
Abstract
Background:
Although internal fixation is the definitive treatment in unstable pelvic fractures with disruption of the anterior arch and a vertical fracture of the sacrum (AO type C1.3), there have been no agreement of the best technique of internal fixation yet. We aimed to derive comparable objective data on stiffness and load to failure in this type of fracture fixations.
Methods:
Synbone was modified into AO type C1.3 fracture model, while treatments were divided into six internal fixation treatment groups using tension band plate (TBP), symphysis pubis plate (SP) with iliosacral screw at S1 and S2 (IS S1-S2), pubic screw (PS) with iliosacral TBP, PS and IS S1-S2, SP and IS S1-S3, PS and S1-S3 and finally PS and IS S1-S3. Sensor was applied to detect the shifting and rotation of fracture fragments. Mechanical strength test conducted with the application of axial force on the sacrum vertebra (S1).
Results:
The highest translational stiffness was observed in the group IS S1-S3 + PS (830.36 N/mm, p = 0.031) and there was no difference on the rigidity of the rotation between the groups posterior fixation using IS S1-S2 and IS S1-S3 (p = 0.51). Meanwhile the highest load to failure was found in group IS S1-S3 + PS (1522.20 N). PS provided advantages compared to the use of plate.
Conclusions:
Group of PS and S1-S3 IS is the configuration of internal fixation with best translational and rotational stiffness and the largest load to failure compared to other techniques in AO type C1.3 fracture.
Keywords
Introduction
Internal fixation of unstable pelvic fractures with disruption of the anterior arch and a vertical fracture of the sacrum is currently the choice for definitive management. However, there has been no consensus on which internal fixation techniques best in this pelvic fracture AO type C1.3. Several studies stated the best type of fixation in the case of vertical instability is the use of iliosacral screws (IS) on S1 and S2. 1,2 However, most of the researches using IS S1-S2 and pubic screw (PS) reported failures. 3 A three-dimensional movement should be carried out in the assessment of a bony pelvic fracture. Until now there have been no test that compares biomechanics especially S1-S3 configuration on an unstable pelvic fractures with anterior arch injuries and posterior arch injuries with vertical fracture of the sacrum. 4 –7
By performing biomechanical test on the unstable pelvic fracture AO type C1-3, we aim to obtain comparable objective data on stiffness and load to failure towards axial force resistance in the Synbone® (Synbone, AG) model. The study is also expected to act as the basic consideration in internal fixation selection for unstable pelvic fractures with vertical fracture of the sacrum.
Material and methods
This is a true experimental study using artificial model of pelvic bone (Synbone) modified into vertical fracture of the sacrum model and superior and inferior ipsilateral fracture of pubic rami.
The model was divided into six treatment groups so that the estimated sample size is five samples for each treatment as calculated using the Federer formula: (n – 1) (t – 1) > 15. The mechanical strength study was conducted at the Laboratory Engineering, Faculty of Engineering and Aerospace, Institute of Technology Bandung (FTMD-ITB), Bandung. Disruption of the anterior arch (pubic ramus) 30 mm lateral to the pubic tubercle with the direction perpendicular to the horizontal plane and complete disruption of unilateral posterior arch with vertical fracture of the sacrum 5 mm lateral to the foramen were conducted before biomechanical testing performed on the pelvic models that are included in the treatment group (Figure 1).

Pelvic fracture C1.3 on synthetic bone Synbone model demonstrating vertical fracture of sacrum lateral to foramen and complete superior and inferior pubic rami fracture; (a) View anterior; (b) View superior.
The following implants were used on this study: Reconstruction plate Synthes: 3.5 mm 12 holes, 142 mm in length. Reconstruction plate Synthes: 3.5 mm four holes, 56 mm in length. Cortical screw Synthes: 3.5 mm, 20–28 mm in length. Cannulated screw 7.3 mm Synthes: full threaded, 110 mm in length for S1, 105 mm in length for S2 and 100 mm in length for S3. Cannulated screw 7.3 mm Synthes: partial threaded, 100 mm in length for pubic rami.
