
Abstract
Background:
We hypothesized that leucocyte esterase strip test can aid in diagnosing septic arthritis in native synovial fluid because leucocyte esterase concentrations would be elevated at the infection site because of secretion by recruited neutrophils.
Method:
The cohort included 27 patients (suspected septic arthritis and normal subjects). A standard chemical test strip (graded as negative, trace, +, ++ or +++) was used to detect the presence of leucocyte esterase. Fluid leucocyte count, Gram staining, culture, erythrocyte sedimentation rate and C-reactive protein were also assessed.
Results:
The leucocyte esterase test with a threshold of ++/+++ had a sensitivity of 79.2% (95% CI [confidence interval], 65.9% to 89.2%), specificity of 80.8% (95% CI, 73.3% to 87.1%), positive predictive value (PPV) of 61.8% (95% CI, 49.2% to 73.3%) and negative predictive value (NPV) of 90.1% (95% CI, 84.3% to 95.4%).
Conclusion:
The leucocyte esterase strip test yielded a high specificity, PPV, NPV, high sensitivity and high diagnostic accuracy. Leucocyte esterase is an accurate, quick and bedside test for septic arthritis and can be used effectively for diagnosing periprosthetic joint infections along with other battery of tests according to the Musculoskeletal Infection Society criteria.
Introduction
Acute monoarticular arthritis with or without fever is a common clinical problem encountered in emergency settings. Septic arthritis accounts for approximately 0.25% hospitalizations among children. Septic arthritis commonly occurs in persons of age group less than 20 years, 1 with 70% infections occurring between 1 month and 5 years of age and 50% occurring in children younger than 2 years of age. The incidence of septic arthritis is reported to be 5–71 per 100,000. 2,3
Septic arthritis requires a rapid diagnosis and early management by arthrotomy and joint lavage to prevent destruction of joint by proteolytic and other enzymes released by bacteria. Following conditions can mimic or present in the same manner as acute monoarticular septic arthritis –juvenile rheumatoid arthritis (JRA), transient synovitis, reactive arthritis, haemophilic arthropathy, Kawasaki syndrome, Henoch–Schonlein purpura, rheumatic fever with arthralgia, avascular necrosis, slipped capital femoral epiphysis, trauma, neoplasia, Lyme’s arthritis and Legg–Calve–Perthe’s syndrome. 4 –8 Therefore, it becomes a matter of great urgency to make a definitive diagnosis of septic arthritis.
At present the provisional diagnosis of septic arthritis is made on the basis of Kocher’s criteria, which includes high fever, inability to move the affected joint, total leucocyte count (TLC) > 12,000/mm3 and erythrocyte sedimentation rate (ESR) > 40 mm/h. 9 Depending on the number of criteria present, there is variable probability of septic arthritis being present. The diagnosis is confirmed by joint aspiration either direct or sonography-guided, its cell count, Gram’s stain and culture.
The Gram’s stain, though 100% specific, is only 45% sensitive for diagnosis of septic arthritis and takes around 40 min for the result. 10 So, overall there is no such test available, which is rapid, simple, easy to perform and can be done bedside, giving an accurate diagnosis of septic arthritis.
Leucocyte esterase test could be the answer. Leucocyte esterase enzyme is secreted by activated neutrophils, which are recruited at the site of infection. This enzyme is picked up by reagent strips specially designed for this. Leucocyte esterase test has been successfully used previously, as a bedside test in the diagnosis of urinary test infections since the early 1980s, 11 –13 pleural fluid, 14 subacute bacterial peritonitis, 15 bacterial meningitis, 16 bronchoalveolar lavage fluid 17 and middle ear effusion. 18 It has been used in orthopaedics for the first time in the case of periprosthetic infections 19 and proved to be of extreme importance (almost 100% specific).
So, it is hypothesized that leucocyte esterase enzyme can also be used to diagnose septic arthritis as it is simple, easy to perform, rapid and can be used as a bedside investigation.
Material and method
This prospective study was conducted from December 2013 to April 2015. Sample of convenience was taken during the study period.
Inclusion criteria – any age; acute monoarticular disease of major joint; clinical symptoms: acute onset, fever, limping while walking, unable to bear weight on the affected extremity, severe pain even on gentle passive movement, pseudoparalysis in children.
Exclusion criteria – poor skin condition; presence of sinus; presence of blood in aspirate (as if aspirate is bloody, the colorimetric test is not reliable); known case of haemophilia or any other bleeding disorder; patients who give definite history of antibiotic intake for the same condition; proven case of any other joint pathology.
