
Abstract
In the first part of this article, we have discussed the pathogenesis, clinical presentation, diagnosis and classification of infection after fracture osteosynthesis with implants, termed here as osteosynthesis-associated infection (OAI). Prolonged antibiotic treatment is usually necessary. Implant retention and maintenance of fracture stability to allow for fracture healing in spite of infection are allowed for OAI. Depending on the severity of infection, status of fracture healing and host status, the treatment follows five common pathways. These are non-operative treatment, debridement with implant retention, conversion of fixation, implant removal and suppression therapy. The decision-making process leading to each treatment pathway and challenging scenarios is discussed in detail.
Introduction
The term osteosynthesis-associated infection (OAI) is defined as infection occurring after surgical fixation of fractures with internally placed implants. The goal of treatment is to eradicate infection, allow fracture healing, preserve body function and prevent its recurrence. 1 Presentation is heterogeneous and treatment is highly individualized. Because of a lack of properly conducted comparative studies, the current discussion is at best based on larger series by Torbert et al., 2 Berkes et al. 3 and Rightmire et al., 4 a number of smaller case series and heterogeneous studies.
The three most important factors in devising a treatment strategy for OAI are mechanical stability, time interval between fixation and infection and the presence of union. The other guiding factors are implant type, presence of collections, non-viable bone, graft or substitute, soft tissue and bone defect, joint involvement, host status and response to treatment. Patients requiring surgical treatment are best referred to subspecialized centres that are better equipped. 5 Patients should expect prolonged hospital stay, multiple surgeries and prolonged use of intravenous antibiotics. Optimization of the general nutritional status and co-morbid factors including smoking cessation is an important part of general management. 6
Fracture stability and implant retention
Although commonly considered as orthopaedic implant infection, OAI is fundamentally different from prosthetic joint infection (PJI). In PJI, permanent eradication is necessary but difficult because of a large potential joint space and sizable implants. Late haematogenous infection long after surgery is common in PJI while early infection is more common in OAI.
In OAI, implants can be definitively removed after fracture union. The potential dead space is smaller. Involved joints in OAI are lined by vulnerable living cartilage while cartilage preservation is irrelevant for PJI. For late PJI, the success rate of implant retention is as low as 15–54%, 7 while for OAI, when fracture stability is maintained, the rate of successful hardware retention is 56–86%. 3,4
The majority of OAI occurs within 10 weeks from surgery. 2 Even in the presence of infection, fractures can still heal provided that it is vascular and stable. 8 The ability to heal is poor if there is sequestrum, bone defect and implant loosening. Stability is important as movement across the fracture causes soft tissue irritation, damage to revascularization, haematoma and dead space formation. These factors are detrimental to both fracture healing and control of infection. 9
An infected and united fracture is easier managed than an infected and non-united fracture. 10 Even though the eradication of biofilm organisms maybe difficult with the presence of implants, suppression of infection is possible as long as collections, tissue necrosis and dead spaces are minimal. If the hardware can provide much stability to the fracture, it is preferentially retained until fracture union.
Treatment strategy
Acute infection 2 weeks after surgery
Around one-quarter of all OAIs presents within 2 weeks
They are sometimes regarded as ‘superficial infections’ when there is only mild wound edge erythema, superficial discharge and breakdown. Ultrasonography or computed tomography (CT) scans are helpful in detecting deep-seated collections which are often not confirmable clinically. Any deep-seated collections should be drained and sent for microbiological tests. If it is certain that the infection is recent and superficial, empirical intravenous antibiotics for 2 weeks without surgical debridement may suffice. In situations with large deep-seated collections, persistent discharge or breakdown of wound edges, a formal debridement with implant retention is indicated. Preemptive drainage of wound haematomas that are doubtful of being infected is indicated, especially in high-risk regions like the tibia.