Internal fixation was performed on each treatment group. The first group was treated with one symphysis pubis plate (SP) and posterior iliosacral tension band plate (TBP). The second group was treated with one SP and two IS at S1 and S2 (IS S1-S2). The third group was treated with PS and posterior iliosacral TBP. The fourth group was treated with PS and two IS at S1 and S2 (IS S1-S2). The fifth group was treated with one SP and two IS on S1 and S3 (IS S1-S3). The sixth group was treated with PS and two IS on S1 and S3 (IS S1-S3).
Sensor was installed on five holders (strain gauge circuit TML® [Tokyo Sokki Kenkyujo Co., Ltd.]) connected with data acquisition to detect the shifting of fracture fragments at pubic ramus and posterior (sacrum) pelvic cavity and to detect rotation on mediolateral and craniocaudal axis at a predetermined pivot point: Anteroposterior translation sensor: 10 mm medial from the outer edge of the sacrum and 25 mm from the edge of the posterior sacral. Mediolateral translation sensor: 15 mm caudal from the SI joint, 5 mm medial from the outer edge of the sacrum, and 5 mm from the medial edge of the ilium. Craniocaudal translational sensor: 35 mm caudal from the SI joint and 40 mm caudal from the SI joint. Translational sensor of pubic ramus fragment: each within 3 mm of the fracture line. Rotational sensor on mediolateral axis: anteroposterior translation with sensors on the sacrum and a sensor on the 5 mm lateral from the sacroiliac joint with lumbosacral pivot point. Sensor rotation about the axis craniocaudal: mediolateral translation with mediolateral translation sensor and a sensor 5 mm lateral to the anterior side of the sacroiliac joint with lumbosacral pivot point.
Sensor was installed on the fixated bone and the pelvic models were taken to the engineering laboratory FTMD-ITB, Bandung. Mechanical strength tests were done using material strength tester. Double leg stance was used as the pelvic bone holder model, 6,8 using Austin Moore prosthesis implants measuring 40 with buffer on the posterior side for bone stability during pressure application (Figure 2). The position of the bones at the field test is symphysis pubis and anterior superior iliac spine is on one field frontal. 9,10

Compression test model during axial load test. Double leg stance was used as the pelvic bone holder model, using Austin Moore prosthesis implants measuring 40 with buffer on the posterior side for bone stability during pressure application.
Mechanical strength test conducted on a test group with pelvic models provides the axial force on the plates of sacrum vertebra (S1); this mechanical strength test using a compression test Tensilon® RTF AMD-1310 made in Japan and recorded on a recorder LabView® Signal Express 2011 made in Japan which is connected with strain gauges TML through a set of data acquisition that is capable of detecting translational until 0:01 mm. The axial force with the loading speed of 10 mm/min was given in the test group started with 25 N preload force that aims to make the test sample stable. The load is continued until a translation of ≥2 mm or ≥2° rotation on one of the five point measurements or macroscopic damage was observed to the bones.
Results
Translational and rotational stiffness against axial force
Translational and rotational stiffness and fixation configuration were defined as the slope of the resultant curve of load–displacement vector for three translational points and two rotational points (Figure 3). In the translational and rotational stiffness, analysis of variance test was performed and found significant differences between the average value of translational and rotational stiffness between each treatment (p < 0.05). Further test with Bonferroni post hoc between each treatment group showed a difference in translational and rotational stiffness between each treatment group.