Method
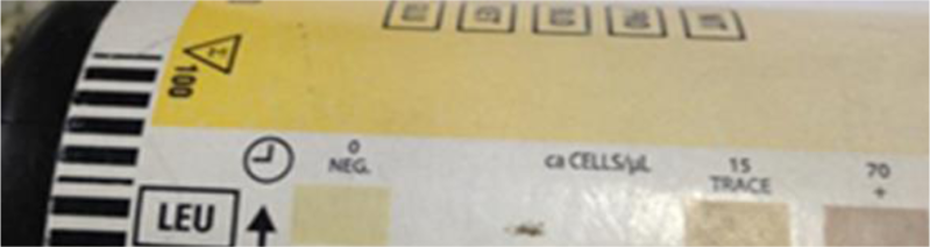
A written informed consent for joint aspiration and study inclusion was obtained. Joint was aspirated under aseptic condition and adequate local anaesthesia and the aspirate was poured over leucocyte esterase strip (MULTISTIX 10SG reagent strips). Waiting period before reading the result was 120 s. The colour change was appreciated and it was compared with the colour scheme provided on the strip box. Two such strips were used and analysed as per the standard procedure in such cases. The aspirate was also sent for Gram’s stain and culture for the final comparison and management of the patient. The strips used and method of reading them is shown in Figures 1 –4.

MULTISTIX 10SG reagent strips showing leucocyte esterase box.
How to read a negative test.

A 2+ reading of a test.

A 3+ reading of a test.
Outcome measures: If the strip shows colour change and Gram’s stain and culture were also positive, then it signified true positive result. If strip shows no colour change and Gram’s stain and culture were also negative, then it signified true negative result. If strip shows colour change but Gram’s stain and culture were negative, then it signified false-positive result. If strip did not show colour change but the culture and Gram’s stain were positive, then it signified false-negative result.
On the basis of true positives, true negatives, false positives and false negatives, sensitivity and specificity had been calculated.
Despite the whole process, the diagnosis and management of septic arthritis were done according to the conventional management protocols and not on the basis of the results of leucocyte esterase strip tests.
Results and observations
A total of 27 patients were included in the study as per the inclusion criteria. Sample size was dependent on the number of patients who met the inclusion criteria and presented within 17 months of the study period. The data related to the patients was collected and analysed. For comparison of percentages, chi-square test was used and for mean comparison unpaired t-test was used. Software used for statistical analysis was SPSS version 15.0.
The following results were obtained:
Septic arthritis is a disease that can occur in any age group but most cases occur before 20 years of age. This study also shows the same predilection of age distribution as most of our cases, that is, 67% were of <20 years of age with 7.4% cases occurring in <5 years of age.
Male to female ratio was 2:1 and the most common joint involved was the knee joint. In all, 70.3% patients showed raised TLC > 12,000/mm3; 25 out of 27 patients showed raised ESR, that is, 92.6% patients of suspected septic arthritis have ESR > 40 mm/h, which is a significant association.
In our study, 26 out of 27 patients showed raised C-reactive protein (CRP) while 1 patient shows CRP value less than 20 (normal CRP < 10 mg/L).
Aspiration of 27 joints done under total aseptic conditions and 22 out of 27 aspirates showed frank pus while rest 5 had clear to serous appearance.
Synovial fluid cell count is very important in diagnosing septic arthritis. Usually in cases of septic arthritis the TLC is >50,000/mm3 and in differential leucocyte count (DLC), polymorphonuclears (PMNs) are >75%. It is a very consistent association and in this study, PMNs >75% in DLC was shown by 26 out of 27 patients, that is, 96.3%, which is a significant association. The TLC of the synovial fluid in cases of septic arthritis is >50,000/mm3, but in our study the value of TLC was highly variable and was less than 50,000 in most of the patients. The mean value of synovial fluid TLC calculated in our study was 16,005/mm3 for culture-positive patients and 997/mm3 for culture-negative patients. Statistical relation between TLC, ESR and CRP in acute septic arthritis is shown in Table 1. The mean age of the patients, duration of symptoms before presentation, mean value of ESR, CRP, mean blood TLC and synovial fluid mean PMNs count is shown in Table 2.
Relation between blood TLC/DLC, ESR and CRP in acute septic arthritis.

TLC: total leucocyte count; DLC: differential leucocyte count; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein.
The mean age of the patients included in the study, duration of symptoms before presentation, mean value of ESR, CRP, mean blood TLC and synovial fluid mean PMN’s count.
