
Abstract
Purpose:
How the symptomatology of lateral femoral cutaneous nerve (LFCN) injury changes after total hip arthroplasty (THA) via direct anterior approach (DAA) is not known. Our hypothesis was that the symptoms of LFCN injury after THA via DAA in longer follow-up periods would resolve spontaneously, leading to an improved quality of life (QOL). The aims of this study were to investigate how the symptom LFCN injury changed after DAA–THA, and how those changes affected QOL.
Methods:
We investigated the incidence of LFCN injury after DAA–THA using self-reported questionnaires at two time points (initial survey: August 2014, present survey: August 2015). QOL was assessed by the Western Ontario and McMaster Universities Osteoarthritis Index, the Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire, and the Forgotten Joint Score-12 (FJS-12). Types (dysesthesia or hypesthesia) and changes of the symptom were surveyed.
Results:
About 122 hips at average12.8 months postoperatively (initial survey), and of those, 89 hips at average 26.2 months postoperatively (present survey) were analyzed. The incidence of LFCN injury decreased significantly, from 31.9% to 11.2% (p < 0.001). Spontaneous improvement of symptoms was seen in 96%. The difference of FJS-12 between patients with and without LFCN injury at the initial survey disappeared at the present survey. The dysesthesia group showed significant correlations between rate of improvement in LFCN injury and increase of QOL.
Conclusion:
Most symptoms of LFCN injury resolved spontaneously with longer follow-up periods. In particular, improvement of dysesthesia as a symptom of LFCN injury was associated with better QOL.
Keywords
Introduction
The direct anterior approach (DAA), which is an intermuscular and internervous approach to the hip joint, requires no muscle transection. The advantages of DAA for total hip arthroplasty (THA) include less soft tissue trauma, less postoperative pain, earlier postoperative functional recovery, and lower dislocation rate compared with other approaches. 1 –5 Although DAA for THA has gained popularity in recent years, it has also been associated with some notable complications, 3,6 –9 one of which is injury to the lateral femoral cutaneous nerve (LFCN). 2,10 –12
The LFCN is a pure sensory nerve supplying the cutaneous area of the anterolateral thigh. Injury to the LFCN can result in hypesthesia or, in some patients, pain or dysesthesia in the anterolateral aspect of the thigh.
The LFCN either crosses the intermuscular space between the tensor fascia latae (TFL) and sartorius muscles or lies within it. Because the surgical interval for the DAA is the intermuscular space between the TFL and sartorius muscles, the LFCN is always in the vicinity of the surgical field and is at risk of injury. 2,10,11
In our 2014 cross-sectional analysis of 122 hips on which THA via DAA was performed, we found an incidence of LFCN injury of 31.9% approximately 12 months postoperatively and lower quality of life (QOL) in patients with LFCN injury than in those without. 12 However, the follow-up period was relatively short, and it is not known how the symptomatology of LFCN injury changes over a patient’s clinical course. We therefore conducted the present extended longitudinal study to determine (1) whether the symptoms of LFCN injury persisted over an extended follow-up period and (2) how the symptoms of LFCN injury affect patient-reported outcomes (PROs) during that time. We hypothesized that with longer follow-up periods, the symptoms of LFCN injury after THA via DAA would resolve spontaneously, leading to an improved QOL. The aims of this longitudinal study were to investigate how the symptomatology of LFCN injury changed over the clinical course and how those changes affected QOL.
Materials and methods
Investigation of LFCN injury
Initial survey (August 2014): As we reported previously, 12 we designed and sent a self-administered questionnaire to prospectively investigate the incidence of LFCN injury and QOL via PRO measurements (Figure 1). From 2011 to 2014, we performed primary THA via DAA on 122 patients in our department. These 122 patients were included in the initial assessment. We defined LFCN injury as the presence of symptoms over the lateral aspect of the thigh, excluding the area of the operative scar. Patients were asked (1) if they had experienced any discomfort in the thigh after surgery, (2) details of the discomfort (numbness, dull sensation, tingling or jolt-like sensation, pain, or strange feeling), (3) whether the discomfort had disappeared.

Study flowchart.
