
Abstract
Purpose
The purpose of this study was to review pelvic fractures and concomitant orthopaedic injuries in children who have a patent triradiate cartilage (TRO) compared with children whose triradiate cartilage has closed (TRC). We hypothesise that these injuries will differ, leading to correlated alterations in management.
Patients and Methods
Using a database, we retrospectively reviewed patients aged below 18 years with pelvic fractures presenting to our Level 1 trauma center. Radiographs and CT scans were reviewed to identify orthopaedic injuries and categorise pelvic injuries using the modified Torode classification between the two groups.
Results
A total of 178 patients met inclusion criteria (60 TRO and 118 TRC). Mean age ± SD for TRO and TRC groups were 8 ± 4 years and 16 ± 2 years, respectively. TRO patients were more likely to present as a pedestrian struck by a vehicle (odds ratio (OR) 6.0; p < 0.001) and less likely to present after a motor vehicle collision (OR 0.2; p < 0.001). TRO patients were more likely to sustain rami fractures (OR 2.1; p = 0.020) and Torode IIIA injuries (OR 3.6; p < 0.001). They were less likely to sustain acetabular fractures (OR 0.5; p = 0.042), sacral fractures (OR 0.4; p = 0.009), hip dislocations (p = 0.002) and Torode IV injuries (OR 0.4; p = 0.004). TRO patients were less likely to be treated operatively for their pelvic (OR 0.3; p = 0.013) and orthopaedic injuries (OR 0.4; p = 0.006).
Conclusion
We suggest that patients with open triradiate cartilage are unique. Their pelvic injuries may be treated more conservatively as they have a greater potential for periosteal healing and bone remodelling. Patients with closed triradiate cartilage should be treated similarly to adults, as they share a similar mechanism of injury and need for operative fixation.
Introduction
Paediatric pelvic fractures are rare injuries with an incidence of 1 per 100 000 per year and represent 1% to 2% of fractures in children.1–6 Morbidity and mortality of these injuries are higher when compared with other fractures.7,8 Disruption of the pelvic ring results from high-energy mechanisms that warrant an extensive workup for associated injuries. Mortality in paediatric patients sustaining pelvic fractures is lower than their adult counterparts. 9 Fatal haemorrhage seen in adult patients with pelvic fractures is rare in the paediatric population. Instead, paediatric bleeding related to a pelvic fracture is typically due to solid-organ injuries, 10 making identification and treatment of these life-threatening injuries crucial.
The triradiate cartilage is the most important growth plate in the acetabular floor and closes between the ages of 12 and 18 years. Radiographic interpretation of the patency of the triradiate cartilage is an accurate method of determining skeletal maturity 11 and its patency is an important distinction when assessing pelvic and extremity injuries in paediatric patients. 12 The unfused innominate bone is considerably more flexible due to a higher cartilage content and greater elasticity both at the pubic symphysis and sacroiliac joints.13,14 The production of fractures requires great force, which presumably leads to a greater burden of concomitant injuries. 15
The classic classification system for paediatric pelvic fractures was developed by Torode and Zeig in 1985. Using radiographs alone, the classification divides injuries into four groups: (I) avulsion fractures; (II) iliac wing fractures; (III) simple ring fractures; and (IV) ring disruption fractures. 16 Shore et al modified the Torode classification by using CT scans in addition to radiographs. They further subdivided type III injuries into A and B. The III-A injury is a stable anterior ring fracture, while the III-B injury represents a stable injury that also involves the posterior ring. Type IV fractures include unstable injuries such as ring disruptions, hip dislocations and associated pelvic fractures combined with fractures of the pelvis and the acetabulum. 17 The modified classification system has been found to be predictive for significant morbidity and death in multi-trauma patients. 17
We performed a retrospective study to review pelvic fracture patterns and concomitant orthopaedic injuries in children who have an open triradiate cartilage (TRO) compared with children with a closed triradiate cartilage (TRC). We hypothesise that based on the patency of the triradiate cartilage, these injuries will differ, ultimately leading to differences in management.
Patients and methods
Following institutional review board approval, we utilised our institution's trauma database to identify patients between 2001 and 2014. The charts were reviewed by the authors. To be included in the study, patients were aged under 18 years and sustained a pelvic fracture from a blunt-force mechanism. Firearm injuries were excluded. Patients were divided into two groups: those with open triradiate cartilage (TRO) and those in which the triradiate cartilage had closed (TRC). Authors reviewed radiographs and CT scans to classify each patient's orthopaedic injuries, including pelvic injuries according to the Modified Torode Classification.
For each patient, the following epidemiological data were extracted: age; race; gender; time of presentation; mechanism of injury; Glasgow Coma Scale (GCS); Injury Severity Score (ISS); length of hospitalisation; need for surgical orthopaedic intervention; and disposition. Associated injuries were classified as injuries to: head/neck region; face; chest; abdomen; and extremities. The ISS was subdivided to calculate the Abbreviated Injury Scores (AIS) for the aforementioned body areas as well.
