
Abstract
A successful Total knee arthroplasty (TKA) procedure requires restoration of mechanical axis and soft tissue balancing. Deformity of tibia and femur occurs with history of trauma or osteotomy, infection, metabolic bone disease and excessive bowing. Tackling pre-existing extra-articular deformity of lower limbs during total knee arthroplasty can be challenging due to difficulty in restoring alignment axis and soft tissue balancing. We have recorded 6 patients underwent total knee arthroplasty with preexisting extra-articular femoral deformity by intra-articular correction from 1995 to 2017. All patients had extra-articular deformity of the femur due to fracture malunion which were treated either conservatively, plating or intra-medullary nail. Coronal deformity is corrected from an average of 15.5 degrees to 4.6 degrees from neutral axis. Sagittal deformity is corrected from average of 6.8 degrees to 3.6 degrees. One patient developed progressive genu recurvatum at 7 years follow-up with range of motion at 25 degrees extension and 110 degrees flexion. The average pre-operative Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score was 68.5 (range 51−87) decreased to 50.7 (range 21–71) at 12 months post-operative and Knee score averaged 53.3 (range 51–55) increased to an average of 88.5 (range 82–94). There was only one revision for aseptic loosening 16 years after total knee replacement (TKR) and no other cases of radiological sign of aseptic loosening. In conclusion, Intra-articular correction of an extra articular femoral deformity for TKR is an attractive approach in mild to moderate deformity further from the knee joint.
Introduction
Total knee arthroplasty (TKA) has been a revolutionary procedure to relieve pain, restoring function in patients with primary or secondary knee osteoarthritis.
A successful TKA procedure requires restoration of mechanical axis and soft tissue balancing. Deformity of tibia and femur can occur with history of trauma or osteotomy, infection, metabolic bone disease and excessive bowing. Deformities of the lower limb can be in different plane includes coronal, sagittal, rotational and combined deformity. Tackling pre-existing extra-articular deformity of lower limbs during TKA can be challenging, mainly due to difficulty in restoring alignment axis and soft tissue balancing.
