
Abstract
Background: It is unclear what influence patient sex and body mass index (BMI) have on perioperative outcomes following total hip arthroplasty (THA), especially regarding anterior versus posterolateral approaches. Purpose/Study Questions: We sought to compare perioperative outcomes of primary THA via direct anterior (DAA) versus posterolateral (PLA) approaches, stratified by patient sex and BMI. Methods: A retrospective review at a single institution identified 8258 patients 18 to 80 years old who underwent primary THA via DAA or PLA for osteoarthritis between February 2019 and April 2022. Patients were stratified by sex and BMI (<30 or 30–40). We compared operative times, lengths of stay (LOS), opioid consumption and prescribing patterns, and achievement of Hip Injury and Osteoarthritis Outcome Score for Joint Replacement (HOOS JR) minimum clinically important difference (MCID), substantial clinical benefit (SCB), and patient acceptable symptom state (PASS) across the cohorts. Results: Median operative time was 6 to 11 minutes longer for DAA than for PLA. Median LOS was shorter for DAA, with the largest difference observed in women with BMI <30 (19-hour difference) and BMI 30 to 40 (20-hour difference). In-hospital milligram morphine equivalents consumed were lower for DAA in men with BMI <30 (45 vs 53), women with BMI <30 (45 vs 53), and women with BMI 30–40 (60 vs 75). There was no difference observed in HOOS JR MCID, SCB, or PASS achievement scores at 1 year for any cohort. Conclusion: This retrospective study found longer operative times for DAA than PLA and shorter LOS in women undergoing DAA than those undergoing PLA. There were minimal clinical differences in in-hospital opioid consumption, 90-day opioid prescription patterns, and patient-reported outcome measures. These findings suggest that patient sex and BMI may have implications on case scheduling and discharge planning for primary THA. Further study is warranted.
Keywords
Introduction
Total hip arthroplasty (THA) is a successful operation for osteoarthritis that is increasing in volume [22,28,37]. Current estimates predict over 1.4 million THAs performed annually in the United States by 2040 [37]. As THA volume increases, surgeons seek not only to improve patient outcomes but also to increase efficiency to manage THA volume effectively. Most commonly, THA is performed via posterolateral (PLA) or direct anterior (DAA) approaches, with DAA increasing in popularity [2]. A 2022 American Association of Hip and Knee Surgeons (AAHKS) annual meeting poll found DAA to exceed PLA in its percent utilization for primary THA [1–3,7]. As such, differences in perioperative outcomes between DAA and PLA are important considerations when attempting to increase operating room, hospitalization, and patient discharge efficiency and improve patient outcomes postoperatively.
Prior studies have consistently shown that DAA has a longer operative time than PLA, with an increased mean difference ranging from 5 to 20 minutes [4,29,38,40,41]. However, the effect that sex and body mass index (BMI) might have on operative time and lengths of stay (LOS), as well as other perioperative measures, for patients undergoing primary THA via DAA versus PLA are not well understood [32].
Thus, the objective of this study was to compare operative time and LOS of patients undergoing primary THA via DAA and PLA when stratified by patient sex and BMI. Secondarily, we sought to compare in-hospital opioid consumption, 90-day opioid prescribing patterns, and differences in short-term patient-reported outcome measures (PROMs), including the achievement of Hip Injury and Osteoarthritis Outcome Score for Joint Replacement (HOOS JR) minimum clinically important difference (MCID), substantial clinical benefit (SCB), and patient acceptable symptom state (PASS) at 1 year postoperatively.
Methods
After receiving approval from the Institutional Review Board at Hospital for Special Surgery, we retrospectively reviewed a single institutional database to identify all patients aged 18 to 80 years undergoing primary THA for osteoarthritis from February 1, 2019, to April 29, 2022, allowing for 1-year minimum potential follow-up. Patients were excluded if they had a BMI >40, underwent simultaneous bilateral THA, received an approach other than DAA or PLA, underwent THA for a diagnosis other than primary osteoarthritis (eg, conversion THA, post-traumatic arthritis, or inflammatory arthritis) or were discharged to a rehabilitation facility. Patients with a BMI >40 were excluded due to the relatively small number of DAA patients with a BMI >40 that would have met the other study inclusion criteria (n = 25). Patients discharged to rehabilitation centers were excluded because opioid prescriptions from rehabilitation centers could not be collected from the electronic medical record. Patients were excluded if they did not have 90-day follow-up, had another orthopedic procedure within 90 days preceding or following THA, or were taking opioids or benzodiazepines preoperatively.