Present survey (August 2015): One year after the initial survey, the same questionnaire used in the initial survey was sent to the same patients to assess the incidence of LFCN injury and changes in QOL. To analyze LFCN injury more precisely, symptoms of LFCN injury were classified into two groups: (1) dysesthesias such as pain, tingling, and jolt-like or other strange sensation (dysesthesia group) and (2) hypesthesias such as numbness and dull sensation (hypesthesia group). Changes in symptoms during the interval between completion of the two surveys were assessed using a visual analog scale (VAS) score ranging from 0 (no change in symptoms) to 10 (complete disappearance of symptoms).
Assessment of the effect of LFCN injury on QOL using PROs
PRO tools were assessed at the initial and present surveys using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) (pain, stiffness, and function subscales), 13 the Japanese Orthopaedic Association (JOA) Hip Disease Evaluation Questionnaire (JHEQ), 14 the Forgotten-Joint Score-12 (FJS-12), 15 and patients’ questionnaire responses. The WOMAC, first reported by Bellamy and Buchanan in 1986, is used worldwide to evaluate the lower limbs, particularly the hip and knee joints, and has a total score range from 0 (best) to 96 (worst). 13 The JHEQ is a validated self-administered questionnaire evaluating QOL of Asian-lifestyle patients with hip disease; the total score range is from 0 (worst) to 84 (best). 14 The FJS-12, another self-administered questionnaire, is a specific and very subjective PRO tool that assesses patients’ awareness of their knee or hip joint during activities of daily living. Its final score range is from 0 (worst) to 100 (best). 15
Changes in the PROs between the first and present assessments were calculated to determine whether those changes related to symptom improvement in patients with LFCN injury.
Direct anterior approach
All surgeries were performed by four hip surgeons using the same surgical protocol. DAA was performed with the patient in the supine position on a standard surgical table. 16 The skin incision began 2 cm lateral and distal to the anterior superior iliac spine and proceeded distally for up to 10 cm along a line angling toward the head of the fibula. Briefly, the fascia of the TFL muscle was incised about 2 cm lateral to the skin incision to prevent LFCN injury, and the intermuscular space between the TFL and sartorius muscles was bluntly entered. The anterior articular capsule was exposed, incised, and resected as much as possible to expose the femoral head. For stem insertion, the surgical table was extended so that the hip joint could be extended to 15°. The superior and posterior portions of the articular capsule were partially incised so that the greater trochanter could be elevated with a retractor. Finally, the size and stability of the implant were confirmed intraoperatively under fluoroscopy.
Statistical analysis
The highest scores (indicating the best results) for both the WOMAC and JHEQ are 0 and 84. Therefore, the lowest and highest scores for each questionnaire were converted to 0 and 100, respectively.
To assess the impact of LFCN injury on patient QOL, we used the Mann–Whitney U test to compare differences in the PROs between patients reporting LFCN injury, versus those with no symptoms, at the second assessment. We used the Wilcoxon signed-rank test to assess the changes in PROs during the interval between the two assessments in patients with and without LFCN injury at the initial assessment. We assessed the correlation between the rate of improvement in symptoms and the changes in PRO scores for those patients who reported LFCN injury using Pearson’s r. All statistical analyses were performed using IBM SPSS Statistics for Mac IBM Corp., Armonk, NY, USA).
Results
For the initial survey, 12 a total of 122 hips were analyzed at a mean of 12.8 months postoperatively. Of the 122 questionnaires sent to the patients, 90 replies were received for the present survey. Of those, one patient was excluded because the symptom was considered peri-incisional sensory change rather than LFCN injury. Thus, 89 hips (15 male, 74 female; mean age at surgery 66.3 years (range, 35–88 years)) were analyzed in the present survey. The mean follow-up period at the time of the present survey was 26.2 months (range, 14–42 months).
Incidence of the LFCN injury and its detail
The incidence of LFCN injury decreased significantly from 31.9% (39 of 122 hips) to 11.2% (10 of 89 hips) (p < 0.001). In the initial study, the main symptoms of LFCN injury were hypesthesia (53.8%) and dysesthesia (46.2%); however, the main symptoms of LFCN injury in the 89 hips in the present survey were hypesthesia (70%) and dysesthesia (30%) (Table 1).
Result of the incidence and detail of LFCN at the initial and the present study.