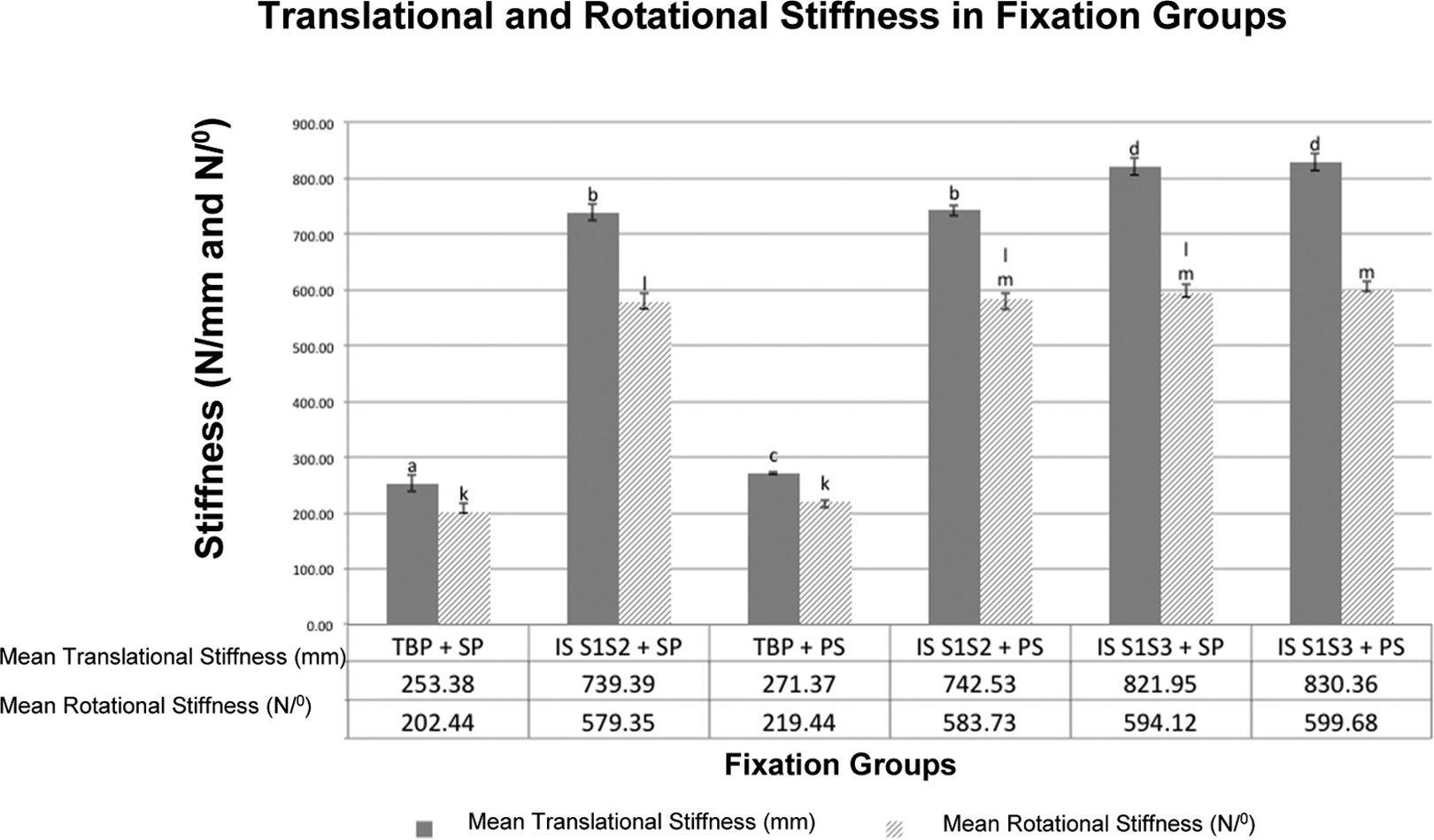
Graph of rotational and translational stiffness means for each treatment group. Notation letter (translation: a, b, c and rotation: k, l, m) is not the same as the above chart, graph between the same colour indicates a significant difference (p < 0.05) whereas the same letter indicates no significant difference. It appears that the highest translational stiffness in the group S1-S3 IS + PS (830.36 N/mm) and the rigidity of the rotation, there is no difference between the groups posterior fixation using IS S1-S2 and IS S1-S3. PS: pubic screw.