Delayed infection before expected fracture union
In delayed OAI occurring from 3 to 10 weeks after osteosynthesis, fracture healing is often incomplete. Biofilm formation and osteomyelitis are moderate. The surgical strategy is similar to the debridement, antibiotics and implant retention protocol in PJI. 11 Routine removal of implants is best avoided as this may result in gross instability and worsening of infection. Smoking, diabetes, medical comorbidities, pseudomonas infection and open fractures are risk factors for failed implant retention. External fixation with implant removal is necessary when the duration of infection is prolonged or when implants are loose. 4
From the two larger retrospective series by Berkes et al. 3 and Rightmire et al., 4 the expected rate of successful hardware retention with debridement and systemic antibiotics is 68–71%. Despite fracture healing being usually successful, around 50% of implants would require eventual removal for unresolved infections. OAIs with intramedullary (IM) nails are thought to be associated with delayed diagnosis and are more difficult to access surgically. Despite this, Chen et al. 12 reported high rates of successful retention of IM nailing in patients with OAI after femur fractures. On the other hand, patients who underwent removal and external fixation experienced a higher incidence of non-union and other complications.
Late infection with non-union
When infection presents at more than 10 weeks after osteosynthesis, it is nearly always well established and deep seated. These are often regarded as infected non-unions. Delayed diagnosis, implant loosening, tissue necrosis, mature biofilm and sequestrum formation are usual. External bracing alone is unstable and non-surgical treatment is likely to fail. Loose implants are no longer functional and therefore must be removed or revised. The sequestrum should be excised. Infection must be controlled before reconstruction of bone defects. There is a low threshold for conversion to external fixation. 12,13 In situations where this is not possible, revision of the internal fixation with stable bridging implants is indicated. In a systematic review of 34 case series, a fracture union rate of 66–100% 14 is generally achievable by single- or two-stage surgery. However, up to 60% of patients may have persistence of infection after fracture union.
Indolent infections must be suspected for all aseptic non-unions, delayed unions and implant loosening. Specimen should be routinely sent for microbiology and histological examination. Around 20% of these cultures specimen may return as ‘surprise’ positives. Still, the chance of successful union is 80% when these situations are adequately managed with antibiotics. 15
Infection after fracture union
Management of infection after fracture union is usually straightforward by debridement and implant removal. In patients with previous OAI, implants should be preemptively removed because infections are likely to recur from biofilms. 3,16 CT scans are useful in clarifying the status of union when radiographs are doubtful. Patients associated with osteomyelitis, septic arthritis or soft tissue defects are managed accordingly following standard principles (Figure 1).

Outline of five different treatment pathways for OAI in different clinical situations. The management pathway should be stepped up upon failure of control from (1) non-operative treatment to (2) implant retention and lastly to (3) conversion of fixation. (4) Implant removal is performed after fracture union and (5) suppression therapy is recommended for poor surgical candidates. OAI: osteosynthesis-associated infection.
General surgical considerations
Surgical debridement
Debridement of necrotic soft tissue, debris, pus and haematoma should proceed aggressively, while skin at the wound margins is sparingly removed. The implant and fracture are assessed for stability. Exchange of implants reduces the biofilm burden and allows for access to locations covered by the plate. Devitalized bone should be removed in severe and persistent infections even when structurally relevant. Wound lavage is performed using a large amount of normal saline. The use of antiseptics and high-flow pulsatile systems 17 is weakly supported by evidence but often performed. Sizable bone voids can be filled with antibiotic-impregnated spacers, and soft tissue defects are controlled by meticulous closure, vacuum assistance or flaps. Primary wound closure is preferred especially when there is exposed bone.
A majority of patients will require more than two or three debridements. 4,16 A second look debridement should be routinely planned and explained to patients before performing the first. When there is doubtful tissue viability and extensive tissue necrosis, re-exploration and debridement should be performed every 2–3 days until a grossly non-infected base with healthy bleeding bone and soft tissue is obtained.