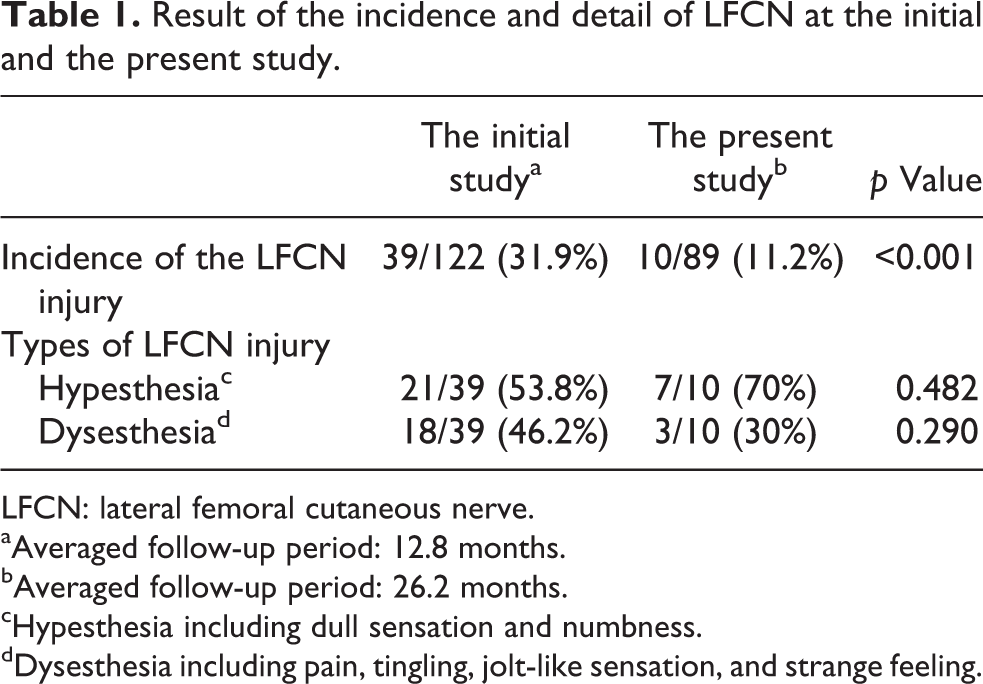
LFCN: lateral femoral cutaneous nerve.
aAveraged follow-up period: 12.8 months.
bAveraged follow-up period: 26.2 months.
cHypesthesia including dull sensation and numbness.
dDysesthesia including pain, tingling, jolt-like sensation, and strange feeling.
At the initial survey, there were 25 hips with and 59 hips without LFCN injury. Of the 25 with LFCN injury, 24 hips (96%) had spontaneous improvement of symptoms, 15 of which (60%) displayed complete resolution at the second survey. The rate of improvement of LFCN injury, assessed using VAS scores, was significantly greater in the dysesthesia group than in the hypesthesia group (p = 0.03; Table 2).
Result of visual analog scale of improvement of the LFCN injury between two survey points, in which 10 indicates that the symptoms are gone completely and 0 indicates that the symptoms are not changed at all.
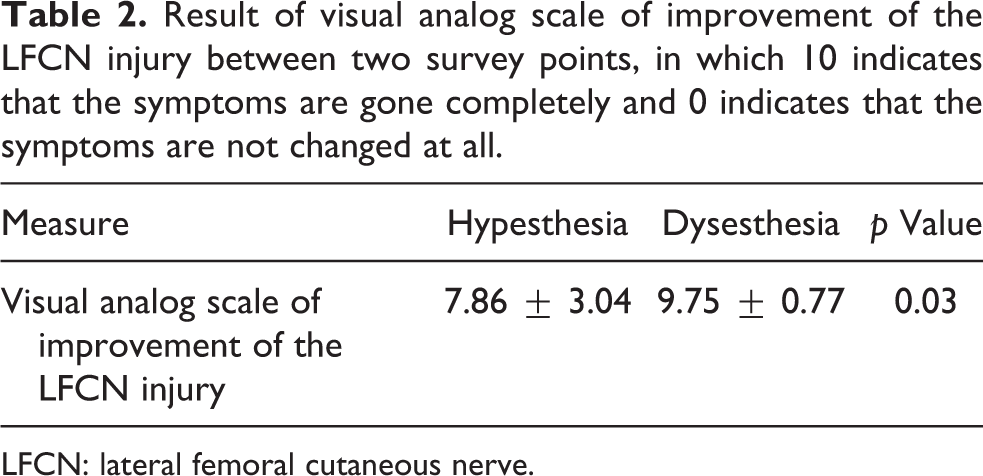
LFCN: lateral femoral cutaneous nerve.
