
Abstract
Background:
The efficacy of tranexamic acid to decrease post-operative blood loss and blood transfusion is well established in literature. However, the ideal mode of administration is debatable. Limited literature has compared all the available modes of administration including intravenous (IV), topical irrigation and retrograde through drain. We hypothesized that no difference would be present in either form of administration of tranexamic acid.
Methods:
Fifty patients in four groups were enrolled for study. Group 1 received drug intravenously, group 2 had topical washing with drug before closure, group 3 received drug after closure through drain and group 4 was control that received no tranexamic acid. Post-operative blood loss, calculated blood loss, haemoglobin drop, transfusion requirements and complications were studied for all four groups.
Results:
Tranexamic acid results in lower bleeding irrespective of the mode of administration compared to control group. Total loss at end of 5 days is similar in all tranexamic acid groups irrespective of method used to deliver the drug. Calculated blood loss and haemoglobin drop was minimum for IV and in patients who were administered drug retrograde through drain. Requirement for blood transfusion was found to be lower in all tranexamic acid patients compared to non-tranexamic acid group. The requirement was highest in topical wash group among all tranexamic acid groups.
Conclusion:
We conclude that intra-articular administration through drain and IV administration are equally effective and superior to topical wash method in reducing blood loss, haemoglobin fall and transfusion requirements.
Introduction
Total knee arthroplasty stands among one of the greatest surgical accomplishments of last century. Last few decades have seen advancements in understanding of the biomechanics of the knee. This resulted in improvements in techniques and functional outcomes. With increase in number of aging population, better techniques and implants and increasing survivor ship of knee arthroplasty, the number of patients undergoing surgery is increasing. The trend appears to keep up in foreseeable future. 1 Since the surgery is elective, it becomes imperative to decrease the perioperative complications and morbidity to the patient. Intraoperative and post-operative blood loss is however an unavoidable complication of the surgery. 2 –4 Continuous efforts are taken to decease the perioperative blood loss. Use of hypotensive anaesthesia, 5 pneumatic tourniquet, fibrin glue 6 mechanical compression by clamping of the drain to produce tamponade effect 7 –10 and use of pharmacological agents like tranexamic acid have been tried. 11 –13 Among all these agents, use of tranexamic acid has been vastly studied and has shown to decrease post-operative blood loss and requirement of transfusion.
Tranexamic acid is pharmacologically an antagonist to plasminogen and thereby helps to maintain the clotting state. 14 This decreases the post-operative blood loss. Even though studies with a level of evidence we have supported the effectiveness of the drug in decreasing post-operative blood loss and requirement of blood transfusion, 15–16 the debate on ideal mode of drug administration is still not settled. The reports in literature are conflicting. The intravenous (IV) administration results in rapid diffusion of drug in the target joint cavity 17 ; a similar concentration was achieved without a wide, systemic distribution through the topical mode thereby decreasing the potential thromboembolic risks. 18 Most studies report no significant difference in IV and topical routes 16,19–20 ; some studies do report favourable result for topical administration, 21,22 while others report IV use to be associated with decrease in transfusion requirements. 23 Also among topical routes, the drug has been administered through different techniques, including tissue impregnation before knee closure 22 or delivery to the joint through the drain after closure. 21 The effectiveness of either method is not yet determined.
To the best of our knowledge, there is very little data in literature that compares all the routes of administration of tranexamic acid in a single study or that compares the two modes of topical administration. We undertook this study to find out the best route of administration of tranexamic acid to decrease blood loss and transfusion requirements without increasing any thrombotic events. We hypothesized that there was no difference in effectiveness of tranexamic acid given via IV or topical routes.
Materials and method
Patients
We performed a single institution, two centres-based double-blinded prospective randomized control trial from September 2014 to February 2015, wherein we enrolled all patients with primary osteoarthritis of the knee who were planned for unilateral conventional total knee arthroplasty. The clearance was taken from the institution review board. We excluded all patients with secondary osteoarthritis (rheumatoid and other inflammatory arthritis, post-traumatic arthritis), known allergies to tranexamic acid, major comorbidities, coagulopathies (International Normalised Ratio [INR] > 1.4), previous history of stroke or severe ischaemic cardiopathy and patients undergoing bilateral total knee arthroplasty. There were total of 200 patients who were enrolled for the study. Informed consent was taken from all patients.