Use of external fixators
Complete implant removal and conversion to external fixator is indicated when there is failure of control after repeated debridement or when there are multiple adverse local and systemic factors. 12 Illizarov-type ring external fixators provide better fixation in cancellous bone. They are particularly useful in the periarticular region where preservation of joint motion is a concern. The success rate of ring external fixation is high. 18 –20 The main drawbacks include bulkiness, patient discomfort and very high rate of pin tract infections. In patients with low systemic risks and favourable soft tissue, conversion back to internal fixation can be considered after the infection is controlled. 21
Local antimicrobial therapy
Local antibiotic therapy is not strongly evidence-based but commonly practiced. 22 Knowledge is borrowed from PJI where local antibiotic concentrations are increased with minimal systemic toxicity. 23 The various options include commercially available antibiotic impregnated polymethyl methacrylate (PMMA) beads, 24,25 antibiotic-loaded PMMA bone cement spacers 26,27 and antibiotic-loaded PMMA-coated IM rods. 28 Even local application of vancomycin to the operative site has appeared to reduce infection in high-risk surgeries. 29
Antibiotic beads are used in contaminated open wounds with smaller sized bone and soft tissue voids. 30 They are commercially prepared and relatively easy to remove. It is indicated when stability of the fracture is maintained and short-term filling is desired.
A two-stage approach with antibiotic-laden spacer and subsequent reconstruction appears to be relatively simple, effective and predictable compared to other elaborate means. 31 Masquelet and Begue 27 described the technique of antibiotic cement spacer-induced membrane and delayed bone grafting. This technique has high success and low complication rates for traumatic and infection-related bone defects. 26,31,32 At debridement, sizable defects are temporarily filled with antibiotic-laden cement which also provides structural support and prevents fibrous ingrowth. Since PMMA curing is exothermic, heat injury and denaturing of impregnated drugs are possible. Heat stable water-soluble drugs such as aminoglycosides, vancomycin and imipenem are preferred. Combining two or more antibiotics in a single spacer is common and shown to be synergistic in vivo. 33 The amount of antibiotics used is typically up to 10% by weight for PJI. For example, 0.5–1 g of gentamicin and 2–4 g of vancomycin is mixed with 40 g of PMMA cement in our usual practice. Higher concentrations of antibiotics may be considered, as structural integrity is less relevant to OAI. The mixing of PMMA is performed without vacuum, so that porosities, irregularities and the surface area for drug release are increased. 34
The rate of antibiotic elusion varies between drugs and geometries of the spacer. 35 It should be noted that a high concentration is released within a very short period hours after implantation, and the local concentration is exponentially reduced within a few days. 36 Since an inhibitory concentration is not reliably maintained after 2 weeks, it is mandatory to supplement local antibiotics with systemic therapy. 37 Retained PMMA spacers can become a nidus for infection and should therefore be routinely removed.
Second-stage cancellous bone grafting is performed after 6–8 weeks. A pseudo-membrane can usually be found enclosing the PMMA spacer. Although the cellular and molecular mechanism behind this induced membrane is still being studied, it is usually vascular and rich in growth factors. 26 Tissue samples are obtained to document clearance of infection, and graft material is placed within this viable clean cavity. 38,39 Placement of bone graft and bone substitutes in the presence of uncontrolled infection is contraindicated (Figures 2 and 3).
