
Abstract
We report a case of bilateral external iliac artery compression after application of subcutaneous anterior pelvic fixation (INFIX) technique in a 51-year-old male with an unstable pelvic fracture sustained following a motor vehicle accident. This has not been previously reported in the literature. The management of this complication is discussed in detail, along with key precautions and technical steps to consider while utilizing the ‘INFIX’ technique for pelvic fractures.
Introduction
A technique for subcutaneous anterior pelvic fixation for unstable anterior pelvic ring fractures has recently been reported in the literature and has been called the INFIX. 1 It consists of supra-acetabular pedicle screws connected by a subcutaneous rod. It allows temporary anterior fixation when combined with posterior stabilization if indicated, and can be removed after 3–4 months. 2 It can reduce the potential complications usually associated with external fixation of unstable pelvic fractures. It can also improve patient tolerance due to lack of external metalwork and allows mobilization.
The complications such as femoral nerve palsy 2,3 and post-operative infection have been reported following this newer INFIX device. However, we are not aware of any reports of vascular complications following this procedure to date. We report the case of an immediate bilateral lower limb arterial compression following internal fixation of a pelvic fracture using a subcutaneous anterior internal pelvic fixation (INFIX) technique.
Case history
A 51-year-old, obese, Caucasian male presented to the emergency department with a polytrauma following a motor vehicle accident. The primary survey revealed grade II shock which responded to crystalloid resuscitation, bilateral chest injuries requiring chest drains, suspicion of pelvic fracture stabilized with temporary pelvic binder and a right open tibia fracture initially managed according to British Orthopaedic Association (BOA)/British Association of Plastic Reconstructive and Aesthetic Surgeons (BAPRAS) open fracture guidelines. 4 A trauma protocol computerized tomography (CT) scan and plain radiographs identified bilateral chest injuries with flail segments, a retroperitoneal haematoma, anterio-posterior compression (APC) III pelvic fracture (Figure 1) and a grade IIIB open right tibial diaphysis fracture. The abdominal CT scan ruled out any other intra-abdominal injuries.

Reformatted image from trauma protocol pelvic CT scan confirms unstable APC III pelvic fracture with symphysis widening, pubic rami fracture and left sacroiliac joint injury. CT: computerized tomography; APC: anterio-posterior compression.
An emergency stabilization of his pelvic fracture was performed using a subcutaneous anterior pelvic fixation (INFIX) device (ARMADA®, NuVasive UK Ltd, Herts, UK). Two supra-acetabular 7-mm pedicle screws were inserted into the ilium anteriorly and an anterior subcutaneous pelvis internal fixator (ASPIF) attached. The left sacroiliac joint was stabilized percutaneously using a 6.5-mm cannulated screw (Depuy Synthes©, Switzerland). The right open tibia fracture was stabilized with a temporary external fixation device after wound debridement. The procedures were carried out by two senior trauma surgeons without any intraoperative difficulties. However, immediately following the operation, on removal of the surgical drape, there was mottling of the left leg and loss of palpable pulses on left side (Figure 2). The right leg was also slightly mottled but the posterior tibial and dorsalis pedis pulses were present.

(a) A clinical photograph demonstrating mottling of left lower limb prior to revision of INFIX. (b) A clinical photograph of same limb with resolution of mottling after revision.
After immediate consultation with a senior vascular surgeon, an urgent CT angiogram was performed which identified bulging of the rectus muscles underneath the ASPIF and subsequent compression of the external iliac arteries against the ASPIF anterior bar bilaterally but more pronounced on left side (Figure 3).