Classical options including (1) two stages procedure; correction osteotomy of the extra-articular deformity and subsequent TKA after union of osteotomy. (2) Simultaneous correction osteotomy of deformity at the time of TKA as single stage and (3) Intra-articular bone resection and soft tissue release to correct extra-articular deformity.
Wang and wang 1 performed intra-articular correction of an extra-articular deformity in 15 patients with satisfactory results and suggested it is an effective procedure for extra-articular varus deformity of < 20 degrees in femur and < 30 degrees in tibia in coronal plane.
Surgical considerations
The goal of restoring neutral mechanical alignment is by creating bone cut perpendicular to mechanical axes of both femur and tibia. In order to determine the axis of the lower limb, standard full-length anterior-posterior (AP) radiograph is required. Alghamdi et al. 2 reported over 50% of tibial deformity were not detected and therefore full-length anterior-posterior (AP) radiograph is essential. Pre-operative planning with full length in neutral rotation can determine the amount of bone cut required to restore mechanical alignment.
Coronal deformity can be determined by mechanical axis deviation (MAD- line drawn from centre of hip to centre of ankle). With centre of knee falls medial to MAD, valgus alignment is present and varus alignment if knee falls lateral to MAD. To determine whether the deformity is originated from femur or tibia, lateral distal femoral angle (LDFA) and medial proximal tibial angle (MPTA) is measured. (Figure 1) For femoral deformity and tibia deformity, the LDFA and MPTA will fall out of the normal range of 85–90 degrees respectively. 3
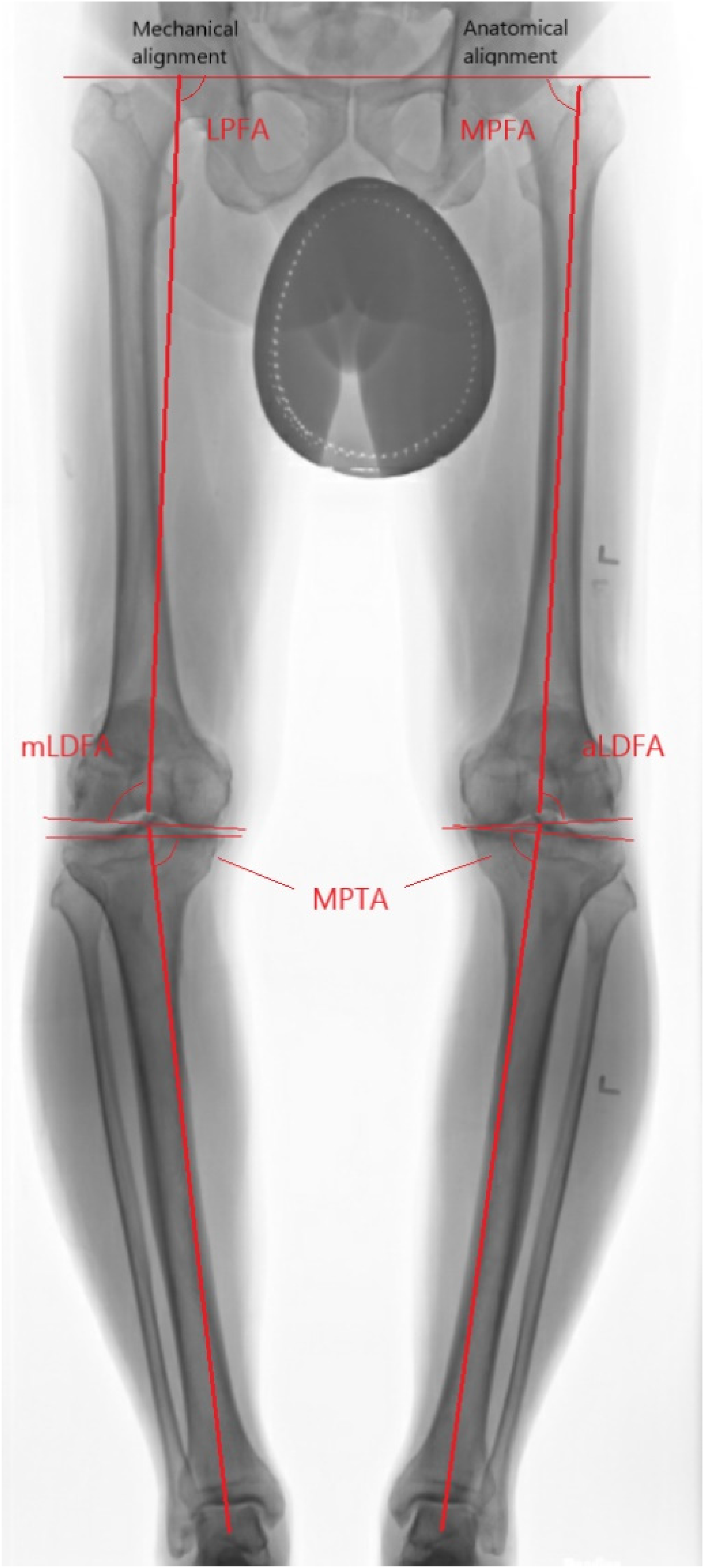
Lower limb alignment.
Wolff et al. 4 has conducted an analysis on the bone cut when deformity in femur and tibia at various level. They found that the closer the deformity to the joint, the greater impact the deformity has on the orientation of the resection. For instance, a deformity in the proximal femur has minimal on the joint line whereas a same degree of deformity at supracondylar region will require a large intra-articular compensatory wedge to produce a bone cut perpendicular to the mechanical axis. (Figures 2–7)
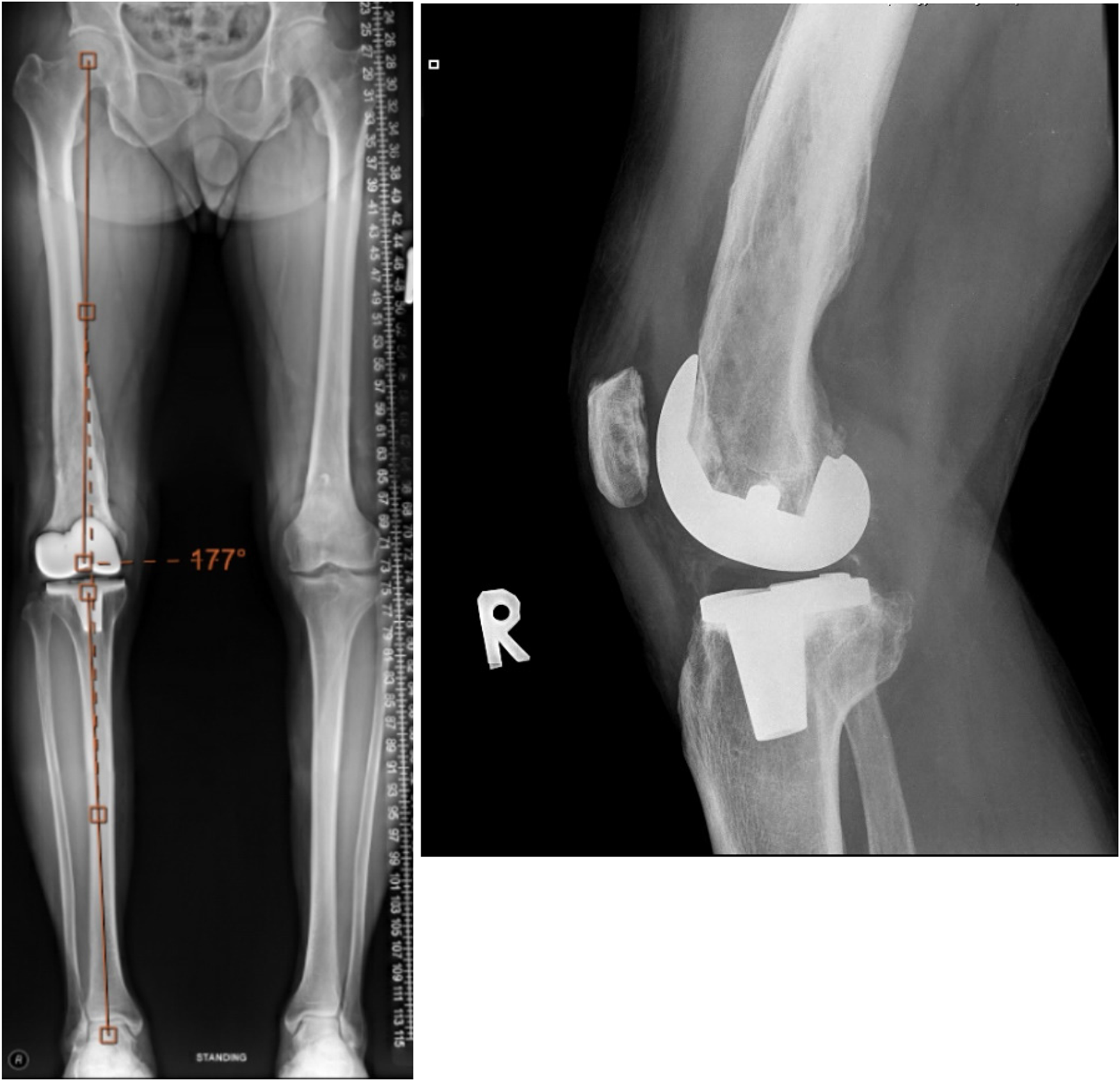
Post-operative radiograph.