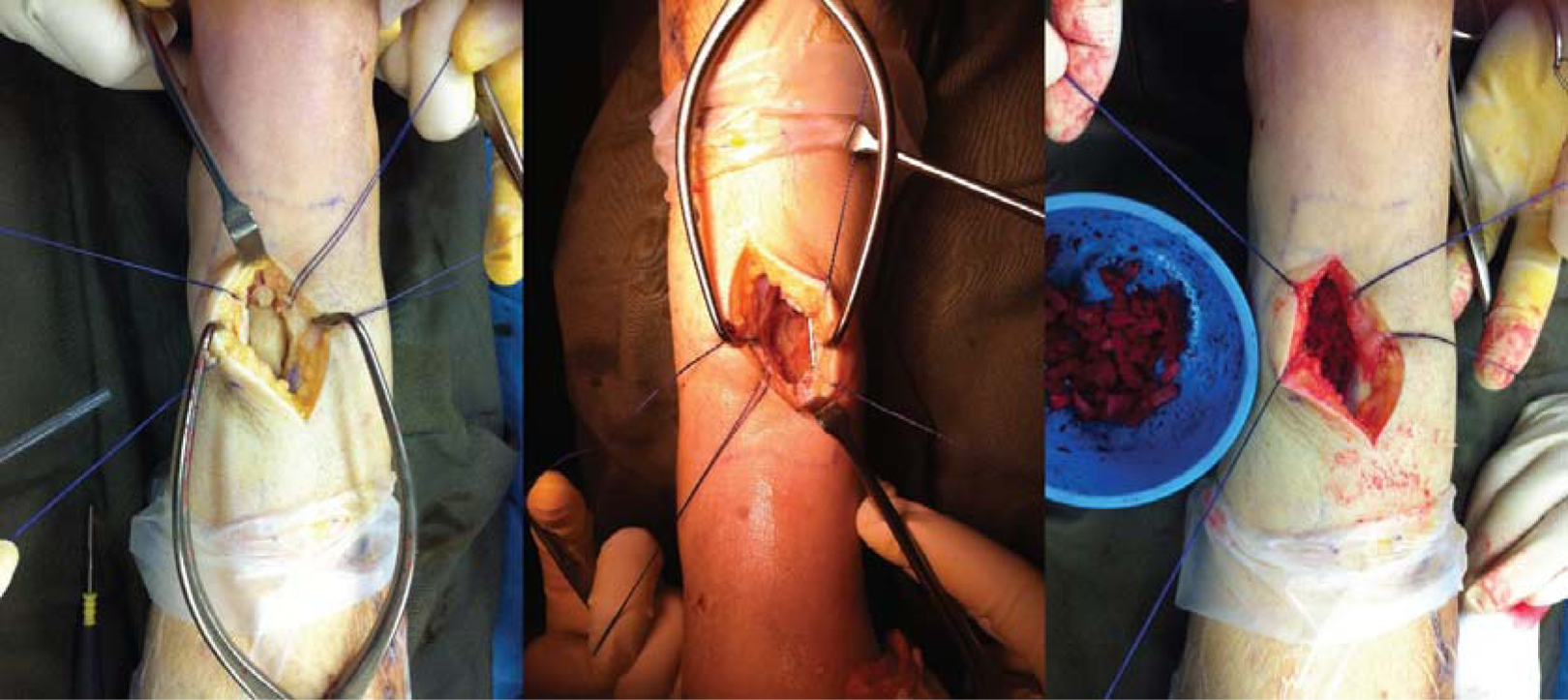
The PMMA-induced spacer technique at the bone grafting stage in a patient with distal tibia bone defect. After control of the infection, the fibrous pseudo-capsule encasing the PMMA spacer is opened and autogenous bone graft is placed within a well-contained cavity. PMMA: polymethyl methacrylate.

Serial radiograph of the same patient from before cement removal and bone grafting (0 m) showing union and remodelling up to 20 months.
Specific challenging scenarios
Massive bone defects
Bone defects are common in OAI, and sometimes a necessary evil resulting from adequate debridement of the sequestrum. When such defects are segmental, fracture healing is compromised. A plethora of techniques exists in the management of bone defects. 40 It is repeatedly mentioned that priority must be given for eradiation of infection before tackling of bone defects. 41 The majority of smaller defects of less than 4 cm is usually handled successfully with the two-stage antibiotic PMMA spacer-induced membrane technique mentioned above. A study reported reduced reinfection rates when bone graft is mixed with local antibiotics. 42
A combination of techniques can be used to archive success in massive defects. 43 Distraction osteogenesis with circular fixators is useful for larger segmental defects especially when realignment of deformities is also desired. 44 The risks are refractures, pin tract infections, soft tissue impingement and neurovascular complications. 45 Internal fixation augmentation after docking shortens the time needed for external fixation without considerable risk of reinfection. 46,47 The Papineau technique employs open cancellous bone grafting for problematic osseous defects with overlying soft tissue defect with high rate of reported success 48 ; however, the need for repetitive dressing is intensive from the nursing perspective and wound healing by secondary intension and relatively slow.