Assessment of the effect of LFCN injury on QOL using PROs
In regard to PROs at the initial survey, there was a nonsignificant tendency for patients with LFCN injury to have a lower JHEQ than those without (63.6 ± 19.6 for hips with LFCN injury vs. 70.8 ± 22.9 without, p = 0.13), and there was no difference in the mean WOMAC score between the two groups (84.1 ± 14.7 for hips with LFCN injury vs. 86.6 ± 16.9 without, p = 0.53). Although mean FJS-12 score differed significantly between patients with and without LFCN injury at the initial survey (50.9 ± 25.3 for hips with LFCN injury vs. 64.3 ± 25.7 without, p = 0.01), the difference had disappeared by the time of the second assessment (58.6 ± 26.9 for hips with LFCN injury vs. 65.7 ± 28.2 without, p = 0.32; Table 3).
Result of patients reported outcomes at the present survey in patients with or without lateral femoral cutaneous nerve injury at the initial survey.
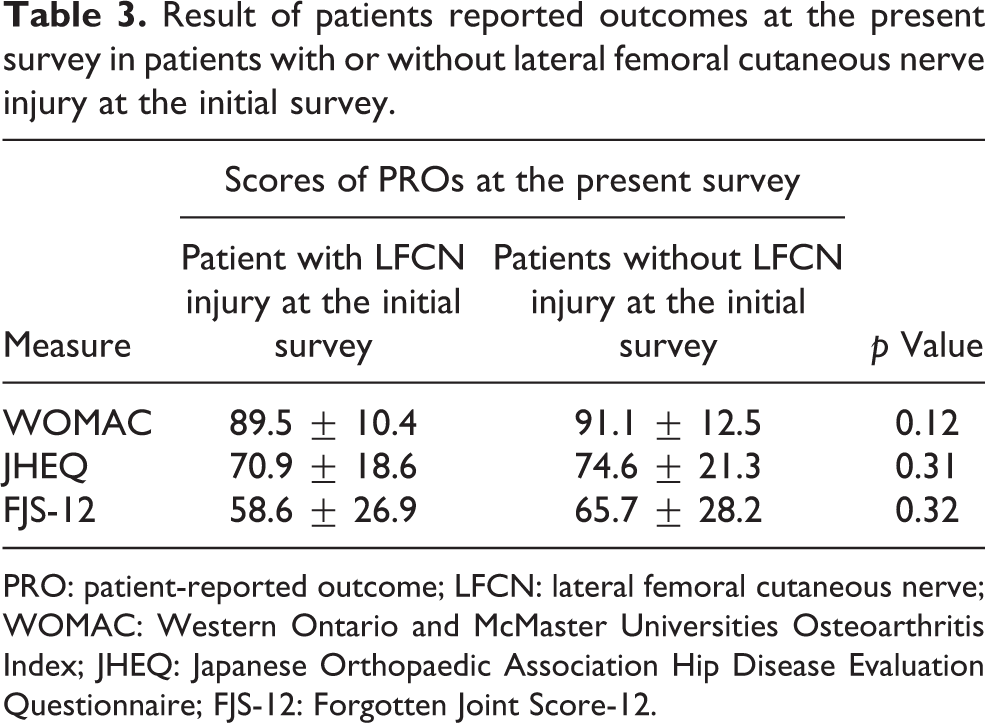
PRO: patient-reported outcome; LFCN: lateral femoral cutaneous nerve; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index; JHEQ: Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire; FJS-12: Forgotten Joint Score-12.
Table 4 shows the results of all PROs for LFCN-injured hips between the initial and present surveys. Significant improvements were seen in WOMAC (p = 0.005), JHEQ (p = 0.003), and FJS-12 (p = 0.02). However, in hips without LFCN injury at the initial survey, there were no differences in PROs between the initial and present surveys (Table 4).
Comparison with result of patients reported outcomes in patients with or without lateral femoral cutaneous nerve injury at the initial and present study.