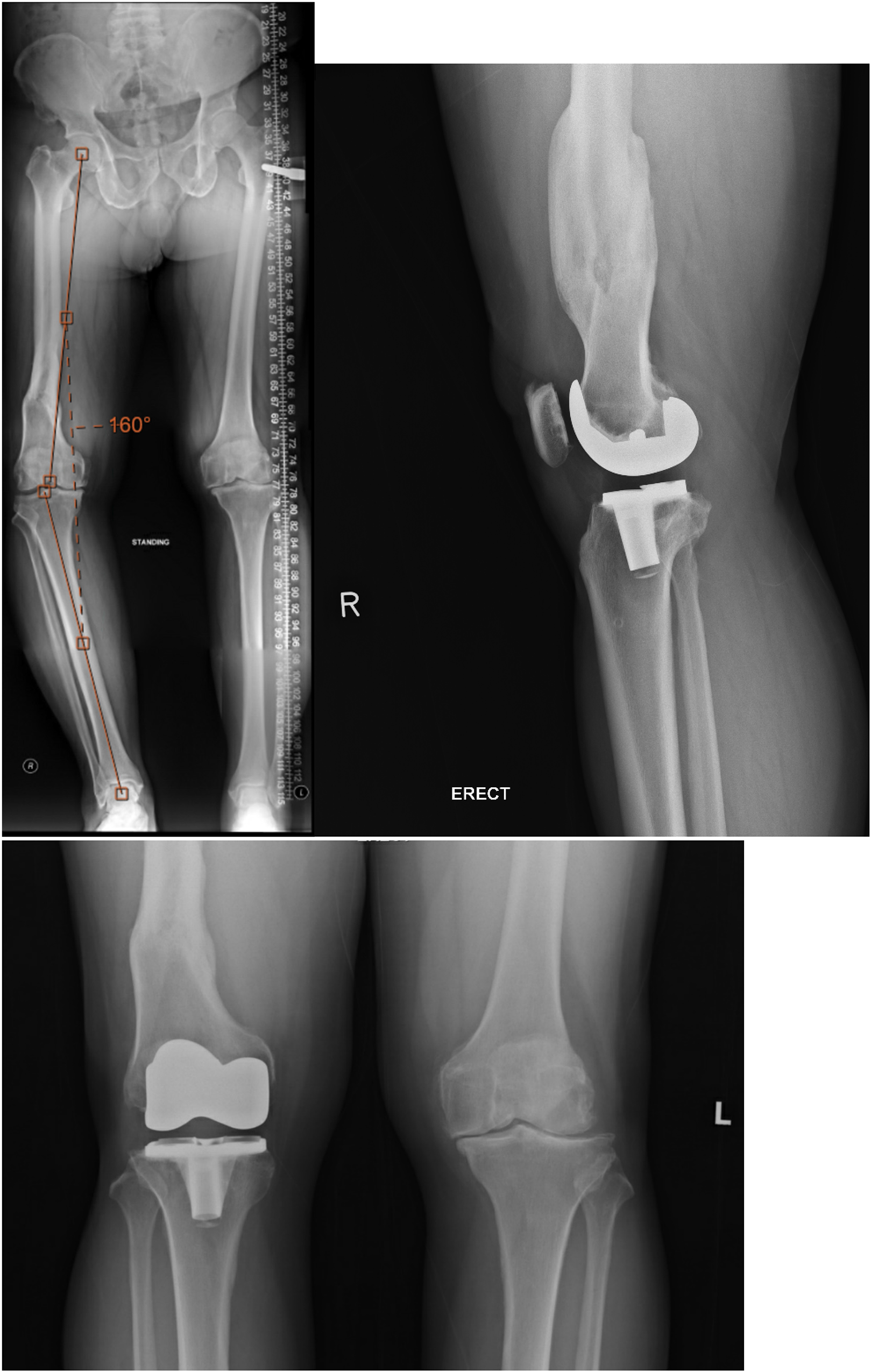
Pre-operative and post-operative radiograph.