Tibialization of the fibula or graft-induced tibiofibular synostosis is an option for isolated tibial defects with an intact fibula. 49 Free vascularized bone transfers are technically demanding but useful for massive defects at a slight danger of flap loss, stress fractures and the need for extended periods of protection.
Soft tissue defects
Routine wound closure and avoidance of exposed bone and hardware are recommended. Suction drainage should be placed into deep cavities and potential dead spaces to prevent retention of haematoma. Locations with thin soft tissue envelope such as the clavicle, patella and distal tibia are especially difficult, and primary closure can be challenging even when the defect is as small as 2 cm.
Flaps are needed for severe soft tissue defects. Free tissue transfer in young patients has high reported success rate even when implants are transiently exposed. 50 –52 Risk factors for failure of free tissue transfer are tobacco smoking, renal or liver failure, immune deficiency, chronic hypoxia, malignancy, diabetes, old age, steroid use, alcoholism and substance abuse. 53
Acute shortening is relatively easy and safe, 54,55 effectively reliving soft tissue tension and reducing dead space. It is particularly useful when there is combined soft tissue and bone defect, optionally followed by distraction osteogenesis.
Negative pressure wound therapy (NPWT) may be used to assist wound coverage accelerate granulation formation and removal of exudate in OAI. It is a useful bridging therapy while waiting for granulation base to develop for skin grafting or to accelerate healing by secondary intension in smaller defects. Importantly, early closure of open fractures by 5–7 days remains the best way to reduce the risk of nosocomial infection, and prolonged NPWT should not be used as a substitute for early wound closure and flap coverage. 56
Infection after IM nailing
OAIs after IM nailing are uniquely challenging to manage. The IM canal is surgically less accessible, and diagnosis is more likely to be delayed. Treatment is based upon the same principles of stabilization, systemic antibiotics, surgical debridement, soft tissue coverage and staged bone defect management. 57 Makridis et al. 58 devised a surgical management protocol based on three different stages of infection. For early infections, implant retention with or without debridement is sufficient. For delayed infections, debridement, reaming and nail exchange with usual or antibiotic laden implants are suggested. For late infections, debridement, nail exchange or conversion to external fixation is recommended.
Antibiotic cement-coated rods are increasingly being used for IM infections. A number of small series reported success using them as temporary means for fracture stabilization and local bacterial killing, 59 –62 followed by refixation with a new IM nail around 2 months later. A large bore chest tube can be used as an economical mould in which PMMA is injected and cured around a rush pin or an Ender’s nail. 63 When axial and rotational stability is required, PMMA-coated small diameter interlocking nails can be used 63 or antibiotic beads can be placed within slotted nails to attain a similar effect.
Reaming effectively removes infected IM debris and bone. The reamer irrigator aspirator (RIA) is a specialized single use reamer which allows simultaneous irrigation and suction within the IM cavity. A number of small studies 64 –66 have reported a success rate of 96–100% using RIA and antibiotic cement rods to treat IM osteomyelitis. RIA appears safe, although more studies are needed to confirm its theoretical advantages in infection, prevention of fat embolism and prevention of thermal necrosis.
Articular involvement
Synovial joints are poorly perfused inherent dead spaces with vulnerable cartilage. Articular involvement is notoriously difficult to manage in OAI. Involvement of the knee and ankle is associated with high-energy tibial plateau and pilon fractures. Shoulder and elbow OAI may lead to very poor results.
Based on experience, we routinely immobilize infected joints after debridement. This is notably dissimilar to PJIs where cartilage preservation is irrelevant, and mobilization is usually allowed with articulated antibiotic-loaded spacers. With immobilization, stiffness is common but control of infection is usually more predictable. An uncontrolled infection in a synovial joint is worse than a stiff joint with relatively preserved cartilage. After control of the infection, it is possible to regain significant functional ranges by open or arthroscopic releases in the shoulder, elbow and knee.