These patients were randomly divided into four groups
Group 1 patients were planned for IV tranexamic acid transfusion. The drug was administered in dose of 10 mg/kg 20 min before tourniquet application as a preoperative dose, 10 mg/kg 15 min before deflation of the tourniquet as an intraoperative dose and 10 mg/kg 3 h after the second dose as a post-operative dose. 23 As placebo, the group received topical wash with 50 ml of saline after surgery and 50 ml of saline retrograde through drain.
Group 2 were planned for topical tranexamic irrigation with 3 g of drug in 50 ml of saline directly applied to joint cavity for 5 min just prior to closure, and as placebo, it was given 10 ml of IV normal saline in doses similar to IV group and 50 ml of saline retrograde through drain after closure. 24
Group 3 was administered 3 g tranexamic acid in 50 ml of saline retrograde through the drain after wound closure, and as placebo, it was given 10 ml of IV normal saline in doses similar to IV group and topical wash with 50 ml of saline before closure. 20
Group 4 was the control group who did not receive any tranexamic acid. This group was given as placebo 10 ml of 0.9% normal saline solution in doses similar to IV group and also received topical wash with 50 ml of saline after surgery and 50 ml of saline retrograde through drain after closure as placebo.
None of the patients were lost to follow-up and each group had 50 patients. The surgical drain was used in all cases and was clamped for 30 min.
All patients had all routine investigations, a preoperative anaesthetic assessment prior to surgery.
Operative technique and post-operative management
Independent statistician prepared patient assignment and placed it in sealed envelopes, which were opened just before surgery by a non-scrubbed nurse. Anaesthesiologists who were not involved in patient care prepared the study medication and placebo. The study medication and placebo were identical in appearance. Patients and surgeons participating in treatment and evaluation were blinded to the group allocation throughout the study period.
All the surgeries were performed by the two senior surgeons under spinal or general anaesthesia. All patients received 1 g of cephazolin as prophylactic antibiotic just before surgery. Pneumatic tourniquet with a mean pressure of 280 mm of mercury was used in all cases after exsanguination with an Esmarch bandage. Midline medial parapatellar approach was used in all cases. Intramedullary alignment was used to take distal femoral valgus cut, and this hole was blocked through a bone plug at end of surgery to prevent any further intramedullary blood loss. Lateral meniscus was excised using a cautery to prevent later bleeding through the genicular artery. The artery was itself cauterized when found during surgery. All case received posterior stabilized type implant and patellar resurfacing was not done in any case. Tourniquet was deflated only after wound closure in all the cases. A single drain in suprapatellar pouch was used. A continuous femoral nerve catheter was left in situ for post-operative pain management. Foleys catheter and compression bandage were removed on day 1, and patients were encouraged for muscle-strengthening exercises and walker-assisted walking. The Deep Vein Thrombosis (DVT) prophylaxis was given on case-to-case basis based on preoperative evaluation of DVT risk. The drains were emptied everyday, and the amount of drained blood was measured. The drains were removed only when this amount of emptied blood was less than 100 ml for a 24 h period. On an average, drains were kept for 3 days (2–5 days). This has been our institution policy, as we have observed that removal of drains at one selected time may not work in all the cases. Some cases have collection for longer time periods and early removal in such cases not only may cause erroneous lower recordings of drained blood but also has a risk of haematoma formation.
All patients were discharged at 2 weeks immediately after suture removal.
Clinical evaluation
Post-operative blood loss was evaluated as immediate post-operative loss (days 0 and 1), delayed post-operative loss (days 2–5) and total loss in the drain that was inserted during surgery. Calculated blood loss was calculated through Gross formula based on estimated blood volume and haematocrit drop. 25 The lowest haematocrit value after surgery was taken into consideration for calculation of blood loss. Nadler’s formula was used to calculate the estimated blood volume. 26 Post-operative haemoglobin and haematocrit were measured immediately after surgery, on post-operative days 1, 2, 3, 5 and 7 and post-operative day 14, and were compared to preoperative values taken 2 weeks prior to surgery. Requirement of blood transfusion was observed in all the groups as immediate (days 0 and 1) and delayed post-operative transfusion (days 2–5). The criterion for transfusion was taken as post-operative haemoglobin value of less than 8 mg/dl. All the groups were studied for any significant difference in post-operative complication rate in terms of deep vein thrombosis, pulmonary embolism, infection, readmission rates and hospital stay. Patients were followed for 3 months for development of any of the above complications. Ultrasound Doppler and computerised Tomography (CT) angiography were performed in patients with clinical suspicion of DVT based on clinical evaluation. Mechanical prophylaxis for DVT using DVT pumps was used in all cases. Pharmacological prophylaxis with molecular weight heparin was used only in high risk cases. Owing to a lower incidence of DVT in Asian population compared to Western literature, a routine use of pharmacological prophylaxis was not warranted. Patients were also observed for any excessive swelling in calf or thigh area, any ecchymosis or bruising at surgical site and any wound-related complications including wound dehiscence or blister formation in all groups. Patients were advised to immediately report to emergency in case of any warning signs of DVT or infection.