Mechanical strength towards load to failure
Mechanical strength of each treatment group was assessed using the parameter of load to failure (Figure 4). ANOVA test results found significant difference on the mean of translational stiffness and rotational stiffness between each treatment group (p < 0.05). Further test with Bonferroni post hoc between each treatment showed differences between the mean load to failure among each treatment group (Table 1).

Graph of mean of load to failure for each treatment group. Notation letters (a, b, c, d) that are not the same as the above graph indicate a significant difference (p < 0.05) whereas the same letter indicates no significant difference. The highest load to failure was found in group IS S1-S3 + PS (1522.20 N). PS: pubic screw.
Load to failure and the failure direction on several fixation groups.
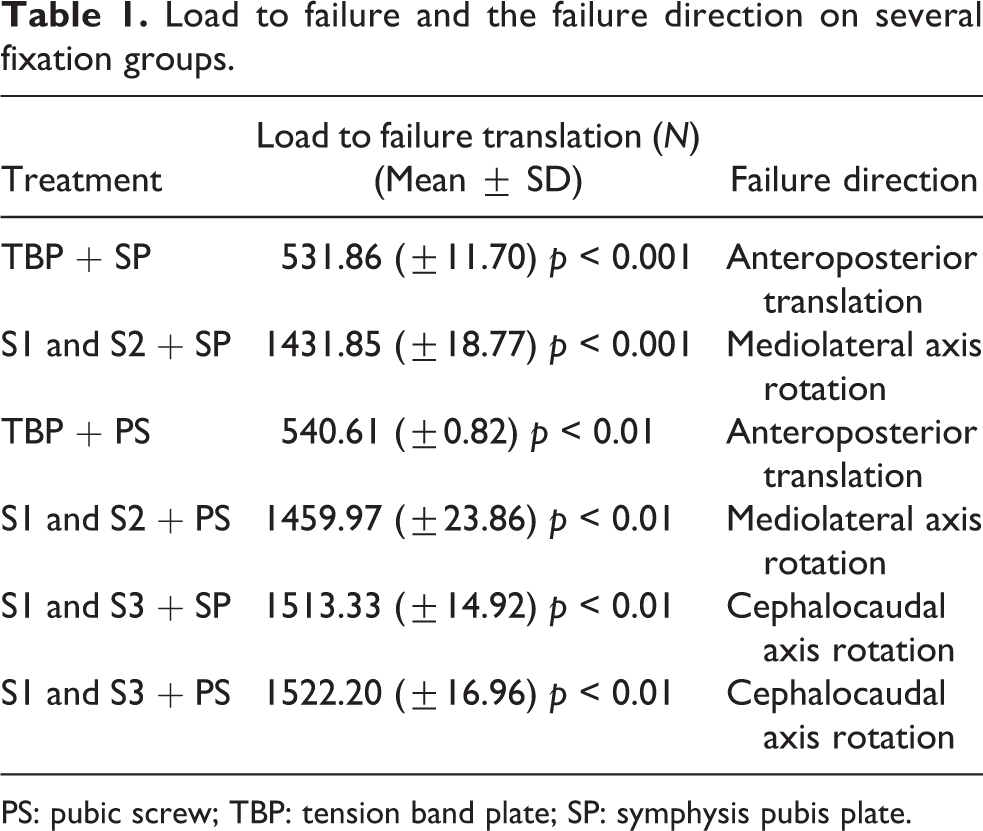
PS: pubic screw; TBP: tension band plate; SP: symphysis pubis plate.