Differences between the two groups were analysed by mechanism of injury, critical injury by region, concurrent musculoskeletal related injury, pelvic injury type and Torode classification. Non-parametric analysis of categorical information was performed using a Chi-square test, unless an expected value was less than five, in which case Fisher's exact test was used. Odds ratios (OR) were generated with computation of confidence intervals (CI) using the Baptista-Pike method. Non-parametric analysis of continuous variables was performed using a Mann-Whitney U test. All analyses were performed using GraphPad Prism version 7.00 for Mac OS X (GraphPad Software, La Jolla, CA, USA; www.graphpad.com). In all tests, significance was set at p < 0.05.
Results
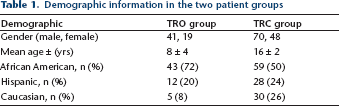
There were 60 patients in the TRO group and 118 patients in the TRC group met the inclusion criteria. Demographic information can be found in Table 1. Distribution of gender, race and hospital stay characteristics were comparable among both groups (Tables 1 and 2). The mortality rates for the TRO and TRC groups were 0% and 5.9%, respectively. Of the mortalities in the TRC group, three (42.9%) died of pelvic haemorrhage and exsanguination, one (14.2%) from lung injury and cause of death was unknown for three (42.9%). GCS and ISS values were calculated upon admission for each patient. While not significant, the highest ISS correlated with patients that were pedestrian struck in the TRO group and with those involved in a motor vehicle collision in the TRC group (Table 2). Over half of the patients in both groups sustained head injuries, with over 40% of them being classified as severe or critical. Patients in both groups who sustained chest trauma have a high likelihood (> 85%) of having these injuries classified as severe or critical.
Demographic information in the two patient groups
Variations in admission characteristics, mechanism of injury, critical injury by region, concurrent musculoskeletal related injury, pelvic injury and Torode classification
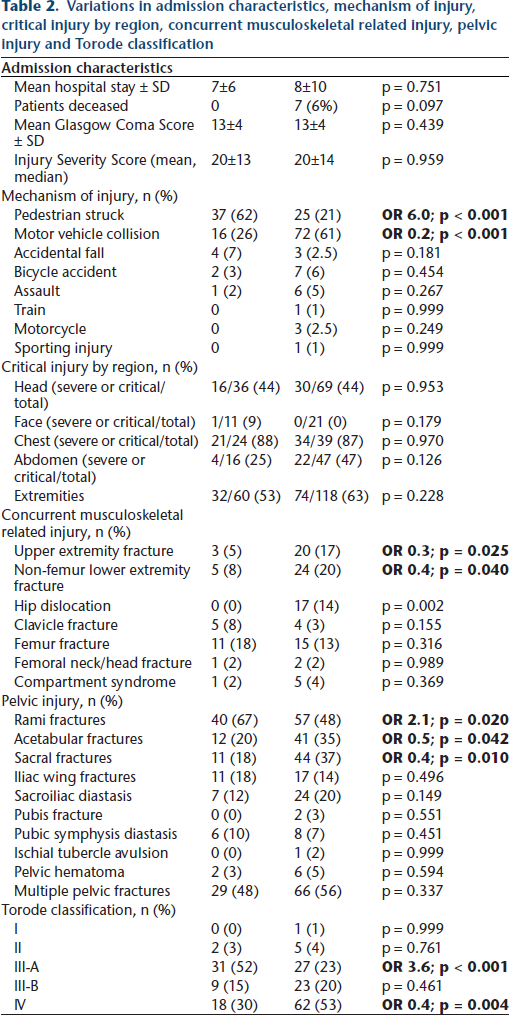
Significant variations were detected regarding mechanism of injury in patients with open (TRO) versus closed (TRC) triradiate cartilage (Table 2). Regarding mechanism of injury, TRO patients were more likely than TRC patients to present after being struck as a pedestrian (37/60 (62%) vs 25/118 (21%); OR 6.0, 95% CI 3.0 to 11.8; p < 0.001), while they were less likely to present after a motor vehicle collision (16/60 (26%) vs 72/1118 (61%), OR 0.2, 95% CI 0.1 to 0.5; p < 0.001). No differences were detected between the two groups when analysing the remaining mechanisms of injury (Table 2).
Significant variations were detected between the two groups regarding the presence of non-pelvic orthopaedic injuries (Table 2). TRO patients were less likely than TRC patients to sustain additional upper extremity fractures (3/60 (5%) vs 20/118 (17%), OR 0.3, 95% CI 0.1 to 0.8, p = 0.025) and non-femur lower extremity fractures (5/60 (8%) vs 24/118 (20%), OR 0.4, 95% CI 0.1 to 0.9; p = 0.040). The 17 TRC patients sustained a hip dislocation, compared with no hip dislocations among TRO patients (p = 0.002). No differences were detected between the two groups who presented with additional injuries (Table 2).