Arthrodesis is considered when salvage of a destroyed joint is impossible. 67 Prosthetic replacement should be carried out in two stages with antibiotic-impregnated spacers after complete clearance of infection in order to minimize the risk of contamination. 68 Tumour prosthesis replacement of large defects carries around one-quarter risk of reinfection. 69
Amputation is indicated when there are significant systemic adverse factors. Those with considerable soft tissue defects are less suitable for joint prosthesis and more suited for amputation or fusion. 70 In special circumstances, amputations may be performed distal to the infection to reduce mechanical and vascular load. 71
Systemic treatment
Pharmacological treatment of OAI is mandatory. This can be divided into three stages: empirical treatment, specific targeted treatment and occasional need for long-term suppression. In the selection of antibiotics, bacterial susceptibility, bone penetration and side effects should be considered.
Empirical antibiotics
Empirical intravenous antibiotics can successfully treat early and superficial infections that do not have well-established biofilms. Antibiotics do not penetrate into haematoma, seroma, abscess or devitalized bone and necrotic soft tissue. High-dose intravenous administration can best ensure bactericidal concentrations in poorly perfused bone and peri-implant areas.
Staphylococcus aureus, in particular, methicillin-sensitive S. aureus, remains a common cause of OAI in the community; anti-staphylococcal antibiotics such as penicillinase-resistant penicillin (e.g. cloxacillin) or first-generation cephalosporin (e.g. cefazolin) are first-line drugs for empirical coverage. In patients with previous history of methicillin-resistant S. aureus infections, and those with prolonged hospitalization or institutional care, glycopeptide such as vancomycin or teicoplanin should be used for empirical treatment. Third-generation cephalosporin such as cefotaxime or ceftriaxone should be considered for OAI around the perineum, 2 elderlies, diabetics or immunocompromised patients because they are at higher risk of gram-negative infections.
In delayed and late infections occurring more than 3 weeks after osteosynthesis, less virulent organisms such as coagulase negative staphylococci (CNS) or unusual organisms are common. Empirical treatment must not interfere with a rapid microbiological diagnosis. Unless in severe sepsis, empirical therapy is withheld until deep tissue and fluid samples are obtained. It is important to note that 80–90% of CNS are resistant to methicillin. Prolonged treatment with a targeted drug is needed in delayed cases because bone and implant involvement is usually established. Misidentification of delayed or late OAIs and inadequacy in antibiotic treatment commonly leads to persistent bacterial residence and development of resistance.
Targeted antibiotics
Resistant strains can account for more than 50% of S. aureus and 32% of all organisms that cause OAI. 2 Target-specific therapy should begin as soon as culture isolates and antibiotic susceptibility patterns become available. When a specific microorganism is identified, the broad-spectrum empirical drug is changed to a narrow-spectrum target-specific antibiotic to minimize host flora suppression and emergence of resistance. Polymicrobial growth is associated with contaminated open fractures and poor host immunity. A combination of drugs is usually necessary.
For staphylococci infections, combined therapies with rifampicin have shown increased in vitro and in vivo eradication compared to monotherapy with quinolone or β-lactams and superior biofilm penetration. A few prospective studies demonstrated the cure rates of 69–100% using a 6-month rifampicin–quinolone combination regimen, especially in earlier infections. 72,73
Duration of antibiotics
In all situations, we recommend initial high-dose intravenous treatment for 3 weeks. Prolonged therapy is always necessary in delayed or late infections with implants. In patients showing rapid response, this may be changed to oral drugs with high bioavailability in bone. 74 A peripherally inserted central catheter simplifies long-term venous access with minimal risks. It is necessary to regularly monitor inflammatory parameters, local conditions and radiological evidence of fracture healing and implant loosening. Antibiotics are stopped only when there is clinical resolution of infection, normalization of biochemical markers and radiological signs of good fracture stability, no implant loosening and progressive healing. When in doubt, positron emission tomography – computed tomography (PET-CT) scans are useful in monitoring both the status of infection and fracture healing.
