
Abstract
Bone and surgical site infections after osteosynthesis are notoriously difficult to manage and pose a tremendous burden in fracture management. In this article, we use the term osteosynthesis-associated infection (OAI) to refer to this clinical entity. While relatively few surgically treated fractures become infected, it is challenging to perform a rapid diagnosis. Optimal management strategies are complex and highly customized to each scenario and take into consideration the status of fracture union, the presence of hardware and the degree of mechanical stability. At present, a high level of relevant evidence is unavailable; most findings presented in the literature are based on laboratory work and non-randomized clinical studies. We present this overview of OAI in two parts: an examination of recent literature concerning OAI pathogenesis, diagnosis and classification and a review of treatment options.
Introduction
The term osteosynthesis-associated infection (OAI) is defined here as the clinical or subclinical infection of a fracture following surgical fixation with an internally placed implant. Prosthetic joint infection (PJI) is another type of orthopaedic implant infection. Patients with either OAI or PJI may present with implant-bound infections, bone and soft tissue defects, sinuses, osteomyelitis, implant loosening and deformities as well as various adverse microbiological and patient characteristics. 1,2 OAI is uniquely challenging, however, due to the presence of trauma, fracture instability, non-union and the need for cartilage preservation. Also, at present, there is a relative lack of consensus among clinicians as to the proper treatment of OAI. PJI has its challenges though effective treatment options are better understood. 3 –5
While OAI is uncommon – the rate of infection after closed fracture, for instance, is only 1–2% 6 – its high complexity of management makes it extremely costly to treat. OAI management frequently involves prolonged hospital stay, rehabilitation, repeated operations and the extensive use of specialized investigation and treatment. 7 –9 As a result, patients with OAI have high morbidity rates and are less likely to return to duty. 10 The increasingly frequent use of internal fixation 11 –13 and the emergence of antibiotic-resistant microorganisms 14 have exacerbated this problem.
Risk factors
Fracture type
Open fractures are most commonly associated with OAI. The risk of secondary infection according to the Gustilo and Anderson grading 15 is 2–4% for grades I and II, and between 4% and 52% for class III fractures, depending on the severity of soft tissue damage. 15 –20 Fractures of the lower limbs, especially near the proximal and distal tibia, 11,17,21 are at the greatest risk. 22 Severe soft tissue involvement, polytrauma, 23 penetrating, blast, combat injuries 10,24 –26 and compartment syndrome are significant risk factors for subsequent infection. 27,28 Irradiation-related fractures, 29 pathological fractures 30 and pelvic fractures requiring arterial embolization 31 are all also at increased risk of OAI. In comparison to acute fractures, fixations of non-unions have double the risk of infection. 17
Patient risk factors
Tobacco smoking, diabetes mellitus, history of stroke, heart failure and multiple previous operations are identified risk factors of OAI. 32 –37 Immunocompromised patients can present atypically 38,39 with slow growing atypical organisms 40 and a combination of less fulminant initial clinical features that lead to a delay in diagnosis but later rapidly deteriorate into life-threatening infections. 41 Elderly patients, 42 –44 intravenous drug users and socially deprived patients are also shown to be at higher risk. 45 In fragility hip fractures, both mortality and disability are increased with OAI. 34,46 HIV-infected patients are at risk of osteoporosis, all types of fractures, 47 –49 infection of non-operated fracture haematoma 50 and OAI. 51
Controllable risk factors
There is robust evidence to show that antibiotic prophylaxis is highly effective in reducing the risk of OAI for both open and closed fractures. 15,17,52 In open fractures, the infection risk is profoundly increased when the administration of prophylactic antibiotics is delayed for more than 6 h. 53
In open fractures, a minor delay in initial surgical debridement of more than 6 h is not associated with significantly increased risk, 54,55 but patients operated on by inexperienced surgeons are at higher risk. 56 Early closure of the primary open wound appears to be beneficial. 57 –59 Prolongation of surgery is associated with infection. 23,27,60 The use of plastic adhesive drapes can reduce bacterial load at the surgical site. 61 Overzealous powered reaming or drilling causes heat necrosis. 62 The risk is increased with multiplicity and size of implants and the presence of bone grafts, allografts or other foreign materials. 63 –67 Prolonged use of surgical drains is thought to increase the risk of OAI, but the issue remains controversial. 43 Indwelling catheters and blood transfusions may carry a small rise in the likelihood of infection. 68 –71 There is weak evidence showing that prolonged use of external fixators for more than 28 days before internal fixation is associated with a higher likelihood of infection. 23,72,73
From a randomized study, smoking cessation effectively halved infection and other complications. 74 Routine auditing of infection rates and clinical practice is effective in minimizing OAI at the hospital management level. 75
Pathogenesis
Microbiology
Staphylococcus aureus causes the majority of OAI cases. Methicillin-resistant S. aureus is now more frequent than methicillin-susceptible S. aureus in some areas and not limited to institutionalized patients. 7,34,36,76 –80 OAI caused by less virulent skin organisms, such as coagulase-negative staphylococci (CNS), can be as frequent as S. aureus 6,46 and 80–90% of CNS cases are methicillin resistant. 81 Lower virulence skin flora, such as Corynebacterium 82,83 and Propionibacterium, 84 –86 are increasingly identified as diagnostic techniques are improved and should not be regarded as contaminants.