Significant variations were detected regarding additional pelvic injury patterns among patients with open (TRO) versus closed (TRC) triradiate cartilage (Table 1). TRO patients were more likely than TRC patients to sustain rami fractures (40/60 (67%) vs 57/118 (48%), OR 2.1, 95% CI 1.1 to 4.0; p = 0.020), while they were less likely to sustain acetabular fractures (12/60 (20%) vs 41/118 (35%), OR 0.5, 95% CI 0.2 to 0.9; p = 0.042) or sacral fractures (11/60 (18%) vs 44/118 (37%), OR 0.4, 95% CI 0.2 to 0.8; p = 0.097). No differences were detected between the two group in sustaining iliac wing fractures (p = 0.496), sacroiliac diastasis (p = 0.149), pubic fractures (p = 0.551), pubic symphysis diastasis (p = 0.451), ischial tubercle avulsions (p = 0.0.999), pelvic hematomas (p = 0.594) or multiple pelvic fractures (p = 0.337). When analysing pelvic fracture type by the Torode classification, TRO patients were more likely than TRC patients to sustain Torode IIIA fractures (31/60 (52%) vs 27/118 (23%), OR 3.6, 95% CI 1.8 to 6.9; p < 0.001), while they were less likely to sustain Torode IV fractures (18/60 (30%) vs 62/118 (53%), OR 0.4, 95% CI 0.2 to 0.7; p = 0.004).
TRO patients were less likely than TRC patients to be treated operatively for non-pelvic orthopaedic injuries (13/60 (21.7%) vs 50/118 (41.7%), OR 0.4, 95% CI 0.2 to 0.8; p = 0.006) and pelvic fractures (5/60 (8.3%) vs 28/118 (23.7%), OR 0.3, 95% CI 0.1 to 0.8; p = 0.013) (Table 3, Fig. 1). Among TRO patients undergoing operative pelvic fixation, all patients (100%) sustained posterior pelvic ring injuries, with one of these patients sustaining a concomitant acetabular fracture. Among TRC patients undergoing operative pelvic fixation, ten (35.7%) underwent fixation of acetabular fractures and 19 (67.9%) underwent fixation of posterior pelvic ring injuries (Fig. 1).
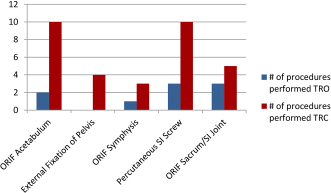
Operative pelvic procedures in the TRC group.
Operative extremity procedures in the TRO group
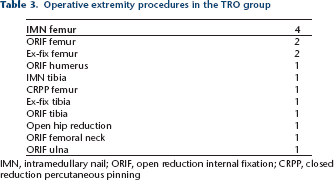
IMN, intramedullary nail; ORIF, open reduction internal fixation; CRPP, closed reduction percutaneous pinning
Discussion
Paediatric pelvic fractures vary in their presentation and treatment. Disruption of the pelvic ring results from high-energy mechanisms that warrant workup for associated injuries. The high incidence of concomitant injuries demands a multisystem approach.15,18–20
The patency of the triradiate cartilage is an important factor in determining how these patients are treated. We found that pelvic fracture patterns in children that have an open triradiate cartilage are significantly different than those whose triradiate has closed. There are limited data on the normal time of triradiate closure. Tonnis reported that it closes between the ages of 13 to 16 years in females and 15 to 18 years in males. 21 Dimeglio noted that the Risser sign may be misleading parameter and it is more accurate to correlate the closure of the triradiate cartilage (unpublished).
Previously documented mortality rates in paediatric pelvic fractures are in the range of 3.6% to 5%,10,12,22–24 although one study reported a mortality rate of as high as 25%. 25 The overall mortality rate in adults is reported to be around 17.5%.10,26 When comparing mortality rates due to pelvic fracture exsanguination, paediatric patients have a mortality rate of 0.3% compared with 3.4% in adults. 10 The differing rates of exsanguination may be explained by the mechanism of injury. Younger children, who are pedestrian-struck, likely experience a lateral compression type injury which is usually not associated with an increase in pelvic volume or haemorrhage. 12 Adult pelvic fractures are commonly sustained as a result of a motor vehicle collision with the driver or passenger sustaining injury. 12 Therefore, adult pelvic fractures often involve an anteroposterior (AP) directed force which may lead to an ‘open book’ type of injury, allowing for exsanguination due to increased pelvic volume. Our results support these findings as patients in the TRC group had an overall mortality rate of 5.9% and a mortality rate of 2.5% due to exsanguination while there were no mortalities in the TRO group.