Discussions
The study compared the rigidity of various types of fixation of pelvic fractures AO type C3 in which the axial force craniocaudal was given. All types of fixation in this study are often used in clinical practice. 11 –13 Several previous studies showed no consistent differences among the various types of fixation. 1,9 –11 Some of these studies used variable number of sample in human and some of them used cadaver. 4 ,14–17 This study used a model to simulate artificial pelvis vertical fracture of the sacrum and ipsilateral pubic ramus. The model is made of a special polyurethane material that can simulate the original structure of cancellous and cortical bone. Although the model does not have bone biomechanical properties similar to native bone that has a complex composition, some tests showed that the fracture on Synbone has a very similar response to the original bone towards the delivery of force and may simulate the mechanical properties of original human bone. The use of this Synbone aims to provide the material properties of the test sample to minimize the variability of test results between test samples. 9 ,17
Translational stiffness
Translational stiffness was defined as slope or gradient of load–displacement curve. 4 ,18 In this study, the assessment of stiffness and rigidity of the entire system fixation were measured at 25 N load to the point of failure. In this study, the load–displacement curve was found with variable translational vector to the point of failure and calculation of gradient was obtained through MSA software (SoftExpert company) on the analyser.
This study also showed that the lowest stiffness fixation was found in the group of TBP + SP (253.38 N/mm) and highest in the group S1-S3 IS + PS (830.36 N/mm). Translational stiffness in unstable pelvic fractures with vertical fracture of the sacrum becomes important than the rigidity of the rotation. The instability of the vertical axial force is more dominant than the cause of translational rotation. The difference in stiffness level between the various fixations according to the research conducted by Yinger et al. 9 stated that the fixation with TBP has a lower stiffness than the IS.
Translational rigidity is important because the ability of the patient to be able to weight bearing immediately after surgery depends mainly on the stiffness of the fixation and the ability to control micromotion. Stiffness of fixation depends on the configuration and materials and bone quality around fixation site. 19
The most dominant translational shifts were towards anterior, inferior and then lateral, which were suspected due to translational direction during axial weighting. Hence, translational direction upon axial weighting beside to craniocaudal (inferior) but also to anterior. In the application of TBP, there was less resistance to axial load in anteroposterior plane compared to IS plane because there was no implant to hold the fragment as such in the iliosacral group. Rotational shifts to the most dominant fragment happened when the sacral space opened. This could happen due to the parallel screw configuration on S1-S2, both located adjacent and parallel to mediolateral screw compared to S1-S3 placed divergently, hence rotational resistance towards mediolateral axis was larger in parallel screw configuration S1-S2.
Rotational stiffness
Rotational stiffness in this study was obtained in the same manner with the translational stiffness, although this study did not measure the rotation on the anteroposterior axis due to the limitations of the tool. Based on the calculation of the rotational stiffness, posterior fixation group with IS S1-S2 and IS S1-S3 showed no significant differences on fixation system rotational stiffness. However, there was a difference in the direction of failure between both groups; in which the axis of rotation of group IS S1-S2 rotated mediolateral or backward ilium to the medial fragment of sacrum while group IS S1-S3 rotated in craniocaudal axis or rotation of ilium out against medial fragment of sacrum. Effect of screw placement at iliosacral provides resistance to the rotation axis of mediolateral, this is because the centre point of craniocaudal axis is at S1, that is, the biggest stress point is at the top, hence the placement of the screws in S1 and S2 provides better resistance to the rotation axis of craniocaudal compared with placements in S1 and S3. 13 ,20 From this, it appears that there is a tendency to rotate the rotation axis of mediolateral. This is according to Abitbol 21 who concluded that primates evolved from quadripedal to bipedal experience progressive anterior inclination on the sacrum that showed the moment of the rotation on the horizontal axis or mediolateral at the level of the lumbosacral junction bipedal load conditions.