Gastrointestinal tract organisms, including Escherichia coli, Enterobacter, Enterococci, Klebsiella and Proteus, are important causes of OAI in sites near the perineum. 28 Gram-negative glucose non-fermenters, such as Pseudomonas aeruginosa and Acinetobacter baumannii, are frequently found both inside and outside the hospital. They have a minimal nutritional requirement, tolerance to relatively high temperature and resistant to many antibiotics. There is an increasing frequency of infections caused by multidrug-resistant P. aeruginosa and A. baumannii. 87,88 P. aeruginosa is associated with significantly higher recurrence rates and failure of control as compared with Staphylococcus. 89,90
Polymicrobial infection is linked to open fractures 78,79 and poor outcome. 91 Clostridium species, which is found in the soil, and Aeromonas species, which resides in brackish water, are highly virulent organisms associated with life-threatening necrotizing infections, which require urgent surgical intervention. 92 –97 Nontuberculous mycobacterium and fungi are environmental organisms resistant to conventional antibiotics and disinfectants and occasionally introduced via open wounds. 98 –100 Mycobacterium tuberculosis 101,102 is rare even in endemic countries. 103 When atypical slow-growing pathogens are identified, a pre-existing bone infection, pathological fracture and an immunocompromised state must be suspected. 104 –107
Biofilm formation and development of drug resistance
At inoculation, bacteria are in planktonic form and susceptible to host defence and antibiotics. Successful bacteria initiate infection in the soft tissue and replicate rapidly. Bone and implant involvement increase over the following 1–2 weeks characterized by osteitis, bone necrosis, reduced the new bone formation and implant loosening. Organisms became chronically entrenched within implant surface biofilm and emptied Haversian canals, becoming increasingly difficult to eradicate. 108
Biofilm production 109 is critical to bacterial survival in the environment, because planktonic organisms are highly susceptible to adverse external factors. The biofilm is a colony-like aggregation of cells embedded in an exopolysaccharide matrix mixed with extracellular products, firmly attached to the surface of implants. 110,111 There are five stages in its development and maturation. 112 Free-floating planktonic microbes first adhere to metal surfaces (stage I). In stage II, they multiply and start to produce exopolysaccharide matrix, which retains nutrients and more planktonic organisms. In stage III, the early biofilm architecture develops (colonization) and then matures (stage IV), wherein microorganisms in the deeper layers become increasingly dormant and isolated from the external environment. At the final stage (stage V), microbes are dispersed back into the environment to colonize other new substrates.
Biofilm-bound organisms are resistant to phagocytosis. Macrophages that attempt to attack the biofilm may cause more damage to the surrounding tissues. The exopolysaccharide matrix hinders the penetration of antibiotics and antibodies both physically and by electrostatic binding. Physiological dormancy of bacterial cells makes them refractory to antibiotics that target their metabolic and replication pathways. 113,114 For instance, the minimal inhibitory concentration for biofilm bounded pseudomonas can increase 1000-fold when compared to planktonic forms. 111
Organisms within the biofilm can cross-communicate and adapt. This is referred to as the quorum-sensing system. 115,116 Various virulence factors are regulated and released to protect the biofilm from elimination. In chronic infections, there is increased mutation and increased genetic resistance to antibiotics and host defence. 114 Small-colony variants (SCVs) are slow-growing variants of the offending organism which tend to reside in the biofilm and develop resistance and play a major role in persistent or recurrent infections. 117 Because SCVs are overwhelmed in acute infections, they are not easily detected using routine methods.