The minimal duration of antimicrobial therapy for delayed OAI is 6 weeks with retained implants when patients have optimal response both clinically and biochemically. This is increased to 3 months or more if initial control is not rapid and adverse factors local or systemic are present. The duration can be reduced to 3 weeks if all implants are removed with good local control and fracture healing (Table 1).
Recommended antibiotics (choice of antibiotics should be guided by antibiotic susceptibility testing results)a.
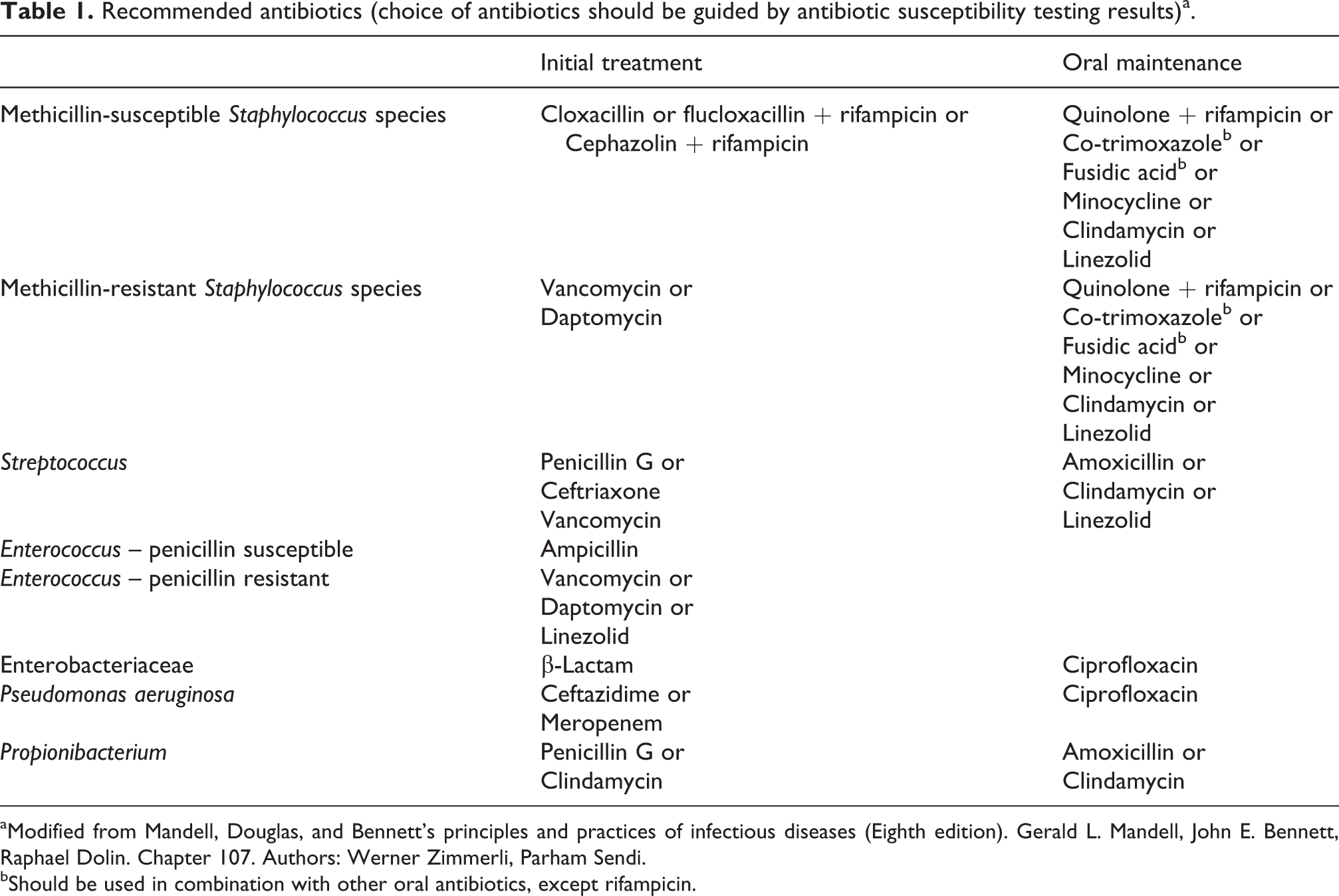
aModified from Mandell, Douglas, and Bennett’s principles and practices of infectious diseases (Eighth edition). Gerald L. Mandell, John E. Bennett, Raphael Dolin. Chapter 107. Authors: Werner Zimmerli, Parham Sendi.
bShould be used in combination with other oral antibiotics, except rifampicin.