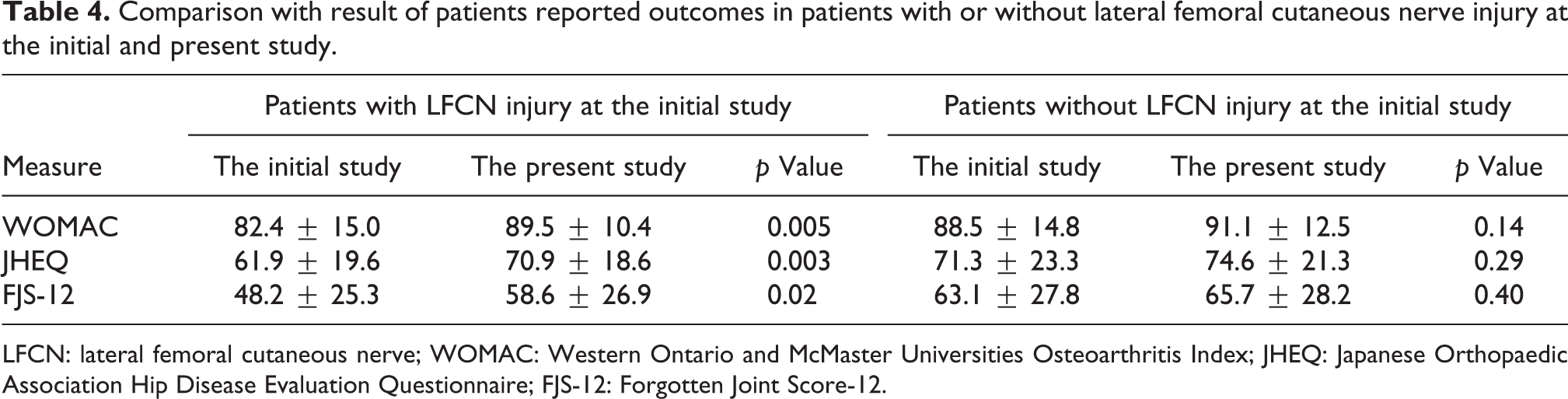
LFCN: lateral femoral cutaneous nerve; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index; JHEQ: Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire; FJS-12: Forgotten Joint Score-12.
With regard to the correlations between improvement in LFCN injury and changes in PROs (Figure 2), in the dysesthesia group, there were significant correlations between the rate of improvement in LFCN injury and each PRO (WOMAC: r = 0.620, p = 0.03; JHEQ: r = 0.563, p = 0.02; FJS-12: r = 0.549, p = 0.04). On other hand, there were no significant correlations in the hypesthesia group (WOMAC: r = 0.205, p = 0.26; JHEQ: r = 0.137, p = 0.30; FJS-12: r = 0.003, p = 0.49).
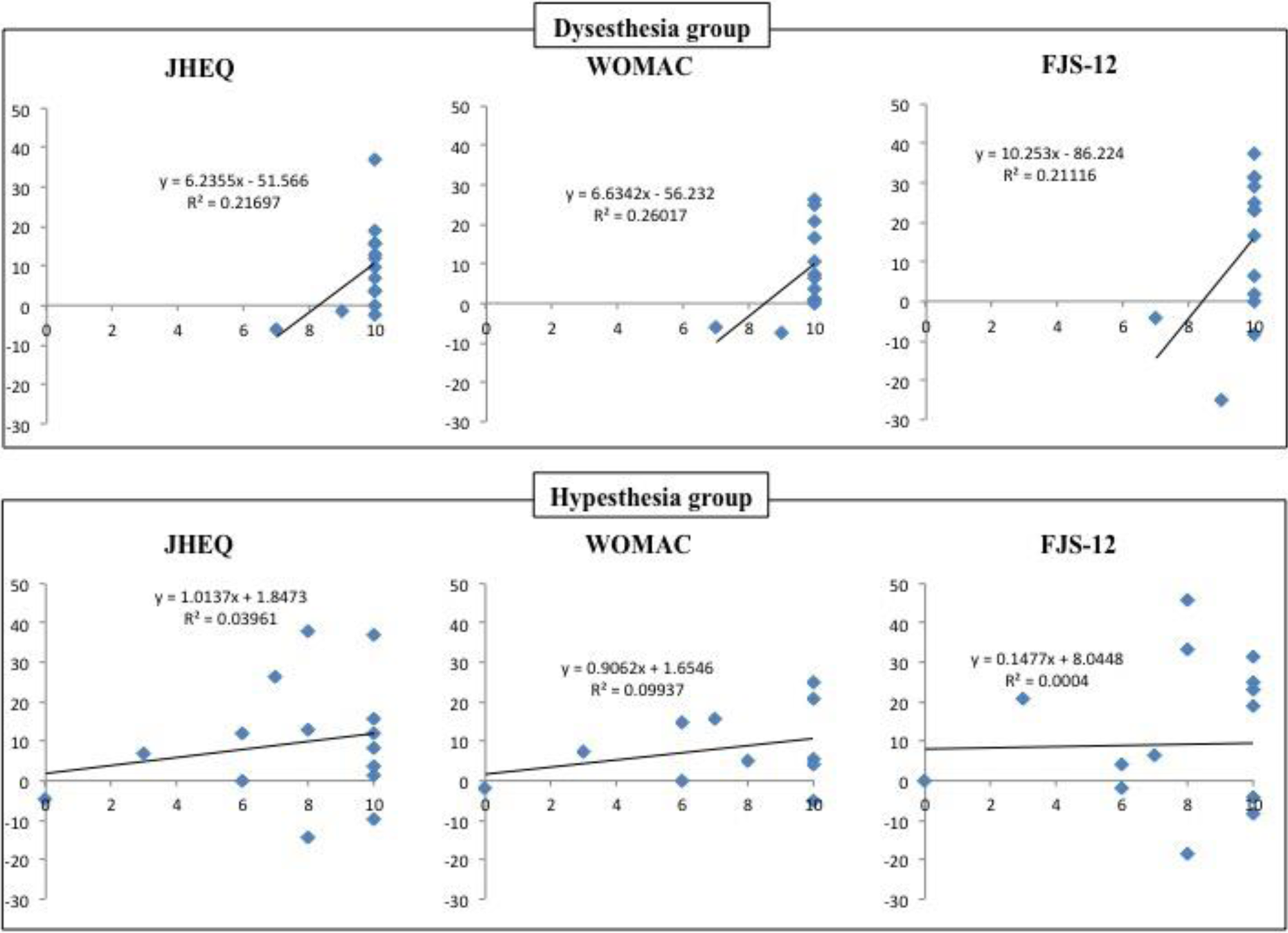
Relation between the changes of each PRO from the initial to the present survey (vertical axis) and changes of the symptoms between two surveys interval using visual analog scale (horizontal axis), in which 10 indicates that the symptoms are gone completely and 0 indicates that the symptoms are not changed at all. Dysesthesia group showed a significant correlation with each PRO. PROs: patient-reported outcomes; JHEQ: Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index; FJS-12: Forgotten Joint Score-12.
Discussion
Although DAA is gaining popularity, the risk of LFCN injury is a major drawback to this approach. However, little is known about this specific complication of DAA. The present study revealed that most of the symptoms of LFCN injury diminish over time and that the types of symptoms, hypesthesia versus dysesthesia, manifest different clinical courses.