Statistical analysis
The quantitative variables were expressed in terms of means ± standard deviation. Any significant difference in means was evaluated using analysis of variance (ANOVA) and Tukey’s post hoc for continuous outcome variables (blood loss, drop in haemoglobin, functional scores or age) and χ 2 test for binary outcome variables (requirement of blood transfusion or presence or absence of complications), and p-value of less than 0.05 was considered significant. SPSS software version 20 (SPSS for mac, International Buisness Machine [IBM], New York, USA) was used to carry out statistical analysis.
Results
There were total of 200 patients operated with unilateral total knee arthroplasty during our study period. All groups had 50 patients. There were 24 males and 161 females in our series with no statistical significant difference in any group. The average age in group 1 was 70.2, group 2 was 71, group 3 was 68.6 and group 4 was 68.3, which were not found to be statistically significant (p = 0.47). All patients belonged to same ethnic group and were Asian in origin with no significant difference in height, weight or Body Mass Index (BMI). All the four groups were thereby equally matched in terms of patient factors. The average preoperative haemoglobin in group 1 was 12.3, group 2 was 12.7, group 3 was 12.5 and control group was 12.5 with no statistical difference (p = 0.76). There were no difference in preoperative deformity or preoperative functional scores (WOMAC and KSS scores). The intraoperative blood loss in all four groups was negligible. The time for drain removal in all groups was 3.1 days, 3.3 days, 3.2 days and 3.1 days, respectively, and was not found statistically significant (p = 0.88). Also, there was no statistical difference in mean surgical time of any group.
Comparison of blood loss through drain – Evident loss in four groups
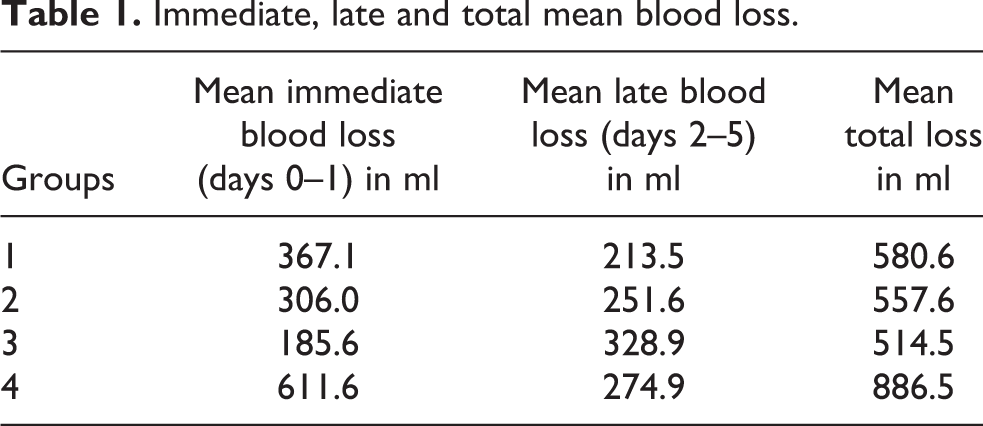
The early post-operative blood loss (days 0–1), late losses (days 2–5) and total drain loss are shown in Table 1. The results of difference of means of ANOVA are shown in Table 2.
Immediate, late and total mean blood loss.
ANOVA test showing significant difference in means.

ANOVA: analysis of variance.
The mean blood loss through surgical drain was significantly higher in control group than all other groups (p = 0.000). Group 3 – retrograde administration through drain group – showed the least immediate blood loss (days 0–1) compared to other tranexamic acid group. The difference was statistically significant compared to group 1 (IV group; p = 0.000) but not statistically relevant compared to group 2 (topical wash group; p = 0.07).
However, group 3 which had least blood loss immediately after surgery had a highest mean blood loss from day 2 onwards. This was significantly higher than IV tranexamic group (group 1; p < 0.05). This implied that even though the blood loss on day 1 may be less in topical group, these tend to bleed more after day 1. Similarly, topical wash group had a mean loss higher than the IV group but was not statistically significant (p > 0.05).