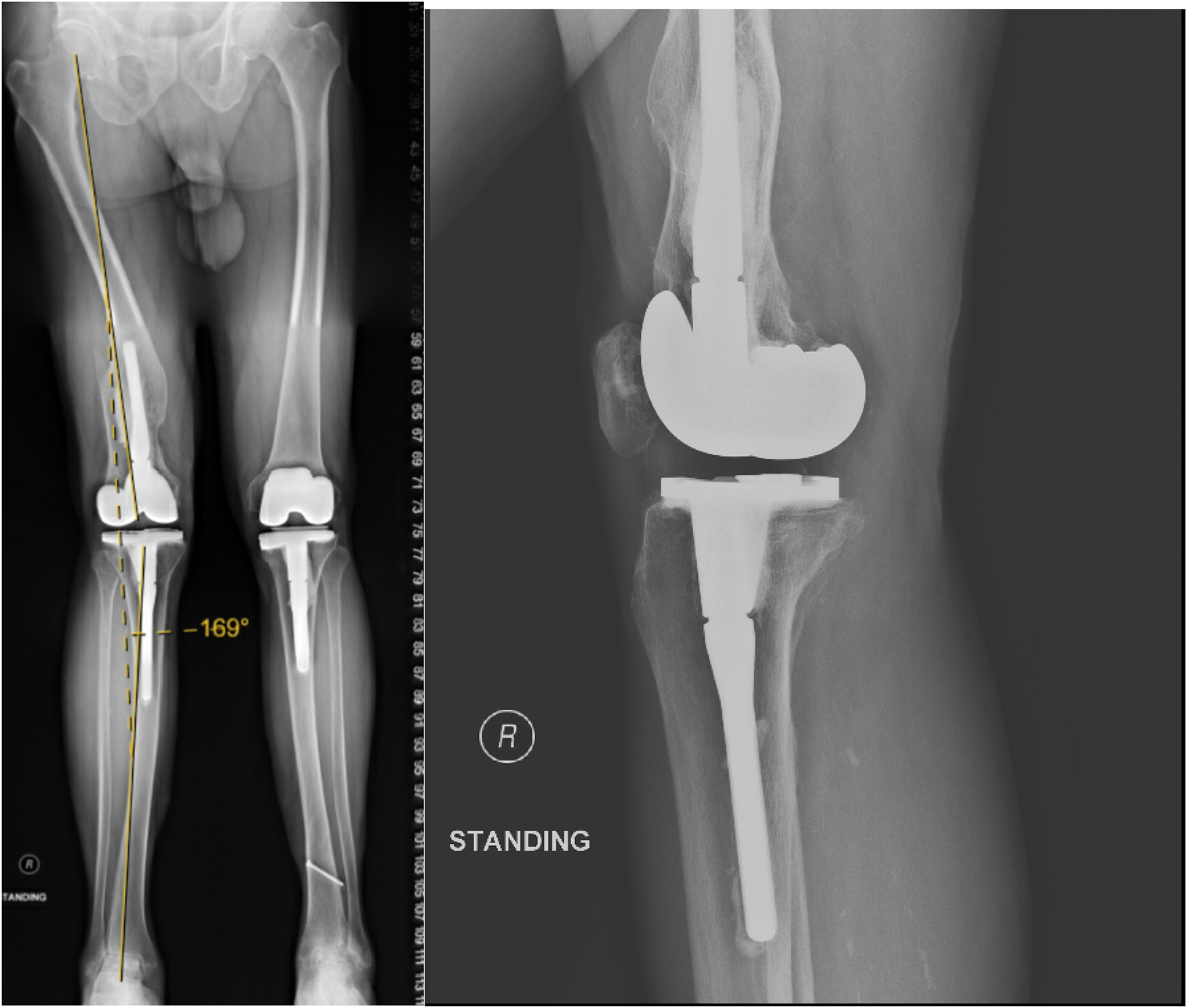
Post-operative radiograph.
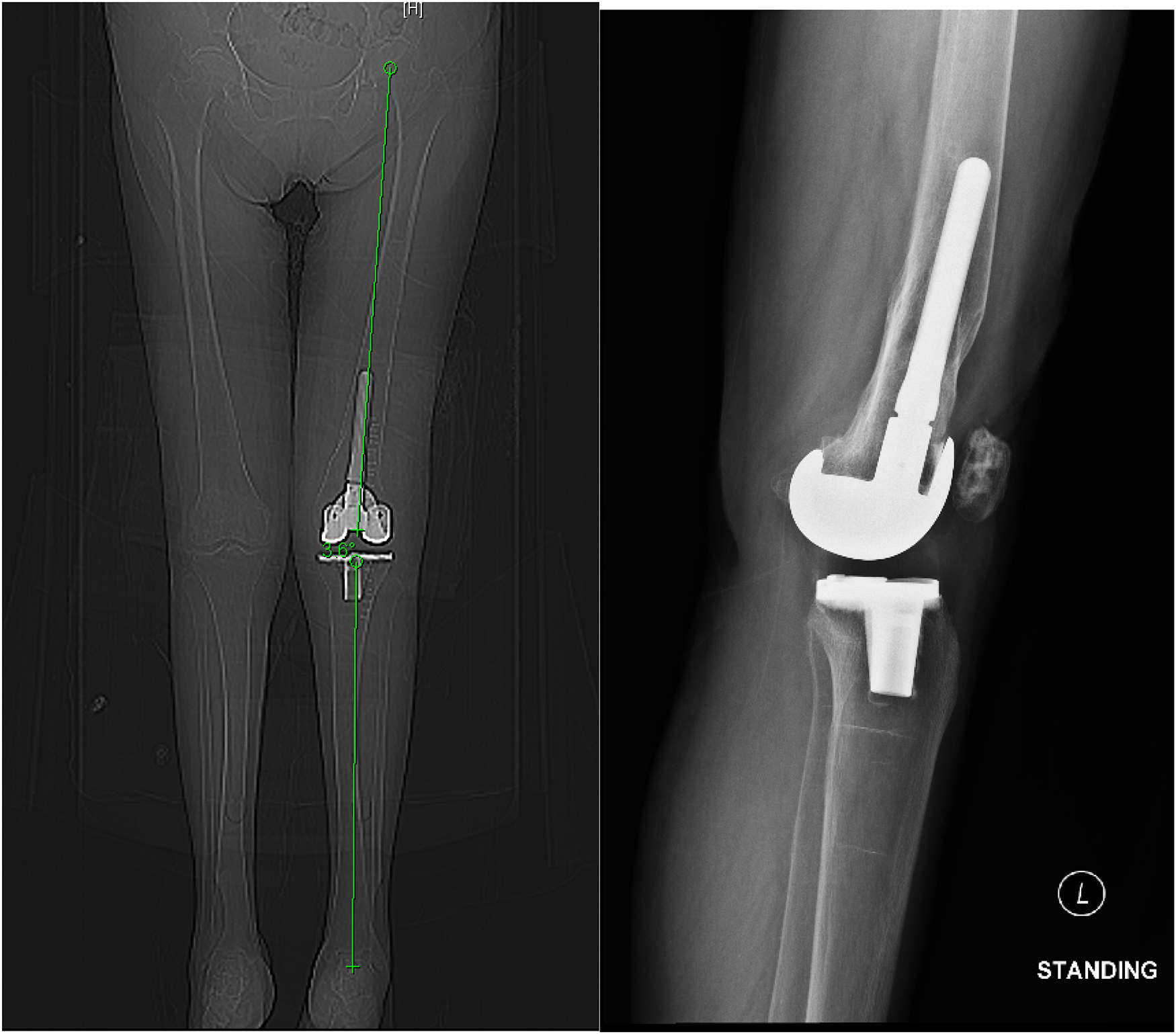