CT angiogram image showing compression of external iliac vessel by metal bar (see arrow). CT: computerized tomography.
A team of vascular and trauma surgeons performed an immediate exploratory procedure to reinstate lower limb circulation. Initial exploration of bilateral femoral triangles revealed an absent femoral pulse on the left side and reduced pulsation on the right using an intraoperative Doppler device. A femoral arteriotomy was performed on the left side and a Fogarty® catheter (Edwards Lifesciences LLC, Irvine, California, USA) was passed distally to rule out distal embolic occlusion. An excellent blood backflow was observed. The ASPIF device was immediately removed which led to resumption of blood flow bilaterally and triphasic Doppler signals were obtained distally. The ASPIF was adjusted to increase its arc of curvature and reapplied. However, the pelvic diastasis could not be fully reduced safely (Figure 4) as this resulted in immediate loss of triphasic Doppler signals from femoral vessels bilaterally. The ASPIF was therefore secured in place with blood flow maintained and good Doppler signals distally. Intraoperative stress views of the pelvis confirmed a stable construct with no evidence of further instability. The lower limb mottling resolved spontaneously (Figure 2(b)), distal pulses were palpable bilaterally and there was no sign of compartment syndrome at the end of the procedure. A nasogastric tube was inserted to decompress post-operative ileus and avoid intra-abdominal hypertension.
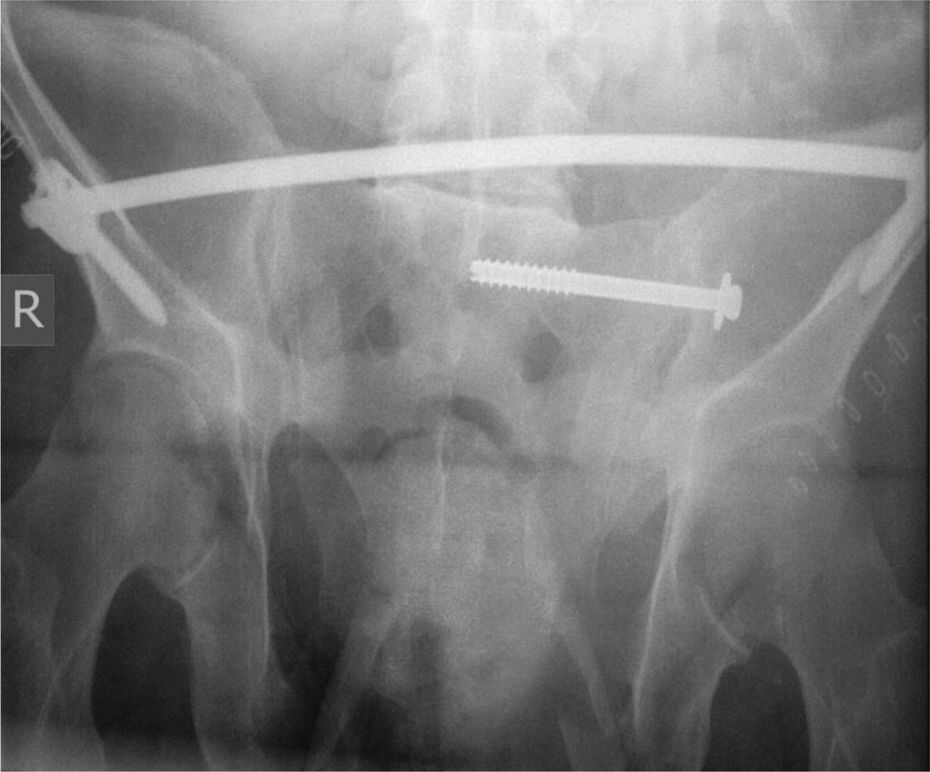
Post-operative radiograph demonstrating INFIX device and sacroiliac screw in situ with residual widening of symphysis.
The patient continued his post-operative recovery on the intensive care unit uneventfully. Three days later, he underwent definitive intra-medullary nailing of his right tibial diaphyseal open fracture with soft tissue flap reconstruction at the regional orthoplastics unit. Definitive internal fixation of pelvic fracture with anterior pelvic plating was performed on day 7 after the injury (Figure 5). A three-month follow-up confirmed satisfactory progress, and full weight bearing has now commenced with the help of a crutch and continued physiotherapy.

A pelvic radiograph demonstrating definitive fixation of pelvic fracture.
Discussion
The INFIX technique has gained a significant popularity as an alternative to pelvic external fixation in recent years for the treatment of unstable pelvic fractures. The senior author adopted this technique 2 years ago and has successfully utilized this technique to treat unstable pelvic ring injuries without any major complications in the past. The complications of femoral nerve injury and post-operative infection rates up to 4% have been reported. 2,5 The complication of vascular compression has not been reported so far, though a review of post-operative CT scans by Merriman et al. showed that on average, the vascular bundle sat 2.2 cm deep to the bar. 6 Apivatthakakul and Rujiwattanapong suggested positioning the rod above the rectus femoris fascia, leaving enough space for the underling neurovascular bundle. 7
We identified various potential reasons for this complication in our reported case. Due to the patient’s body habitus, the ASPIF anterior bar may not have been adequately contoured, therefore reducing pelvic girth. This can result in compression of underlying structures, which can be potentiated by increases in intra-abdominal volume due to post-injury ileus. Vascular compression in this case could potentially have been prevented by adequate contouring of the anterior bar and intestinal decompression.
The traditional square-shaped sterile draping of the pelvis did not allow immediate identification of vascular compression. An aseptic preparation of both lower limbs with full exposure could have identified immediate vascular compromise once the pelvis was reduced with a potentially under-contoured ASPIF bar. The confirmation of palpable pulses before and after securing ASPIF bar could have prevented the unnecessary delay of obtaining CT angiogram to confirm the diagnosis.
This is the first reported case of vascular compromise following anterior subcutaneous pelvic internal fixation, and highlights a number of important learning points which should be considered in all cases when performing this technique. These have been summarized as follows: (1) A nasogastric tube should be considered to prevent potential abdominal distension. (2) During surgical draping, both lower limbs should be left exposed to carry out frequent vascular examination of both lower limbs including skin changes and arterial pulsation throughout the procedure. (3) A sterile ultrasound Doppler device should be available to confirm maintenance of triphasic arterial response after application of ASPIF anterior bar. (4) Ensure the ASPIF anterior bar is truly subcutaneous when inserted. (5) When contouring the bar, adequate curvature of the bar should be ensured to prevent compression of internal pelvic structures when the pelvis is reduced. (6) Take additional care in obese patients or patients with a distended abdomen when inserting the bar. (7) If there are any concerns of vascular compromise during or after the procedure, a vascular surgeon should be consulted and an urgent CT angiogram obtained. (8) A meticulous observation is required during immediate post-operative period to ensure patency of vasculature and allied staff must be informed about importance of frequent vascular examinations.
Conclusion
We believe that the INFIX technique is a useful option for the treatment of unstable pelvic ring injuries and by making the above considerations prior to surgery, the potential vascular complications can be avoided.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.