Also, interestingly, total loss through drain at end of 5 days was not statistically different among various tranexamic acid group patients (p > 0.05) but was significantly less than control group patients (p = 0.000).
Comparison of calculated blood loss
Blood loss calculated through Gross formula was found to be highest in control group of 1610 ml (p = 0.000) compared to all other groups. Group 1 (IV group) and group 3 (retrograde administration through drain group) had least calculated loss of 1131 ml and 1182 ml, respectively. Topical wash group – group 2 – had statistically significant higher loss of 1280 ml than other tranexamic acid groups (p = 0.01 with group 1 and p = 0.03 with group 3).
Comparison of drop of haemoglobin levels in four groups
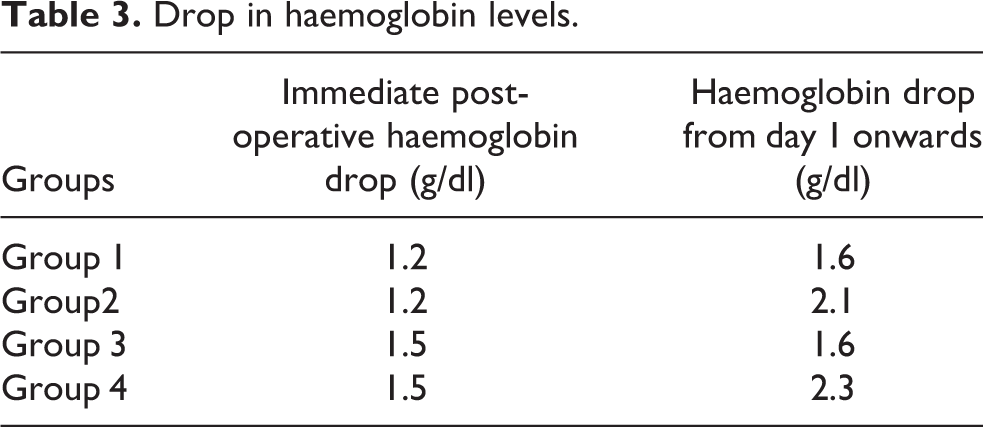
The immediate and day-2 drop in haemoglobin is shown in Table 3, and the p-value of ANOVA is given in Table 4.
Drop in haemoglobin levels.
ANOVA test results showing significance in difference of means in haemoglobin drops among different groups.
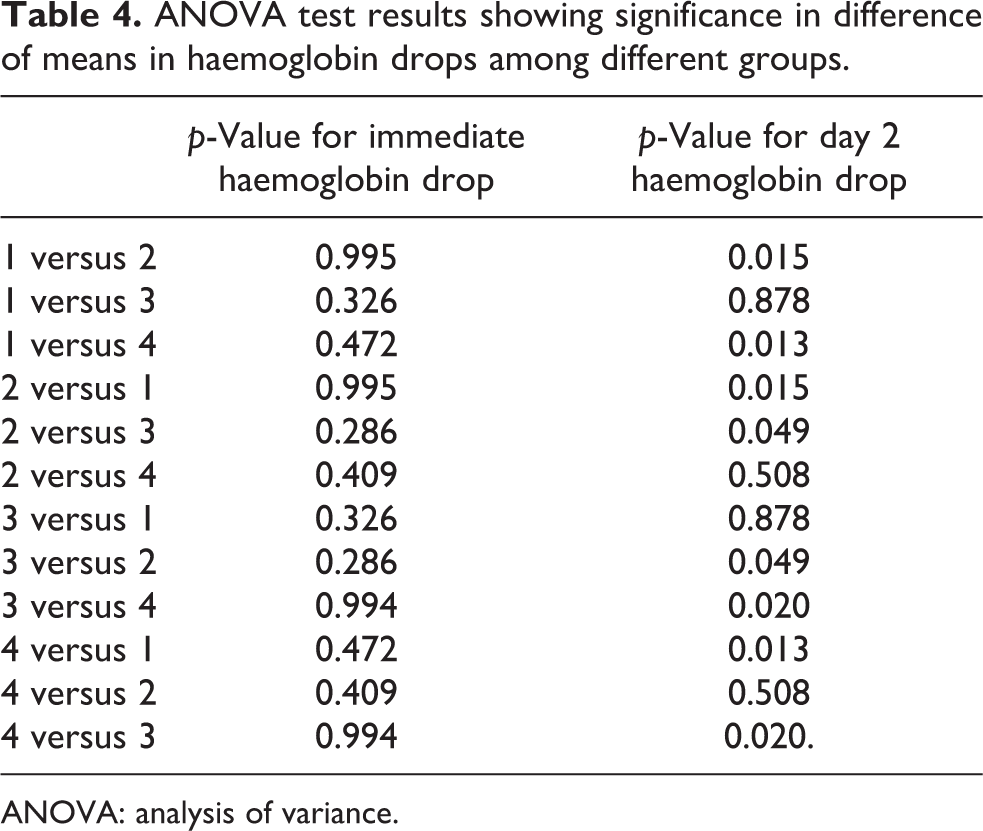
ANOVA: analysis of variance.