Post-operative radiograph.
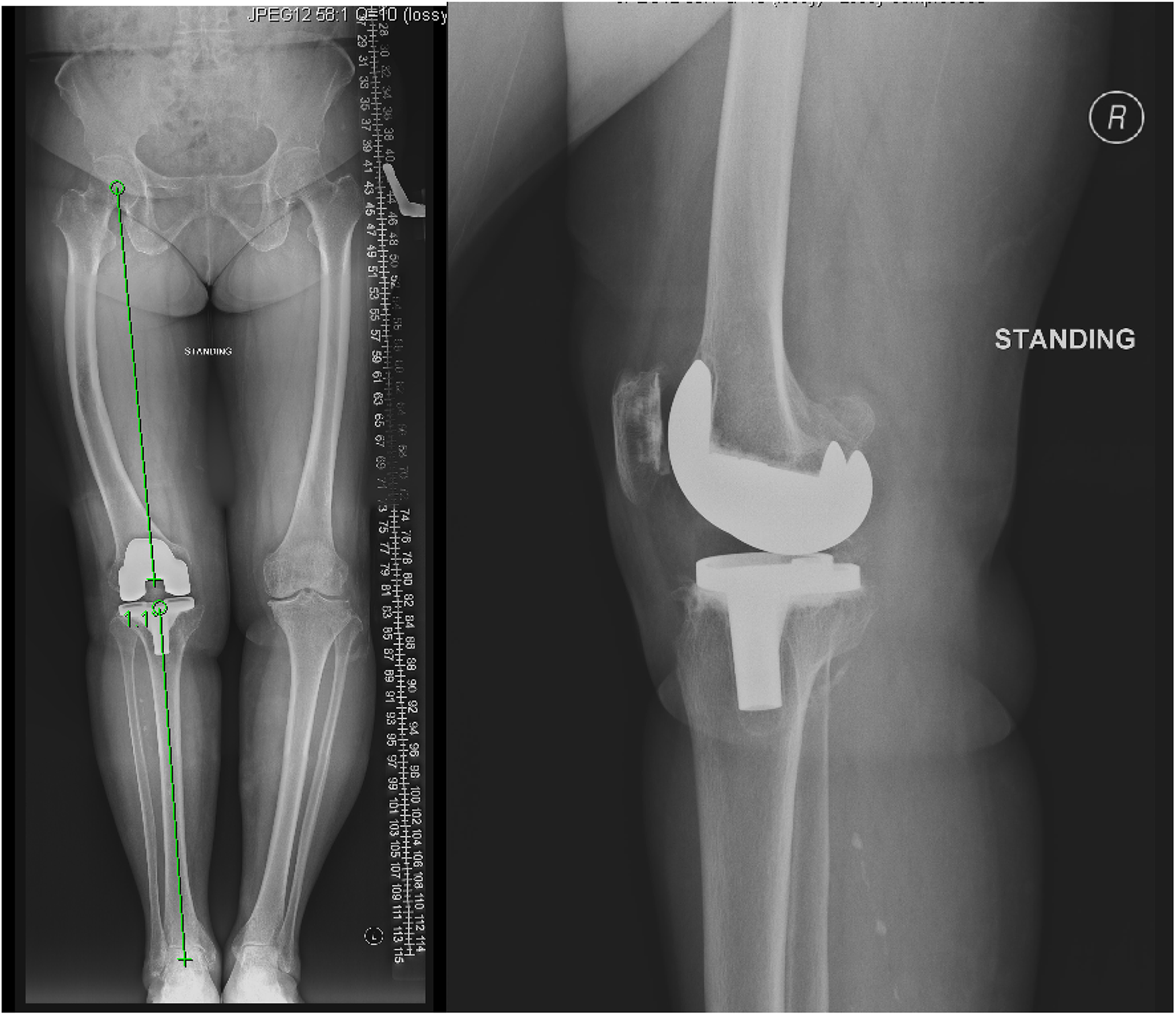
Post-operative radiograph.