A total of 8258 patients met inclusion criteria (Tables 1–4). The mean age for females with BMI <30 was 66 years (standard deviation [SD] = 11), females with BMI 30–40 was 64 years (SD = 10), males with BMI <30 was 65 years (SD = 10), and males with BMI 30–40 was 62 years (SD = 10). Females with BMI <30 who underwent DAA had a lower mean age (65 vs 66, P < .001), and males with BMI <30 who underwent DAA had a higher mean age (66 vs 65, P = .010). Females with BMI <30 who were part of the DAA group were slightly healthier than the PLA cohort and statistically significant differences in American Society of Anesthesiologists (ASA) risk level (P < .001) and Charlson Comorbidity Index (CCI) (P < .001). All cohorts had minor differences in at least 1 preoperative PROM.
Patient demographics and characteristics for females with body mass index < 30.
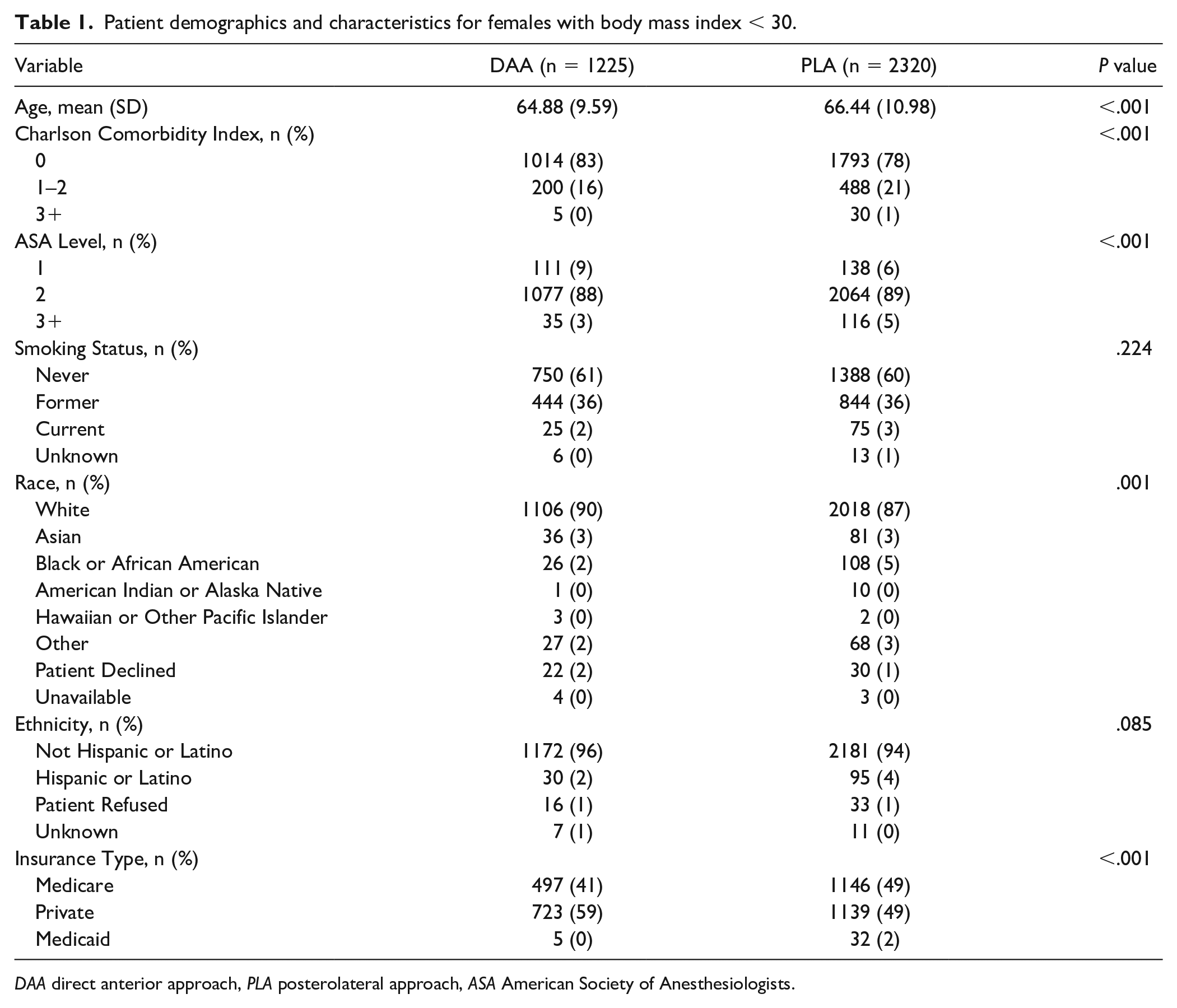
DAA direct anterior approach, PLA posterolateral approach, ASA American Society of Anesthesiologists.