Failed eradication and long-term suppression
Failure of control and re-emergence of infection usually happens within 3 months after stopping antibiotics. 75 Long-term suppression therapy is indicated when fracture healing is incomplete or when surgical treatment is impossible. Suppression should not be a routine alternative to surgery because of increased risk of adverse drug reactions and bacterial resistance. Fracture healing can occur during drug suppression, and implant removal is still strongly advised afterwards.
Adverse effects
Adverse drug reactions often occur when antibiotic treatment is prolonged. These include allergy, drug rash, antibiotic-associated colitis, bone marrow suppression, leukopenia, thrombocytopenia and drug fever. Specific side effects for rifampicin include liver impairment and thrombocytopenia. For vancomycin, patients may develop renal impairment. Patients on daptomycin can develop myositis with need to monitor creatine kinase. 76 Monitory measures for side effects are necessary at constant time intervals. Patients suspected to be suffering from adverse reactions should receive advice from infectious disease specialists.
Drug fever presents a specific diagnostic dilemma. Unlike uncontrolled infection, there is improved local symptoms and signs, improving erythrocyte sedimentation rate (ESR), C-Reactive Protein (CRP) and low leukocyte counts. Antibiotics are stopped or switched to a different class and patients are observed closely without additional surgery. Alternatively, if local and systemic features remain doubtful, strong consideration is given to perform additional debridement together with modification of antibiotics.
Ongoing developments
Dipstick leukocyte esterase colorimetric measurement is recently being evaluated as a cost-effective and rapid test using synovial aspirates in PJI with high sensitivity and specificity. 77 The role of this test has not yet been investigated in OAI. Novel molecular markers based on immunoglobulin G (IgG) antibodies are being studied as an alternative technique for pathogen identification. 78 In addition to sonification, electrical stimulation and laser-generated shockwaves may enhance detachment of biofilms organisms from implants for diagnosis. 79,80
Implant designs are being altered for the prevention and control of OAI in a number of ways. 81 Specialized coating materials 82 and drug eluting implants are currently being developed. 83,84 Nanostructured surface finishing 85 and hydrophilic surface materials such as polyethylene oxide, 86 bioactive copper and silver may inhibit bacterial adhesion and biofilm formation. Prophylactic use of antibiotic-coated nails is being investigated for open fractures. 87
A pilot study showed that local application of bismuth thiols may be effective in preventing infections in open fractures. 88 Local antibiotic delivery and dead space control maybe enhanced using specialized water-soluble gels or polymers other than PMMA which are also less exothermic. 89,90 The role of biological agents such as bone morphological proteins that speed up bone healing is being investigated in OAI. 91,92 The cationic steroid antibiotic CSA-90 is a novel drug being investigated for both bone stimulation and bactericidal properties. 93
Summary
Overall, the subject of OAI remains to be challenging and is predominantly an experience-based practice. Once more, we emphasize the importance of maintaining mechanical stability in any treatment strategy. Two-stage use of antibiotic-loaded PMMA spacers appears to result in more predictable success than single-stage strategies. Much knowledge gaps remain to be filled by properly conducted clinical research. Investigations in novel techniques and robust comparative studies are particularly needed. While randomized studies are hard to conduct in this heterogeneous group of patients, establishment of large international multicentre bone infection registries may provide useful insights.
Footnotes
Authors’ contribution
This work has not been published and is not being considered for publication elsewhere. All co-authors have made significant contributions to the work and have read and approved the submission of manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.