There was no statistical difference in any of the groups for haemoglobin drop measured immediately after surgery within 2 h. However, IV group (group 1) and ‘retrograde administration through drain’ group (group 3) were most effective to prevent haemoglobin drop measured subsequently after surgery with p-value less than 0.05 compared to control group and topical wash group (Table 4). The drop in topical wash group was less than the control group but it was not statistically significant (p > 0.05)
Comparison on requirement of blood transfusion in four groups
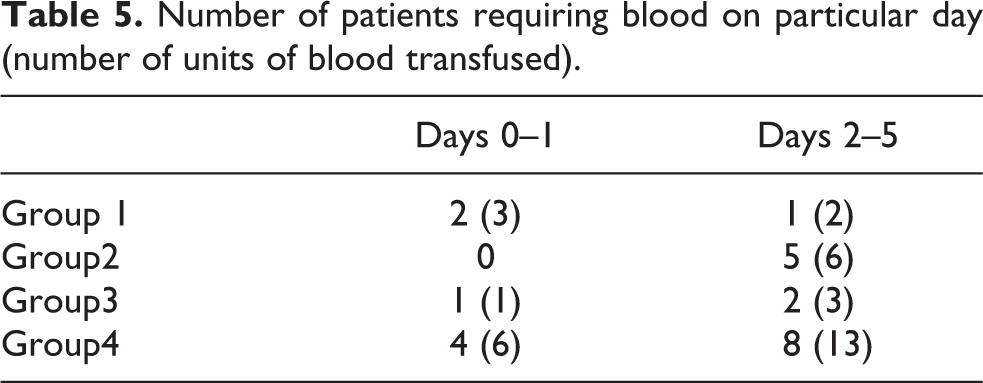
Requirement for blood transfusion was higher for control group compared to any tranexamic acid group, and the value was statistically significant (p < 0.05; Table 5). There was, however, no statistically significant difference among patients in different tranexamic acid groups in overall requirement of blood transfusion. Among tranexamic acid group patients, the requirement was maximum in topical wash group but was not statistically significant (p > 0.05).
Number of patients requiring blood on particular day (number of units of blood transfused).
There was no difference in incidence of studied complications in any group. One patient each in control group and topical wash group had a symptomatic DVT diagnosed on Doppler ultrasonography which was managed medically. None of the patients had pulmonary embolism. No wound-related complications were observed in any group.
Discussion
Our study shows that tranexamic acid results in lower bleeding irrespective of the mode of administration compared to control group. The important finding of our study was that the group in which drug was administered through drain at end of surgery resulted in least post-operative bleeding in first 24–36 h but this group tends to bleed more compared to IV group on subsequent days. However, the results of total loss at end of 5 days are similar in all groups irrespective of method used to deliver the drug. Calculated blood loss was minimum for groups 1 and 3, which appeared to be better that topical wash method. Haemoglobin drop was least in group 3 (retrograde administration through drain group) and group 1 (IV group) but topical wash group failed to show any significant effectiveness in preventing haemoglobin drop. Requirement for blood transfusion was found to be lower in all tranexamic acid patients compared to non-tranexamic acid group. The requirement was highest in topical wash group among all tranexamic acid groups.