While the skeletal maturity of the pelvis is the main contributing factor to fracture pattern, we found that the mechanism of injury also plays a role. Patients in the TRO group are more likely to sustain superior or inferior rami fractures and Torode type III-A fractures due to laterally directed forces that commonly occur from being struck by a vehicle. In the immature pelvis, the pelvic bone (ilium) tends to fail before the pelvic ligaments and may help to explain the low incidence of unstable ring injuries. 22
Patients in the TRC group are more likely to sustain acetabular fractures, sacral fractures, Torode type IV fractures and hip dislocations, independently. These injury patterns are likely due to AP directed forces that are encountered in a motor vehicle collision and mimic an AP compression type injury. Silber et al had similar findings as they found a significantly increased incidence of posterior pelvic ring injuries and acetabular fractures in patients who were skeletally mature. 22
In both groups, though not statistically significant, the mean ISS values for type III-B and IV fractures were higher than those of types I, II and III-A. Shore et al found similar findings. 17 When compared with the results of Shore et al, the proportion of type IV injuries were higher in our study, 10% versus 30% in the TRO group and 52.1% in the TRC group. This may be an indication that our patients experienced higher energy trauma.
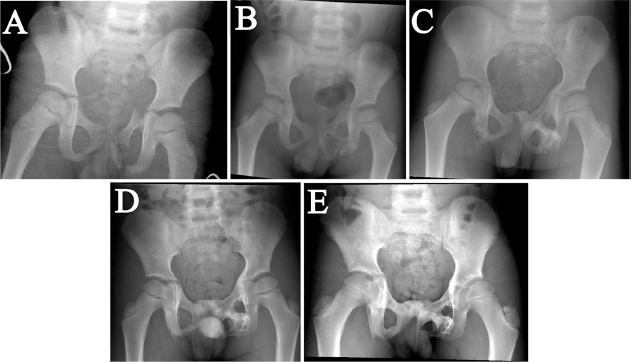
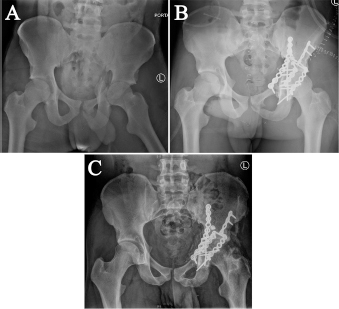
Patients in the TRO group were less likely to undergo operative intervention for both their pelvic and their non-pelvic injuries, independently. A possible explanation for this is that children have been found to tolerate bed rest and immobilisation better than adults. Symphyseal and sacroiliac disruptions may also be treated in a closed manner secondary to children's greater potential for periosteal healing and bone remodelling.2,27,28 The percentage of TRC patients treated with operative fixation for a pelvic injury in our study, 25.4%, is similar to that of adults at 28.1%. 29 In their series, Silber et al reported that all patients requiring operative fixation of pelvic fractures had a closed triradate cartilage. 22 Figure 2 shows a four year-old patient who was pedestrian-struck and was treated non-operatively while Figure 3 shows a skeletally mature 15-year-old patient with a similar injury that was treated operatively.
(
(
Our study has several weaknesses. First, as a retrospective study, there may be a treatment bias as surgeons may opt to treat similar injuries in different ways. We were not able to determine the extent of all extremity injuries as this information was not readily available in the medical record. Our study may also have inherent bias when presenting the high rate of severe associated injuries, as the rate of severe pelvic fractures was greater than the reported literature. 17 In the previously referenced study, patients were not separated based on their skeletal maturity. Nonetheless, our results highlight the importance of having a high index of suspicion for additional injuries in children with pelvic fractures.
To our knowledge, we report the largest cohort of children sustaining pelvic fractures. Our overall results are similar to Silber et al, 12 although they used plain radiography for fracture classification and to identify patency of the triradiate cartilage. All patients in our study had both radiography and a CT scan of their pelvis which ensures proper classification and identification of fracture patterns and patency of the triradiate cartilage.
Overall, we found that both skeletally mature and immature children who sustain pelvic fractures have injuries to multiple body organ systems with varying severity. We suggest that patients with an open triradiate cartilage are unique. Patients with a closed triradiate cartilage should be treated as adults, as they share similar mechanisms of injury, mortality rates, fracture patterns and an overall need for operative fixation. Regardless of skeletal maturity, it is essential for emergency providers, critical care teams and orthopaedic surgeons to identify pelvic fractures in paediatric patients as markers of high energy trauma, with a need to seek out associated injuries. Understanding the most common areas of concomitant injury should help focus secondary and tertiary exams in children presenting with pelvic fractures.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
We have no conflicts of interest to disclose. We received no additional funding for this study from any sources. This is a retrospective study; therefore, informed consent was not obtained.