Implant material and design
The presence of foreign bodies impairs the host defences. 118 Macrophages accumulated around implants are functionally defective as they become exhausted when unable to engulf targets of excessive physical size. 119 Similarly, granulocytes become activated because of foreign materials, but bacteria-targeted degranulation, ingestion and superoxide production are all impaired. 120 Materials that are less biocompatible triggers off a more intense cytokine cascade, together with adjacent tissue damage and formation of an immune-impaired reactive capsule and a potential space in between. 121,122
Microorganism and biofilm adhesion is affected by bacterial, environmental and surface characteristics. 123 Microrough surfaces at bacterial length scales are prone because of increased surface area and greater resistance to shear forces. 124 Different microorganisms have different affinity for surfaces depending on factors, such as surface topology, chemical composition, charge, hydrophobicity and physical configuration, as well as environmental factors, such as temperature, pH, electrolyte concentration, flow and the presence of serum proteins and antibiotics.
The most commonly used materials are stainless steel and titanium alloy. While stainless steel is less biocompatible and more susceptible to staphylococcal infection in animal models, 121,125,126 they are typically manufactured with a polished surface finish. Conversely, the finishing of titanium alloy is usually anodized, and its microrough surface favours biofilm development. In all, there is no definite in vivo evidence to support the superiority of either material. 127
Implants with internal dead spaces, such as cannulated open section nails, are more prone to OAI. 128 Minimally invasive plating alone does not appear to reduce infection when compared to open surgery. 129 Rather, infection is lowered with low contact plating, because periosteal stripping and disturbance to blood supply are minimized. 130,131 In limited studies, absorbable polymer implants had similar infection risk compared with metallic implants. 132 There is, however, a general concern for associated infection related to their biocompatibility, associated tissue reaction, osteolysis and retained debris. 133
Infection and fracture stability
An unstable infected fracture is more problematic than a stably infected fracture. 134 Although infection is more likely to occur in conjunction with the presence of a foreign body, stable internal fixation of fractures appears to reduce the likelihood of infection. In a rabbit model, osteotomies inoculated with S. aureus were less likely to get infected after stable internal fixation compared to unstable internal fixation. 135 Although the mechanism is still unknown, it is believed that increased soft tissue irritation, difficulty in revascularization, 136 haematoma and evolving dead space resulting from excess motion are all unfavorable factors of infection.
Stability is compromised when there is the persistence of infection for more than 2 weeks. 137 Natural bone turnover is affected by the homeostatic balance between osteoblast and osteoclast activities is disrupted. Surface-associated material from staphylococci induces leukocytes production of tumour necrosis factor alpha (TNF-α, IL-I and IL-6 and upregulation of receptor activator of the nuclear factor-κB (RANK) in pre-osteoclasts. Osteoclasts are hyperactivated, and the balance is tipped against bone-forming osteoblasts. Excessive bone is resorbed from infected areas adjacent to the implant and the fracture, leading to mechanical failure, instability, non-union and persistence of infection 138 (Figure 1).