Blood loss is an important unavoidable complication of total knee arthroplasty. 1 The average loss may be from 500 ml to 2 l resulting in a haemoglobin drop of 4 ± 1.5 gm/dl. 2 –4 This bleeding is the source of major morbidity causing swelling, stiffness, arthrofibrosis, oozing through the wounds, delayed rehabilitation and allogeneic blood transfusions. The risk of allogeneic blood transfusion is 4–46% after knee arthroplasty in various studies. 27 Blood transfusion results in transfusion-related immunomodulation decreasing post-operative immunity and increasing the chances of infection. 28 Also, transfusion has a risk of disease transmission- and transfusion-related reactions. This has led to development of numerous blood saving strategies including hypotensive anaesthesia, tourniquet application, tissue haemostasis using fibrin flue, post-operative drain clamping, heavy bulky Robert Jones bandages and pharmacological agents like tranexamic acid. 4 –11
The effectiveness of tranexamic acid in reducing blood loss is well established in world literature. A recent meta-analysis by Alshryda et al., which included nine randomized controlled trials in Total Knee Replacement (TKR), revealed that tranexamic acid significantly reduced the rate of blood transfusion, without an increase in the incidence of thromboembolic events. 16 However, despite so much work, the mode of administration remains a dilemma with conflicting reports.
None of the reports published mentions difference in early and late post-operative blood loss. We found that topical groups bleed less on first 2 days followed by more blood loss in following days compared to IV group with ultimately no difference in blood loss. Sarzaeem et al. found that the mean losses were lowest in intra-articular group. 29 However, the authors have routinely removed the drain at 48 h. Similarly, Hamlin et al. 21 and Seo et al. 22 found topical irrigation results to be better than IV results. But these authors have measured blood loss as drain outputs that were routinely removed after 24 h. We believe that this difference of results from our study is due to routine removal of all drains at 24–48 h. This may have erroneous lower readings in few patients who may continue to have blood loss after that period. Similar to their findings, we also found that bleeding in topical groups was less in first 24–48 h compared to IV group. However, their study does not mention about any loss after that period wherein we found that intra-articular group had bled more. Ultimately, no difference in total blood loss was found in our study. Similar to our results, Gomez-Barrena et al. measured both visible and invisible losses and have found no significant difference in intra-articular and IV groups. 19 Similarly, most of other authors when have measured blood losses as calculated loss have found no difference in IV and intra-articular administration of tranexamic acid. 18,20,30
Among three methods of administration, we found no statistical difference among intra-articular administration retrograde through drain at end of surgery and IV method. However, both these methods were found superior to topical wash method in terms of total calculated blood loss and haemoglobin drop. This finding has been shared by other authors in literature as well. 23,29 Contrary to our results, Soni et al. 30 and Wong 24 have found topical wash equal or superior to IV methods. However, this difference may be due to single IV tranexamic acid dose used by them. We believe that since fibrinolytic response after surgical trauma is known to be biphasic with an increased activity during the first 3 hours, followed by a shutdown that peaks at about 24 h, a single intraoperative dose may not be sufficient. Maniar et al. have showed that three-drug regime is superior to single intraoperative dose. 23
Blood transfusions were significantly less in tranexamic acid group compared to control group, and the data is largely supported in world literature. 11 –13,15,16,19 However, among tranexamic groups, no overall difference in transfusion rates was seen among intra-articular administration through drain or through topical wash, a finding similar to that of Patel et al.,20 Seo et al.22 and Soni 30 et al. The IV group had higher blood requirements on days 0 and 1; however, the topical group required more transfusions in subsequent period. However, no statistical significance was found in this correlation. This requirement of blood transfusion, however, almost mirrored the results of haemoglobin drop and blood loss in our study. However, we cannot compare this data to other literature, as we did not find any reports mentioning the timing of transfusion after surgery.
Between both topical groups, we found that intra-articular administration retrograde through drain at the end of surgery was better compared to topical wash during surgery in terms of preventing the haemoglobin fall.
We understand the shortcomings of our study. Firstly, the study size is not large enough to make any concrete conclusions along with a female predominance of the study group; female predominance is a feature of most studies from this region, and it was not possible to control this parameter. Secondly, as two different surgeons performed surgeries, the surgical technique by itself might be a confounding factor in assessing the blood loss. Thirdly, we also did not include patients who underwent simultaneous bilateral TKA in the present study, and therefore, our conclusions may not apply to these patients. Fourthly, no blood studies have been carried out to estimate serum Tranaxamic acid (TXA) levels following TKA, and thus, no information regarding the toxicity related to TXA can be retrieved. Lastly, the present study has not addressed the subjective knee function score of the patients after TKA, as the main purpose of this study was to evaluate the ideal mode of administration of drug.
Conclusion
Tranexamic acid is an effective way to reduce blood loss and transfusion requirements in perioperative period given through any of the described method. We conclude that intra-articular retrograde administration through drain and IV administration are equally effective and superior to topical wash method in reducing blood loss, haemoglobin fall and transfusion requirements
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.