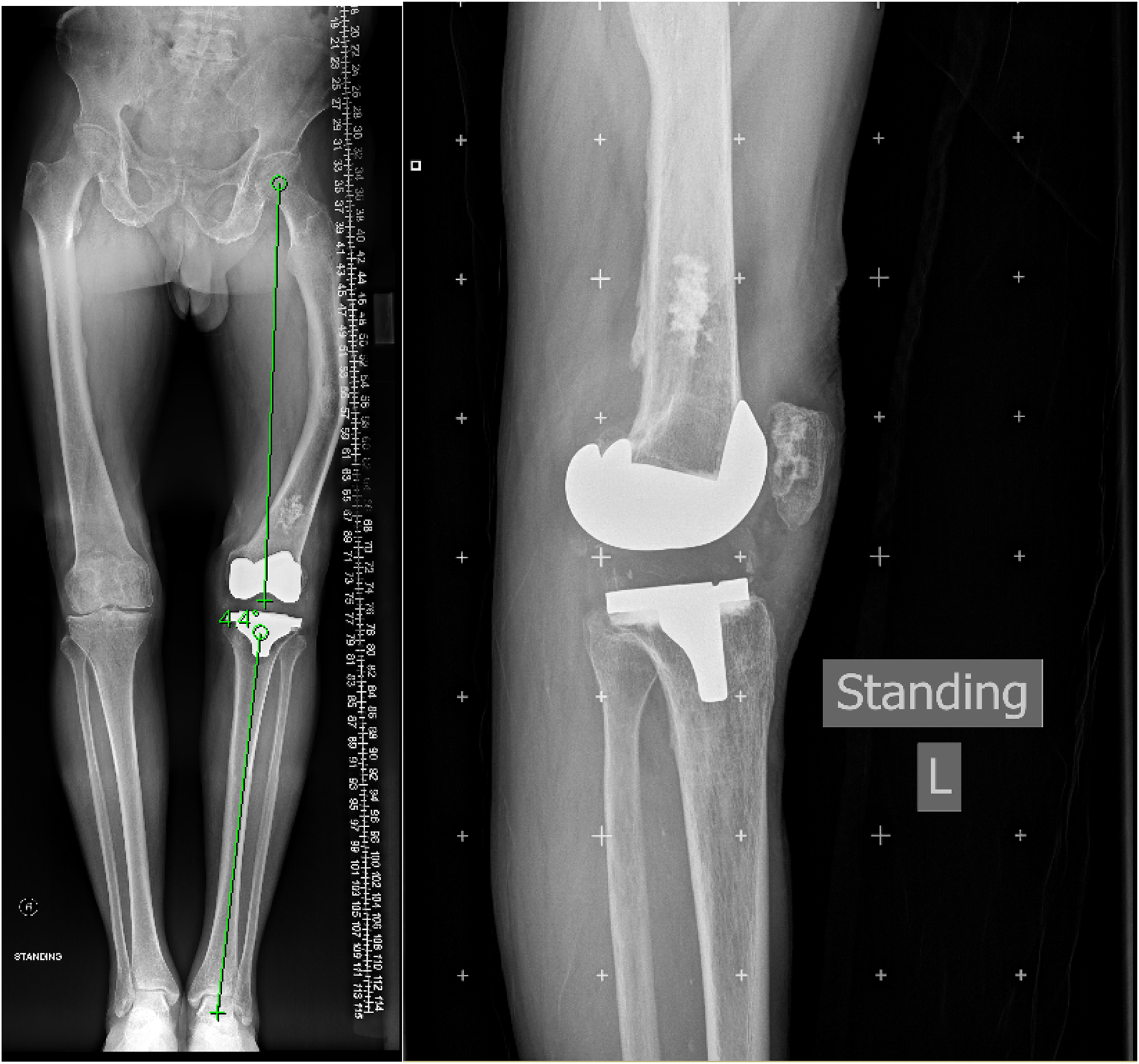
Post-operative radiograph.
Another concern with intra-articular wedge osteotomy is that unequal collateral ligament laxity will be produced. With a bone cut oblique to original joint line and insertion of collateral ligaments remains unchanged, an asymmetrical functional lengthening of collateral ligaments will be expected. Femoral varus deformity will result in removal of more lateral femoral condyle than medial femoral condyle and laxity of lateral gap. Femoral valgus femoral deformity will result in removal of more medial femoral condyle than lateral condyle and ligamentous lengthening of medial soft tissue structures. This implicate a valgus deformity is more surgically challenging as medial laxity is less well tolerated than lateral laxity. In addition, the above gap laxity is at extension only which would not be present at 90 degrees of flexion. The difference in gap laxity between flexion and extension and makes balancing even more difficult. Same principal applies to tibial varus and valgus deformity. However, in contrast to femur, the ligamentous imbalance is throughout the full range of motion after tibial bone cut whereas ligamentous imbalance is primarily in extension after femoral bone cut.