We believe that LFCN injury can be temporary and recover spontaneously. Although it affects QOL during the early postoperative period, this complication does not outweigh the advantages of DAA. At the mean follow-up period of 26.2 months in the present study, the PROs of patients with LFCN injury were comparable to those of patients without LFCN injury, correlating with the resolution of symptoms. This suggests that LFCN injury should be evaluated over a sufficiently long follow-up period. Factors such as subjective versus objective evaluation have led to a wide variation in the reported incidence of LFCN injury 2,5,6,10 ; however, the length of the follow-up period is important when interpreting these results. For example, Goulding et al. found the incidence of LFCN injury in 55 patients after THA via DAA, to be 67%, but the mean follow-up duration was 13.4 months. 2 Our initial study (mean follow-up of 12.8 months) also showed a high incidence (31%). In contrast, Bhargava et al. reported that only 2 of 81 hips (2.47%) had paresthesias at final (2-year) follow-up, 10 even though different evaluation methods made comparison of the two studies difficult.
We believe that the symptoms of LFCN injury resolve spontaneously. We observed a significant decrease in the symptoms of LFCN injury during the interval between the two assessments (12.8 months and 26.2 months). Bhargava et al. also reported that 10 of 12 hips (83.3%) had full resolution of symptoms between 6-week and 2-year follow-ups. 10 Goulding et al. showed that only 3 of 53 patients (5.7%) reported complete resolution of symptoms 2 ; however, the follow-up periods were relatively short and the interval between the two time points (5.3 months and 12.3 months) appears insufficient.