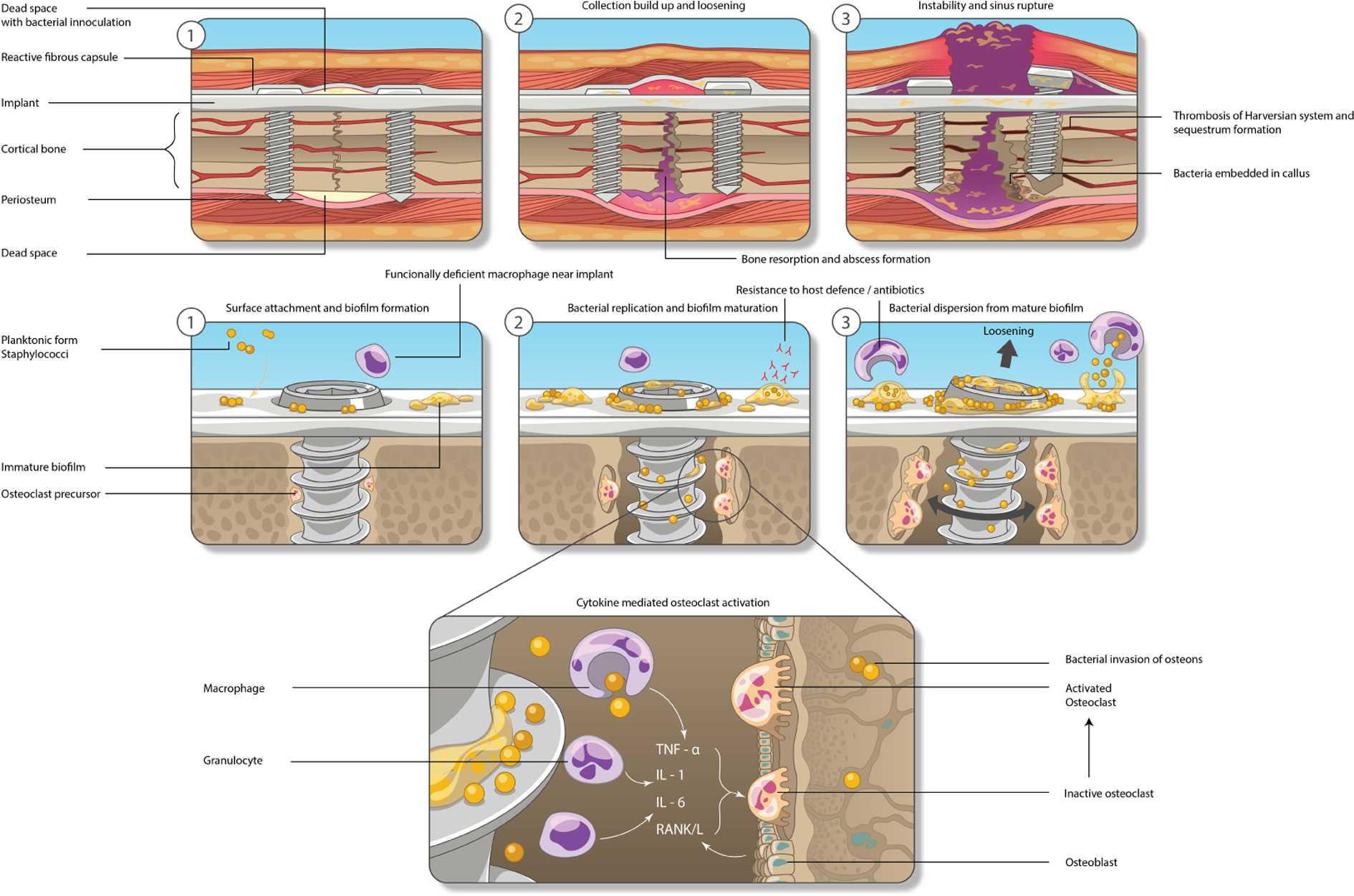
The sequence of events occurring in OAI from inoculation to establishment of infection, implant loosening and abscess rupture at different magnifications (refer to pathogenesis). The illustration is not drawn to scale. OAI: osteosynthesis-associated infection.
Diagnosis
Clinical
The diagnosis of OAI is usually clinical. The presentation varies depending on the virulence of the organism, mode of infection, condition of fracture healing and depth. The typical features are increasing local pain, erythema, swelling, wound breakdown, purulent discharge, sinus formation and systemic symptoms, such as fever. For acute OAI, patients most commonly present in the first month after fracture fixation. 139 Cast treatment can obscure local features and delay the diagnosis. 97 Delayed infections often have less severe features as they are often caused by low virulent microorganisms such as CNS. Moreover, OAI manifestations may be masked because of liberal usage of empirical antibiotic treatment. 140
Imaging studies
Changes in plain radiographs usually occur late and are therefore not useful in detecting acute infections. Patients with delayed infections may have extensive periosteal reactions, implant loosening and non-union on radiographs. 139 Gas indicates severe infections or the presence of a sinus tract if not due to recent surgery. Despite a lack of sensitivity and specificity, 141 routine serial radiographic evaluations serve to provide crucial information on fracture healing and implant stability.