Collateral ligaments insertion to femur and tibia approximately 25 mm from articular surface. If this planned bone cut will violate the insertion of collateral ligaments, a corrective osteotomy should be considered according to Wang et al. 1 Pre-operative planning is essential to determine the planned bone cut. To assess whether an extra-articular deformity can be corrected by intra-articular osteotomy, a perpendicular line to a line from centre of femoral head to centre of knee should be drawn. This is the imaginary osteotomy line of distal femur. If this line does not cross the insertion of collateral ligament, an intra-articular correction is indicated. This also applies to tibial extra-articular deformity. If a line drawn along mechanical axis of tibia distal to the deformity intersect pass between the tibial condyles, an intra-articular osteotomy can be used to correct an extra-articular deformity of tibia.
Case reports
Between 1995 and 2017, we have recorded a total of 6 patients underwent TKA with pre-existing extra-articular femoral deformity. There were 4 male patients and 2 female patients. Their average age was 71 years old (range, 61 to 81) at the time of operation. All 6 patients had extra-articular deformity at middle to distal third of femur owing to fracture malunion which was treated either conservatively, open reduction and internal fixation by plating and closed reduction and intra-medullary nail. All patients had biplanar deformities involving the coronal and sagittal planes. The coronal deformity ranges from 14 degrees valgus to 28 degrees varus and sagittal deformity ranges from 8 degrees recurvatum to 22 degrees procurvatum. The hip–knee–ankle (HKA) angles were measured by standard method with an average of 4.5 degrees varus with a range from 20 degrees varus to 28 degrees valgus. Weight bearing full length scannogram of AP view and lateral views were obtained for pre-operative planning and pre-operative computed tomography computed tomography (CT) scan was performed in one case. All operations were performed by senior Orthopaedic specialist under Joint and Reconstruction team. A standard medial parapatellar approach were employed in all cases. Three cases adopted navigation system and three cases adopted conventional guided cutting jig. In the conventional guide group, all femoral guides were intra-medullary, and the cutting angles were adjusted according to preoperative drawing. Two cases employed extra-medullary tibial guide and remaining one employed intra-medullary tibial guide. Two cases (2 and 6) require extensive medial soft tissue release including deep medial collateral ligament (MCL), posteromedial corner and up to 7 cm of superficial MCL release while in the case with valgus deformity posterolateral release including ilio-tibial band, posterolateral corner and partial release of popliteus tendon were required. Case number 4 required removal of implant (retrograde intra-medullary femoral nail) at the time of surgery. All implants were cemented posterior stabilised design. No bone graft was required in all cases. Operative time was averaged 109 min (range 100 min to 200 min).
Follow-up period averaged 118 months (ranged 41 to 303 months).
The average post-operative HKA angle was 0.18 degrees valgus (range 5 degrees varus to 11 degrees valgus). Flexion range has increased from 95 degrees (range 90–100) to 107.7 degrees (range 85–120) post-operatively. One patient developed progressive genu recurvatum, at 7 years follow-up with range of motion at 25 degrees hyperextension and 110 degrees flexion. He is asymptomatic and tolerated 45 min of walking with brace and reluctant for revision surgery. The remaining patients has satisfactory result. Average pre-operative Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score was 68.5 (range 51−87) improved to 50.7 (range 21–71) at 12 months post-operative and pre-operative Knee score averaged 53.3 (range 51–55) increased to an average of 88.5 (range 82–94). Only Case 3 have bilateral knee revised for aseptic loosening 16 years and 10 years after the index operation for the deformed right side and contralateral left knee respectively. The other cases have no sign of loosening radiologically.
Discussion
There are certain advantages to perform single stage, intra-articular correction of an extra-articular deformity in TKA. It is particularly favourable in elderly patient with low physical demands and limited life expectancy. As described in our series, most of the patient reported satisfactory results. Single stage total knee replacement (TKR) avoids a second stage surgery, shortens the time of recovery and save cost This technique does not require additional incision. Complications of a separate correctional osteotomy including longer operative procedure, more intra-operative blood loss, implant failure, non-union and malunion can be avoided. Early rehabilitation can be expected. Wang et al. 1 has achieved satisfactory short-term clinical outcome adopting the same surgical approach for up 20 degrees extra-articular varus deformity in the femur and up to 30 degrees in the tibia in the coronal plane. Post-operatively, only one patient had deviation of mechanical axis of beyond 2 degrees.
However, it is important to note that not all patients with extra-articular femoral deformity are suitable for single stage intra-articular correction during TKA. Severe femoral valgus deformities that are closer to the knee are more difficult or even impossible to be corrected with an extra-articular osteotomy to restore the mechanical alignment. Wolff et al. 4 suggested if a deformity in the supracondylar area is > 20 degrees, soft tissue balancing will be difficult after joint line resection. In our case number 6, the extensive medial soft tissue release extending to the postero-medial corner may predispose to the recurvatum deformity. (Table 1)
Patient characteristics, operative details and results.