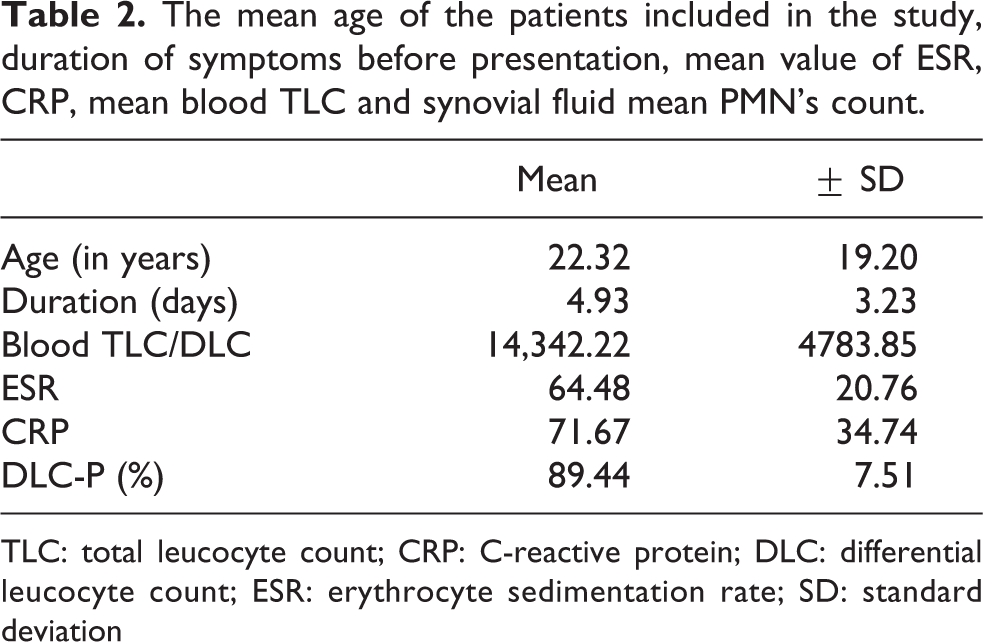
TLC: total leucocyte count; CRP: C-reactive protein; DLC: differential leucocyte count; ESR: erythrocyte sedimentation rate; SD: standard deviation
Gram’s stain is a useful and fast method of diagnosing septic arthritis but the sensitivity of Gram’s stain is very poor in diagnosing septic arthritis. In this study, only 3 out of 27 patients showed positive Gram’s stain, while 24 patients had negative Gram’s stain. In this study, 21 out of 27 patients showed positive culture, their culture showed growth of some microorganism responsible for septic arthritis.
The strip was dipped in the aspirated synovial fluid and the colour change was noted; 2+ and 3+ were considered to be positive results and negative or trace was taken as negative (shown in Figures 2 –4). Out of 27 patients, 22 showed positive results and 5 showed negative results.
Out of 21 culture-positive patients, 17 patients had TLC > 12,000 and only 4 had TLC < 12,000, 81% of culture-positive patients had raised TLC and only 19% had low TLC. While in 6 culture-negative patients, only 2 patients had TLC > 12,000 and 4 had TLC < 12,000 with the p value 0.012, which is significant.
A relationship between culture and ESR is obtained to show the effectiveness of raised ESR in diagnosing acute septic arthritis. Of the 21 culture-positive patients, 20 had raised ESR >40 mm/h, while only 1 had ESR <40 mm/h. In 6 culture-negative patients, 5 patients had raised ESR and only 1 had low ESR with the p value of the association is 0.163 which is not significant.
In this study, 20 patients had CRP elevated out of 21 culture-positive patients (95.24%) and only 1 had low CRP, while out of 6 culture-negative patients, all had raised CRP. The p value of the relation is 0.293 which is not significant.