Computed tomography (CT) is useful in confirming the status of fracture healing, the presence of sequestra and infection. Intravenous contrast enhances the visualization of inflamed soft tissue and the rims around abscess. Soft tissue signal findings are 100% sensitive and 87% specific for orthopaedic implant-related infection. 142 Titanium implants are less susceptible artefacts than stainless steel. The implant should be aligned along the axis of the gantry, so that beam traversal is minimized. Other artefact reduction techniques include using high energy settings, narrow collimation, thin sections and extended dynamic ranges. 143 CT scans contrast sonograms are useful in evaluating deep originating sinuses. 144 Gadolinium-contrast magnetic resonance imaging (MRI) scans are very prone to metallic artefacts but helpful in mapping out infected soft tissue and sequestrum after implant removal.
Ultrasonography is useful for detecting collections. 141 Implant and bone surfaces are highly echogenic, fluid signals are well defined and metallic artefacts are minimal compared to CT or MRI scans. Ultrasound-guided aspiration is appropriate when small collections are deeply situated. The limited acoustic window may fail to penetrate very deep locations at the hip and pelvis in obese patients.
Radionuclide scans are useful in confirming occult implant related infections or anatomical localization of unrecognized focus. The indium-111-labelled leukocyte scan has a superior accuracy of 90% 145 compared to bone-gallium 67 or technetium-99m scintigraphy, because they are prone to false positives from the effects of bone healing, trauma, degeneration and surgery. Unfortunately, there are some major drawbacks of leukocyte scanning. The method is time-consuming, technically complex and relatively expensive, typically requiring at least 2 days for leukocyte labelling and scanning. Routine use of leukocyte scanning to exclude infections in non-unions appears to be less accurate and not cost-effective compared to routine blood tests alone. 146
Positron emission tomography
Until recently, 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) was primarily used for detecting hypermetabolic malignancies. However, PET is discovered to be increasingly useful in infections where glucose metabolism is also increased. The test has a sensitivity of nearly 100% and specificity of above 90% in occult and early musculoskeletal infections, including OAI. Since 2010, the European Medicines Agency (EMEA) considered PET scans to be indicated for the diagnosis of chronic bone and joint and adjacent infection including osteomyelitis, spondylosis, discitis or osteitis including presence of metallic implants. 147
When compared to leukocyte scans, PET is considerably quicker, typically requiring only 2–3 h. There is lower radiation exposure and reduced costs. 148,149 Most importantly, information gathered from PET/CT scans is three-dimensional. The anatomical location of infection is accurately defined. FDG uptake showing moderately raised maximum standardized uptake value circumscribing metallic implants is usually diagnostic of OAI. The images are minimally distorted by metal artefacts. Furthermore, spatial resolution is superior to both leukocyte scans and single photon emission CT. Serial FDG-PET is demonstrated to be useful in monitoring progress. 150,151 With appropriate use of PET scans, infections can be accurately detected where timely surgical treatment can be more appropriately initiated. 152 In very early stages of infection, surgical debridement may be totally avoided by early initiation of antibiotics. 149 Currently, the optimal diagnostic criteria of OAI in PET remain to be studied and accurately defined. False positive exams can rarely occur from acute fracture healing and early post-operative inflammation especially within the first 6 weeks after osteosynthesis.
Blood tests
There is robust data to support routine checking of leukocyte count, erythrocyte sedimentation rate (ESR) and C-reactive protein level (CRP) in OAI cases. In non-unions with suspected infection, the positive predictive value is 100, 56 and 18%, respectively, when three, two and one of the tests are abnormally elevated. In excluding infection, the negative predictive value is 81.6% when all four results are normal. 146
The CRP usually peaks on the second post-operative day and normalizes after 2–3 weeks. 153 A persistently raised CRP beyond 4 to 7 days after surgery raises the suspicion of infection. 154 ESR has high sensitivity but suffers from a long half-life of around 6 weeks and is, therefore, less specific. Serial ESR and CRP levels are very useful in monitoring treatment progress in patients with established OAI. Serum IL-6 levels have a short half-life and have been studied as a possible sensitive and specific alternative to CRP. 155,156 Unfortunately, IL-6 levels are more prone to an elevation in response to major trauma or surgery and still less specific than CRP. 157
Blood cultures should be routinely obtained before surgical treatment. Patients with clinical sepsis have higher yields than those without. False positives due to contamination may be minimized by obtaining two sets of blood culture from two different sites at separate time intervals. Immunocompromised patients with bacteraemia should be suspected to have distant seeding at multiple sites especially when there are multiple implants.