Load to failure on axial force
In all groups, there was no failure of fixation to the load of 500 N to represent the weight of the upper body or the weight is reduced with the weight of both adult's normal feet. 9 ,22 This shows that all types of fixation are able to withstand physiological loads and resilience against failure post-operative. In the results of this study in the fixation groups IS S1-S2 and IS S1-S3 is ranging from 1431.85 N to 1522.20 N, exceeding 950 N are said to be proportional to the force applied during weight bearing with one foot adult normal. 23,24 In the study by Gorczyca et al., 23 force required for the occurrence of failure may be greater in young adults due to better bone quality. The given load in this study is constant and linear, whereas differs on research conducted by Zwienen et al. 22 and Schildhauer et al. 19 who conducted cyclic loading on the model of the pelvic bone with a model of one-leg stance that represents fracture load received during the walk with full weight bearing. In their research, Schildhauer et al. 19 showed loosening of the IS after cyclic loading of 10,000 cycles at 363 N. In this study, it was found that no IS loosening occurs because there is no cyclic loading.
Although placement of IS in S1 and S2 is the best, according to Griffin et al., 3 4 of 30 patients with vertical fracture of the sacrum occurs implant failure in patients who do mounting IS in S1 and S2, where translation occurs on the field for more than a craniocaudal 1 cm and a large rotation occurs in a horizontal plane (mediolateral). According to Griffin, although IS can hold firmly to the lateral side of the fragment, it was unable to withstand the vertical shearing force greatly to the medial fragment of the sacrum as it is relatively small so that the failure occurred on repeated loading.
Studies conducted by Griffin et al. showed that the placement of the screws with the horizontal direction is not strong enough to withstand axial forces, so loosening of the screws occurs, especially around the medial side, and translational force can be converted easily into a rotational force to the rotary axis of the screw. 3 This is evidenced in this study where failure at all directions in fixation using IS occurs in the rotation.
The results of this study indicate that the use of IS on S1-S3 and screw pubis is superior to other methods in the case of unstable pelvic fractures with vertical fracture of the sacrum (AO type C1.3) and these results can provide recommendations on cases where good post-operative rehabilitation to avoid complications is needed. The advantages of using IS on an unstable pelvic injury, which is a minimally invasive technique used to provide benefits for the good preservation of soft tissue because of unstable pelvic fractures, are often accompanied by severe soft tissue damage. 25,26
The effect of anterior arch fixation type towards the fixation system stiffness
In the comparison shift between the pubic ramus fragment, no significant difference in displacement on the use of screws or plates symphysis pubis is found, but in absolute terms, the use of plate gives displacement slightly larger with an average difference of 0.02 mm compared with screw pubis. This is according to the research by Simonian et al. who compared the use of screws and plates symphysis pubis and showed no difference on both cases, 6 because almost the entire force acts on the posterior arch section. In this study, translation of pubic rami was measured from the anterioposterior shift which according to the research by Schildhauer et al. stating that there is a shift in the anteroposterior direction on all types of posterior fixation construction. 19 Uniform shift is caused by the same backward rotary axes, namely the cranial segment of the sacrum, the horizontal axis, mediolateral on condition of pelvic fractures with vertical instability. 22
In clinical use of screws, pubis provide advantages compared to the use of license plate required due to the use of plate wider exposure to the risk of injury to surrounding structures so that the use of screws pubis is recommended in cases with extensive soft tissue injury of the pelvis.
Due to the high incidence of pelvic fractures in young patients enduring high energy injury, our study used the normal non-osteoporotic Synbone, which would be considered as a representative. However, further studies are needed to evaluate pelvic fracture biomechanic in geriatrics.
Conclusions
Configuration of posterior fixation using IS S1-S3 and anterior fixation using screws pubis (PS) give the best fixation of pelvic fractures with vertical fracture of the sacrum (AO type C1.3). This configuration results in the best translational and rotational stiffness and the largest load to failure among six groups of the anterior and posterior fixation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by AO Trauma Asia Pacific Research Grant 2013 Ref: AOTAP13-07.