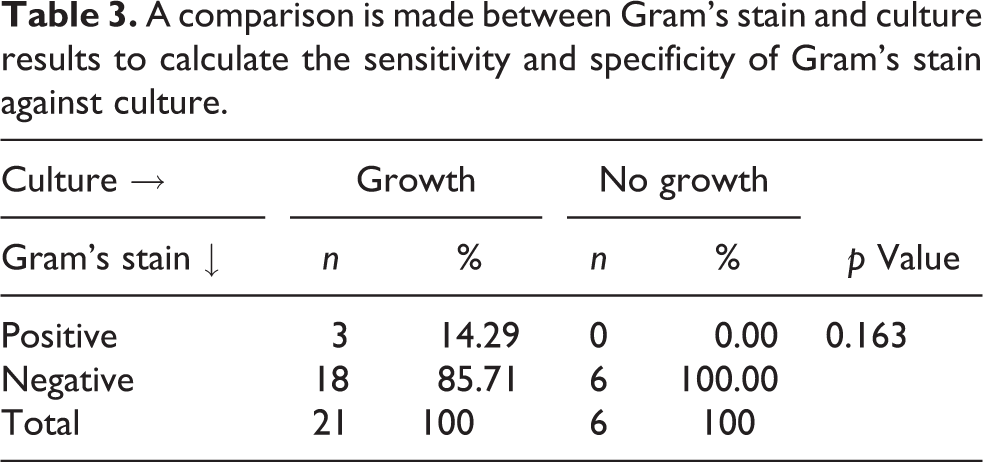
Sensitivity of Gram’s stain in the study came out to be only 14.29% though the specificity is 100%. Positive predictive value (PPV) is also 100%, but negative predictive value (NPV) is 25% with the diagnostic accuracy is 33.33%, which is not a good value for a test to be taken as screening or diagnostic test. Although it can be done within 45 min, the sensitivity of the Gram’s stain is too low to consider it a good test. A comparison is made between Gram’s stain and culture results to calculate the sensitivity and specificity of Gram’s stain against culture is shown in Table 3.
A comparison is made between Gram’s stain and culture results to calculate the sensitivity and specificity of Gram’s stain against culture.
Relationship between culture and leucocyte esterase strip colour change is calculated (shown in Table 4). Out of 21 culture-positive patients, leucocyte esterase strip showed positive result in all 21 patients, while in 6 culture-negative patients, only in 1 patient the strip showed positive result, and in the rest 5 patients the strip showed negative result.
Relationship between culture and leucocyte esterase strip colour change.

The sensitivity of the leucocyte esterase strip test in diagnosing septic arthritis is 100%. Specificity of the test is 83.33% with PPV 95.45% and NPV being 100%. The diagnostic accuracy of the leucocyte esterase strip test is 96.30% according to the data of this study.
Only one observer interpreted all the strip tests, so there was no inter-observer variability in this study. Intra-observer variability was calculated by kappa static and it was 0.67, showing substantial agreement.
Discussion
Septic arthritis is considered an emergency as it leads to the release of various proteolytic and other destructive enzymes by bacteria. It causes destruction of the articular cartilage and leads to pus formation inside the joint. It requires an early diagnosis and treatment with arthrotomy and joint lavage.
The diagnosis is essentially made on clinical grounds but there are conditions that closely mimic septic arthritis. 4 –8 That’s why certain rapid diagnostic tests are required.
The conventional practice in septic arthritis is to use Kocher’s criteria for predicting septic arthritis. Kocher’s criteria include high-grade fever (>38.5°), unable to bear weight on the affected extremity, raised blood TLC > 12,000/mm3, raised ESR > 40 mm/h. 9 CRP, which is an acute phase reactant, has also been an important tool in diagnosing acute infections. 20
Parvizi et al. 19 described leucocyte esterase test in 2011 for the diagnosis of periprosthetic joint infections. This test has been previously used successfully as a bedside test in the diagnosis of urinary test infections since the early 1980s, 11 –13 pleural fluid, 14 subacute bacterial peritonitis, 15 bacterial meningitis, 16 bronchoalveolar lavage fluid 17 and middle ear effusion. 18 This gave us intent to employ this leucocyte esterase test in the diagnosis of acute septic arthritis and this forms the basis of our study.
Cassidy et al. 21 and Henderson et al. 22 also documented that blood TLC and ESR are not a very good predictor of diagnosing septic arthritis as their value is very variable among patients of septic arthritis. In our study also, the p value of the association between ESR and culture positivity is 0.163, that is, not significant. Raised ESR, that is, > 40mm/h was present in both culture-positive and culture-negative patients.
In our study, the p value of the association between CRP and culture was also not significant, that is, 0.293. The value of CRP was high in both culture-positive and culture-negative patients. So, isolated CRP cannot be considered a good diagnostic marker. CRP is an acute inflammatory mediator that is raised in any other non-infective inflammatory conditions as well.
Gram’s stain is also considered a good diagnostic test but the sensitivity described by Faraj et al. 10 is around 45% only, though the specificity is very high (100%). In our study also, the sensitivity of Gram’s stain was only 14.29%, with the specificity being 100% and the diagnostic accuracy being only 33.33%. Out of 21 culture-positive patients, Gram’s stain was positive only in 3 cases. Gram’s stain takes at least 40 min to be performed 23 and due to its poor sensitivity it cannot be used as a diagnostic test.