Local samples
Superficial swabs are less sensitive than bone, tissue or fluid specimens and should be interpreted together with clinical features. 158 Superficial swabs are neither sensitive nor specific in chronic wounds and sinus tracts, because contamination and colonization are usual. 159
Aspiration of peri-implant collection for culture and susceptibility testing is relatively simple. Before surgical intervention, the procedure is performed using aseptic technique under clinical or image guidance. Unless in clinical sepsis, antibiotics should be withheld for 2 weeks before specimen collection.
Exploration and debridement can establish the diagnosis when the local and systemic clinical features, laboratory findings and radiological pictures are inconclusive. A comprehensive set of specimens, including peri-implant soft tissues, callus and bone, should collect routinely at surgery. 160 Necrotic and infected materials typically provide higher yields. Sequestrum may harbour slow-growing organisms. Fluids such as joint fluid, pus, infected haematoma or sanguineous collections can be injected into blood culture bottles to improve the recovery of slow-growing microbes. A larger volume of specimen increases the yield.
Histological examination is complimentary to microbiological tests, because infection presents with specific patterns of inflammatory response, leukocyte migration, abscess and tissue necrosis. Atypical low-grade pathogens such as fungus or mycobacterium are sometimes only identifiable through histology. 161 Antibiotic susceptibility tests are routine. Clinicians should liaise with the microbiology laboratory for testing of additional antibiotics if necessary. 162
Culture-negative infections
There are several reasons for negative culture results in patients with suspected OAI, the most common of which is the prior use of antimicrobials. Other common factors include insufficient microbiological testing, inadequate quantity of specimens, failure to obtain the representative samples and use of non-routine or unfamiliar testing protocols. Negative cultures may also result from infections by fastidious organisms or organisms that cannot be cultured. Finally, the clinical situation may not be an infection, but rather an allergic implant material reaction or other scenarios clinically indistinguishable from infection. 163
Mechanical scraping of implants is ineffective in dislodging microorganisms. 164,165 Fluid bath sonification of retrieved implants has a sensitivity of 90.4% in OAI 166 and an 18–30% increase in pickup rate compared to conventional cultures in implant infections. 162,166 –168 The sonification equipment uses low-frequency ultrasound to detach biofilm-bound organisms by the formation of transient microscopic bubbles on the implant surface. The process is performed in lactated Ringer’s solution. Vortex mixing, centrifugation 169 and inoculation of the sonicated fluid in blood culture bottles 170 appear to further improve the diagnostic yield.
While laboratory bacterial culture remains standard, molecular diagnosis by polymerase chain reaction (PCR) of specific genes can identify suspected organisms in 9–85% of culture negative orthopaedic implant infections. 171 –176 The broad range PCR can detect a broad variety of organisms with known sequences of the 16s-rRNA gene. A positive test would have a concordance rate of around 90% with positive laboratory cultures. Sensitivity may be further improved by using sonicate fluid 171 and additionally performing pathogen-specific PCR against common pathogens such as S. aureus. 176 In PCR, slower growing organisms such as Propionibacterium acnes are increasingly identified. 174 The sensitivity of the test varied widely between studies but is thought to dependent on the number of pre-determined organisms in the genome database and secondly following strict handling procedures. PCR has a number of limitations, including proneness to contamination, high equipment costs, lack of quantitative assessments, lack of information on antibiotic susceptibility and difficulty in picking up polymicrobial infections. For best cost-effectiveness, PCR test should be reserved for culture negative cases only.
Classification
OAI may be classified according to the route of infection, the onset of symptoms after implantation, fracture stability, union status, location, the extent of infection and host status. 177 Romanò 178 proposed a seven-item classification, which simultaneously considered clinical presentation, aetiology, anatomical location, host-type, microorganism, bone defect and soft tissue defect. So far, the system has not been widely adopted and yet no other classification system appeared sufficiently precise and comprehensive.