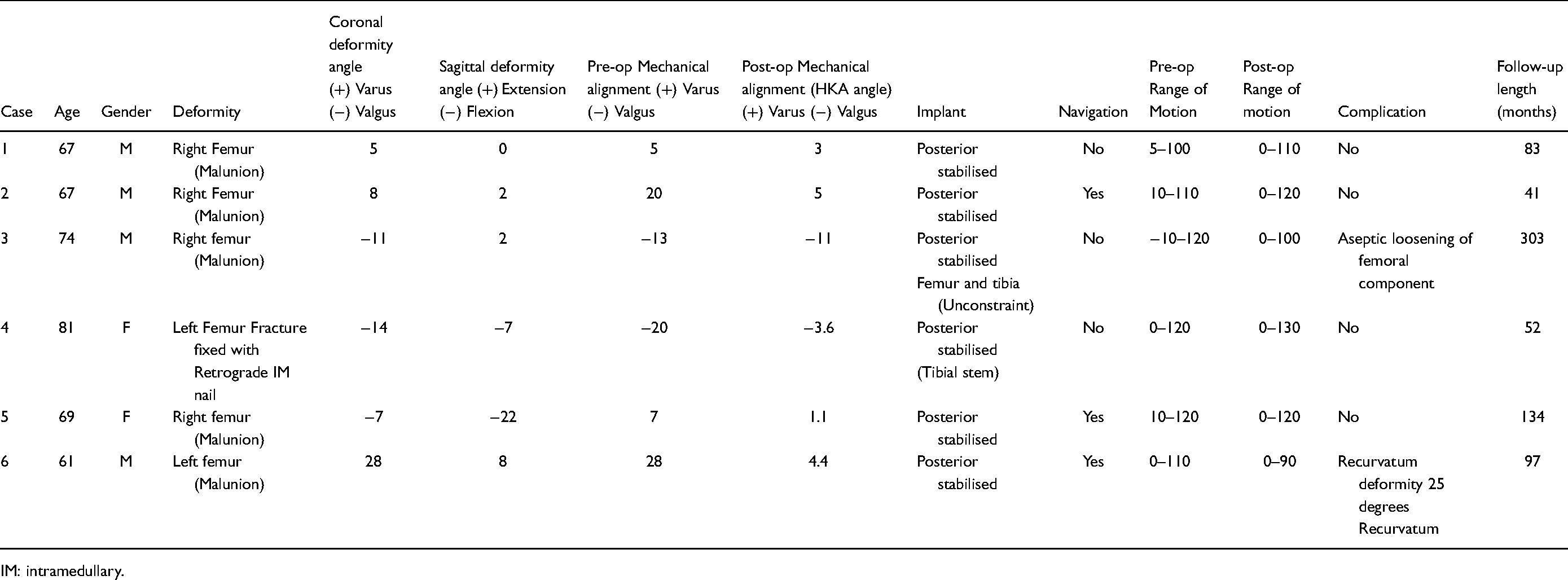
IM: intramedullary.
For younger active patients with severe deformity, it may be desirable to perform a correctional osteotomy and perform balancing of soft tissue close to normal anatomy during TKA via a simultaneous or staged surgery. Lonner et al. 5 reported 11 total knee arthroplasties with significant extra-articular deformity (average of 27 degrees varus) underwent single stage, simultaneous femoral osteotomy and TKA. The complication rate was reported up to 45% including one osteotomy non-union, two post-operative stiffness of knee requiring manipulation under anaesthesia, one implant complication involving internal fixation of osteotomy which required removal of implant and one pulmonary embolism. Despite the high complication rate, they have achieved significant improvement in knee score at an average follow-up of 46 months.
With the development of navigation system, bone cut can be more precise and closer to the planned osteotomy. Another advantage of navigation system is that intramedullary guide is not required, and it may avoid problems with medullary guide insertion in cases with severe deformity or pre-existing hardware like plates, screws and nails which will hinder the intramedullary guides. The latter may necessitate removal which may be impossible without much bone removal. Upon removal, the residual screw holes or osteopenia beneath the plate act as a stress riser and predispose to fracture. Current views would favour avoiding hardware removal as much as possible or partial removal. Cantani 6 reported use of image-free navigation system in a series of 20 patients reporting satisfactory clinical and radiological outcome. With the advent of Robotic arm, more precise ligament balancing may be achieved.
Despite we have obtained pre-operative CT in only one case in this series, we recommend the routine use of pre-operative CT scan and 3-dimensional reconstruction for patient undergoing TKR with extra-articular deformity. Whole length AP and Lateral view of lower limbs may be adequate to assess coronal deformity as described by Wolff. 4 Sagittal deformity is less well-documented in the literature; However, it is understood that recurvatum deformity is better tolerated than procurvatum in femoral deformity due to potential notching during anterior femoral bone cut. There is no absolute cut-off value as the indication for intra-articular correction of procurvatum or recurvatum. Studies has reported successful correction in to up 10 degrees and 15 degrees of procurvatum and recurvatum respectively.7,8 The presence and the degree of rotational deformity is more difficulty to be determined on plain film. Rotational deformity can be evaluated in physical examination where patient may demonstrate asymmetry in tibial tuberosity or foot progression angle between normal and mal-aligned limb during gait examination. Plain film x-ray also provides clues such as subluxation of patella into trochlea groove. Pre-operative CT should include axial cut including the rotation profile of knee, at the level of deformity and anteversion of hip as well as the normal side for comparison. Correction power of rotation deformity in TKA is limited particularly in malunion of femur with excessive internal rotation due to potential notching over anterolateral distal femoral cortex as reported by Wang et al. 1
Conclusion
In summary, intra-articular correction of an extra articular femoral deformity for TKR is an attractive approach in mild to moderate deformity further from the knee joint. This is especially beneficial to elderly patients with low physical demands which saves operative time and prevent complications of an additional osteotomy. We have reported 6 cases and majority of them has enjoyed satisfactory pain relief and function without reoperation at mid-term. With the increasing acceptance of kinematic alignment in recent years, 9 mild deviation from the mechanical axis made surgery easier and does not affect long term result as described in our cases and in literature.7,10,11 Careful patient selection and pre-operative planning is essential to a satisfactory outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.