligament and joint capsule, may be more dominant factors affecting ATS. To support this idea, the ATS ratio was positively correlated with the time since injury to surgery regardless of the presence or absence of a meniscal injury. Further investigations are needed to assess the effect of a medial meniscal injury on ATS.
The tibial slope produces an anteriorly directed shear force component when a compressive tibiofemoral load or a quadriceps muscle force is applied to the knee joint, resulting in ATT relative to the femur. This mechanism has been observed in a cadaver model, 17 as well as in living subjects. 12,14 Dejour et al. 14 reported that a steeper tibial slope resulted in a significantly greater amount of ATT in ACL-deficient and ACL-intact knees during the lateral monopedal stance test (i.e. a dynamic condition). Therefore, we hypothesized that ATS would increase in patients with a steeper tibial slope. In the present study, there was no positive correlation between the extent of ATS and the PTS angle (r = 0.07). Although this finding may be explained by the fact that the measurement in our study was performed under a static condition (maximum extension of the knee, non-weight bearing, and under anesthesia), the current study suggests that the PTS is not a main factor affecting ATS.
This study has some limitations. First, there were differences in the management protocol for post-ACL injury among patients, and the activity level was not totally controlled because most patients were treated at other hospitals before being referred to our institution. Second, this study was performed under static conditions and was limited to sagittal plane movement. Dynamic data would certainly be helpful to assess how this altered tibiofemoral relationship affects actual three-dimensional movements. Third, since an image-intensified fluoroscopic system was used in this study, distortion occurred at the marginal region of the obtained images. To reduce the distortion, images were captured at the center of the screen as much as possible. Fourth, it was not assessed how ATS in ACL-deficient knees changes postoperatively. Despite these limitations, our study provided important information: the time from ACL injury to surgery was a significant factor in ATS. Our study’s findings are clinically relevant because ACL-R should be performed within 6 months after an initial injury.
Conclusions
The present study’s results suggested that ACL-R should be performed within 6 months after injury if surgeons prefer to avoid an abnormal increase in ATS in maximum extension and at the latest within 12 months to avoid medial meniscal injury at the time of ACL-R.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.