According to time after surgery
Chronological classification of OAI is preferred, because it gives guidance on the treatment strategy. 20 Early or acute infections (within ≤2 weeks after implantation) are most common and associated with virulent organisms, such S. aureus, aerobic gram-negative bacilli or Streptococcus pyogenes. 80 Fortunately, organisms at an early stage are susceptible to antibiotics and associated with less biofilm and sequestrum formation.
Delayed infections (3–10 weeks after implantation) are associated with moderate or less virulent skin flora such S. aureus or CNS. Late infections (>10 weeks after implantation) are commonly associated with delayed diagnosis. Typical organisms are S. Aureus, S. epidermidis and Pseudomonas aeruginosa. 80,179 Delayed and late infections are harder to eradicate due to the presence of biofilm, sequestrum and microbial resistance. Reactivation due to the continuous bacterial residence after successful treatment is common. 90,180 Management is complicated when there are implant loosening and incomplete union. This will be discussed in the second part of this article (Figure 2).

A 76-year-old lady suffering from CNS infection of the proximal humerus 6 weeks from fixation. Infection was controlled with debridement, implant removal, suture stabilization of the tuberosities, immobilization and 4 weeks of antibiotics. Despite healing, the glenohumeral joint was destroyed with only 90° of shoulder elevation. The presentation of this patient can be classified as a delayed infection. CNS: coagulase-negative staphylococci. Note: the extensive periosteal reaction and failure of fixation.
According to route of infection
The route of infection can be exogenous, contiguous or haematogenous. 6,181 Direct exogenous inoculation is most common and is associated with adverse wound factors. Contiguous spread of an adjacent local infection, such as cellulitis or a nearby septic joint and haematogenous seeding from distant sites, is relatively less often compared to PJI. 182,183 It is important to note whether the patient has other foci of infection especially for immunocompromised hosts and those with prosthetic devices. 184
According to fracture healing
The concern for fracture healing is unique in OAI. Romanò 178 proposed a three-category classification based on stability and callus formation. In type I infections, there is stable osteosynthesis and progressive callus formation. Cases may be treated non-operatively with antibiotics and allowing time until union. In type II infections, there is stable osteosynthesis but scarce or absent callus progression. Stability must be maintained, and hardware can be retained. Infection is controlled surgically and with drugs. Bone healing is accelerated through physical stimulation and biological factors. In type III infections, osteosynthesis is unstable, hardware revision or external fixation is required in addition to above.
According to clinical severity
Many studies classify infections as superficial or deep. Superficial infections are usually early infections, only affecting the overlying soft tissue without collection and osteomyelitis. The definition is controversial, because superficial surgical wounds are nearly always connected to the deep unless the fascial barrier in between is water tight. The so-called milder form of ‘superficial infection’ is less common than deep infection according to a prospective multicenter study of hip fractures. 76 Superficial infections are clinically indistinguishable from deep one in locations with thin soft tissue envelope such as near the ankle. 185 Some classifications considered the presence of an active sinus 186 and size of bone defects 187,188 to grade clinical severity and guide management.
According to host type
Host immunity and physiological status are an important factor in surgical decision-making. The systems proposed by Cierny 189 and McPherson 190 classify hosts into types A, B and C. Type A hosts have no significant local adverse factors or medical comorbidities and healthy immune response, metabolism and vascularity of the infected area. Type B hosts have one or two significant local or systemic adverse factors, and Type C hosts either have three or more adverse factors or are medically too unwell to undergo surgery. Type C patients are most immunocompromised and unlikely to benefit from multiple stages of surgery, so either drug suppression therapy or amputation is considered. The downgrading of hosts to a more favourable status is possible by control of systemic and local adverse factors (Table 1).
Systemic and local factors that affect local immunity, metabolism and vascularity in the host physiological classification system adopted from Cierny et al. 189

Summary
We have discussed the risk factors, pathogenesis, diagnostic and classification considerations of OAI above. Stability of the fracture appears to be highly relevant. Despite some adverse effects of implants, their maintenance may be beneficial, because stability imparts better overall control of infection. The absence of a rapid, simple and reliable protocol for diagnosis and the lack of consensus in classification is where further research is needed. Understanding the fundamentals above is essential in formulating preventive and treatment tactics. The management of OAI will be discussed in the second part of this article.
Footnotes
Authors’ contribution
This work has not been published and is not being considered for publication elsewhere. All co-authors have made significant contributions to the work and have read and approved the submission of manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.