The present study revealed that the type of LFCN injury influences QOL; the process of recovery from LFCN injury, and associated changes in QOL, differed significantly between the hypesthesia and dysesthesia groups. Although the type and severity of the symptoms vary, we established two groups on the basis of different sense modalities. Hypesthesia is a negative symptom; negative symptoms include deficits of different somatosensory qualities. Nickel et al. described these symptoms as uncomfortable but not painful. 17 Although patients may notice the symptom under certain circumstances, it usually does not cause too much concern. In other words, it is difficult for patients with hypesthesia to perceive that healing has occurred even if the symptom is improved. Therefore, PROs in the hypesthesia group might not correlate significantly with the rate of improvement.
Dysesthesia, in contrast, is a positive symptom. Abnormal ectopic excitability of afferent neurons leads to positive symptoms. Dysesthesia is caused by spontaneous discharge of neural fibers. 17,18 It occurs spontaneously and could be felt constantly, but is sometimes paroxysmal. Because the symptom is unremitting and aggravated by activity, as much as the degree of neurapraxia is severe, which correlated directly with QOL. This may explain why improvement of symptoms in the dysesthesia group, but not the hypesthesia group, was significantly correlated with PROs. This mechanism may also explain why there was significantly greater symptom improvement in the dysesthesia group than in the hypesthesia group. In the future, a prospective comparative study should be performed to investigate whether the presence of dysesthesia is associated with postoperative QOL.
Our finding of different clinical courses between the dysesthesia and hypesthesia groups suggests a mechanism of the incidence of the LFCN injury. It has been suggested that LFCN injury might be the result of various mechanisms, such as laceration, stretching, compression, and involvement in scar tissue formation. 2,11 We believe the most frequent mechanism to be stretching from retraction during the procedure; it is difficult to imagine spontaneous regeneration of a direct laceration of the LFCN with subsequent complete resolution of symptoms. The classic understanding of complete injuries of the peripheral nerves is that there is little chance of recovery. 19,20 Stretching of the LFCN would occur at the time of retraction of the intermuscular space between the TFL and sartorius muscles, where the LFCN is located or a branch of the LFCN crosses the TFL muscle. The stretching of the LFCN is more likely to cause temporary injury because the continuity of the nerve is maintained, which can lead to spontaneous resolution of symptoms. Therefore, we believe that avoiding excessive force and unnecessary retraction may help to prevent LFCN injury from occurring intraoperatively.
In contrast, LFCN laceration would occur at the time of incision of the skin and subcutaneous tissue and can lead to complete injury or irreversible damage. Further analysis of preoperative identification of the LFCN must be addressed in the future.
The present study has several limitations. First, clinician-reported outcomes were not assessed. It is possible that recovery of hip function over time brings about improvement in PROs. However, we think that there is no difference in the recovery process of hip function between the patients with LFCN injury and those without, because some studies showed that LFCN injury will not affect hip function. 10,12 Second, the diagnosis of LFCN injury at both the first and second assessments was determined by the subjective symptom assessment by questionnaires, which relies on patients’ recollection of the progress or degree of the symptoms. Objective evaluation by specific measurement such as two-point discrimination is more accurate and important. It enables to identify the clinical symptom as neuropathic symptom. 2,21 However, it is a possibility that uncomfortable symptom for the patient is underestimated in some cases. 2,21 Consequently, the incidence of LFCN injury may be underreported. 2,21 Therefore, we believed that the evaluation of subjective symptoms is very useful and important. 12 Third, the sample size of the present study was smaller than that of the initial study. Assessments took place within the same follow-up interval to increase validity and demonstrate the natural history of LFCN injury. Therefore, patients who did not respond within the scheduled period were excluded. And a collection bias was minimum, because the incidence rate of the LFCN injury at the initial survey in those excluded patients was similar to those in total patients in the initial survey.
Conclusion
Most symptoms of LFCN injury after THA via DAA resolved spontaneously with longer follow-up periods. In particular, improvement of dysesthesia as a symptom of LFCN injury was associated with better QOL.
Footnotes
Acknowledgment
The authors thank Dr. Mikio Matsumoto and Dr. Hironori Ochi for assisting the operation and collecting the data.
Author contribution
YH, TB, and KK designed the study. YO and KS obtained and analyzed the data. YH wrote the initial draft. AD ensured the accuracy of the data and analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.