Culture is gold standard for the definitive diagnosis of acute septic arthritis. It is positive in every case of septic arthritis unless patients had already received antibiotics. In our study, we had taken culture as a gold standard test, and all other tests are compared with the culture.
Synovial fluid TLC in our study had shown highly variable value. Only two samples had a value of TLC > 50,000/mm3. Rest all had very variable value. Few patients had values of 20,000/mm3 to 30,000/mm3 and few had values <10,000/mm3. Although the classical cut-off value of synovial fluid TLC is >50,000/mm3, it has been found to be very variable among the studies conducted previously. In 2004, Henderson et al. found that the value of joint white blood cells (WBC) is highly variable among the patients of septic arthritis and about one-third patients with septic arthritis have a synovial fluid WBC count <50,000/mm3. 22 The sensitivity of synovial fluid WBC is also only 64% in diagnosing septic arthritis.
The joint WBC cutoff in our study came out to be low, that is, 16,005/mm3. The other causes that may be responsible for the low synovial fluid TLC obtained in our study are technical drawbacks such as improper synovial fluid processing and delay in the synovial fluid processing. Another possible explanation for the low synovial fluid TLC could be that WBCs in the synovial fluid may get disintegrated in frank pus. In thick curdy pus, the concentration of cells could vary in various smears.
Leucocyte esterase test was used in orthopaedics for the first time ever in the diagnosis of periprosthetic joint infections by Parvizi et al. 19 In the diagnosis of periprosthetic joint infections, it has sensitivity of 80.6% and a specificity of 100% for a ++ strip reading. Similarly, Wetters et al. 24 found the leucocyte esterase strip test valuable with a sensitivity and specificity ranging from 92.9% to 100% and 77.0% to 88.8%, respectively, for the detection of periprosthetic joint infection. The leucocyte esterase strip test is a quick, easy-to-perform, cost-effective measure with high sensitivity and specificity.
In our study, the sensitivity of the leucocyte esterase strip test was 83.33%, which is very high. The specificity of the strip test was also 100%. Out of 21 culture-positive patients, this test was positive in all the 21 patients. Only in one patient who was culture-negative, this test came out to be positive. Even that patient had a history of 15–20 days and there is a probability that the patient had already received antibiotics leading to a negative culture. The PPV of the leucocyte esterase strip test was 95.45% and NPV was 100%. The overall diagnostic accuracy of this test when performed alone was 96.30%, which makes it a good test. There are several factors that make it a perfect test for diagnosing acute septic arthritis; first of all, it is very easy to perform with no expertise required, as after dipping the strip into the synovial fluid only colour change is to be noted and compared with the colorimeter, which does not need any technical expertise. It is a rapid test that takes only 120 s for the strip to change colour, while other test such as Gram’s stain takes at least 40 min. Synovial fluid aspirate culture takes at least 48 h, which beats the purpose of a rapid diagnostic test. Also the strip used is not very costly, it costs around 15 rupee per strip.
Added advantage of leucocyte esterase test over culture may be that culture is negative in patients who have already received antibiotics as the culture is based on the detection of the microorganism, while leucocyte esterase test can still be positive as it is based on the detection of leucocyte esterase enzyme secreted by activated neutrophils.
Out of a total of 27 cases, which fulfilled the Kocher’s criteria for the diagnosis of septic arthritis, 5 patients had clear looking synovial fluid on arthrotomy, negative Gram’s stain, negative culture and also negative leucocyte esterase test. Synovial fluid TLC in these patients was also low, that is around 997/mm3. Despite the high ESR and CRP, leucocyte esterase test was negative in these patients. Although the Gram’s stain and culture was also negative in these patients but the reliability of Gram’s stain is very poor and the culture takes at least 48 h. While, leucocyte esterase test can be done within 120 s and is highly reliable too. These cases proved to be non-infective later on and probably did not need arthrotomy. The possible diagnosis in such cases could be JRA and transient synovitis, but the arthrotomy was done on the basis of Kocher’s criteria. So, with the availability of our test and its usefulness, such unnecessary arthrotomies can possibly be avoided in the future.
Few limitations of our study are – sample size was small due to the limitation of the study period, leucocyte esterase strip specificity is high but PPV is low and this test is unreliable if the aspirate has blood.
Conclusion
Leucocyte esterase is a rapid, efficient, bedside (easy to perform), cost-effective test with good sensitivity 83.33% and excellent specificity of 100%. It can be used reliably as a single test for diagnosing septic arthritis. This test can also be useful in differentiating acute septic arthritis from other conditions such as JRA and transient synovitis, which have similar presentation and guide us to the correct treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.