Patient demographics and characteristics for females with body mass index 30–40.
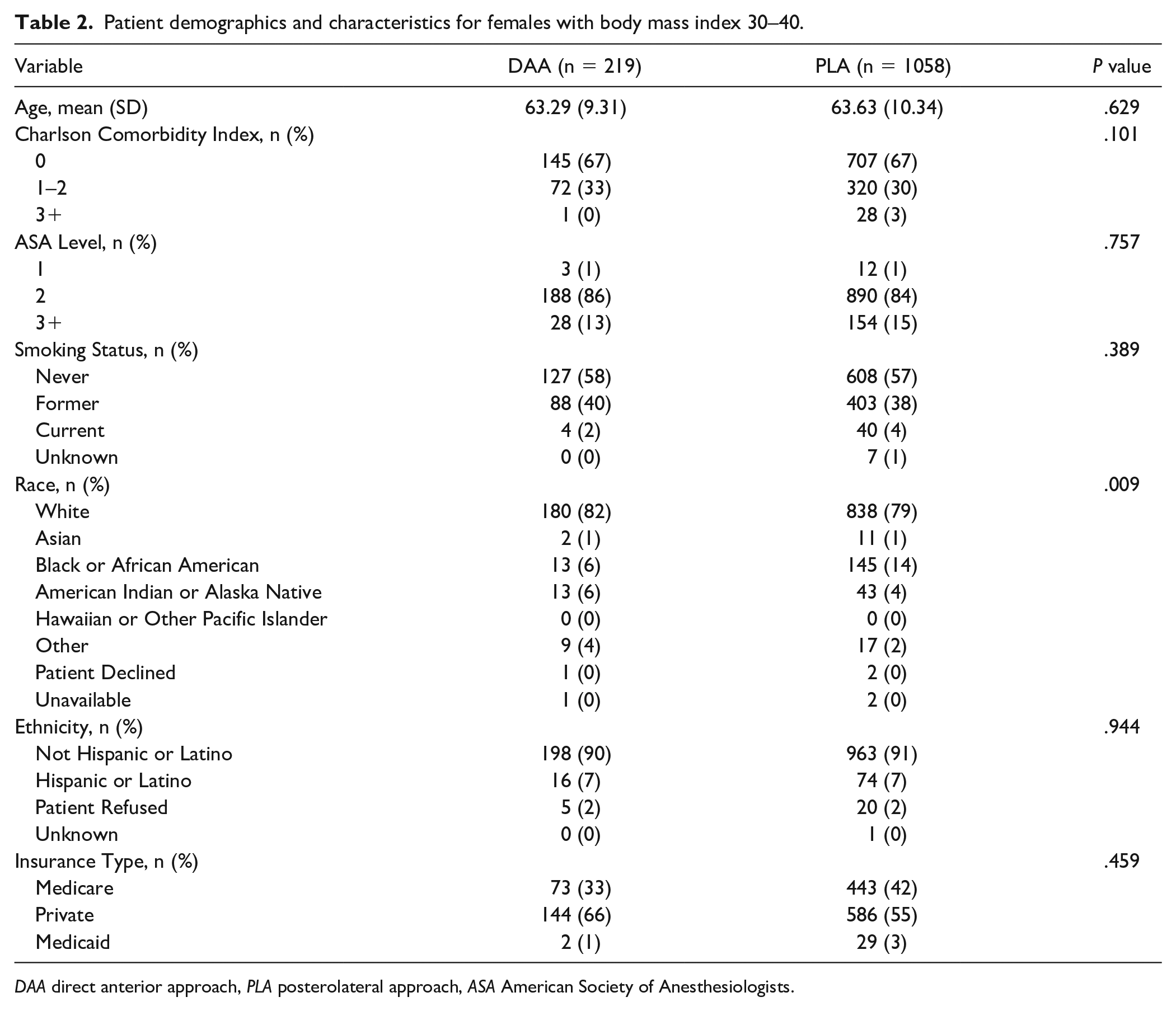
DAA direct anterior approach, PLA posterolateral approach, ASA American Society of Anesthesiologists.
Patient demographics and characteristics for males with body mass index < 30.
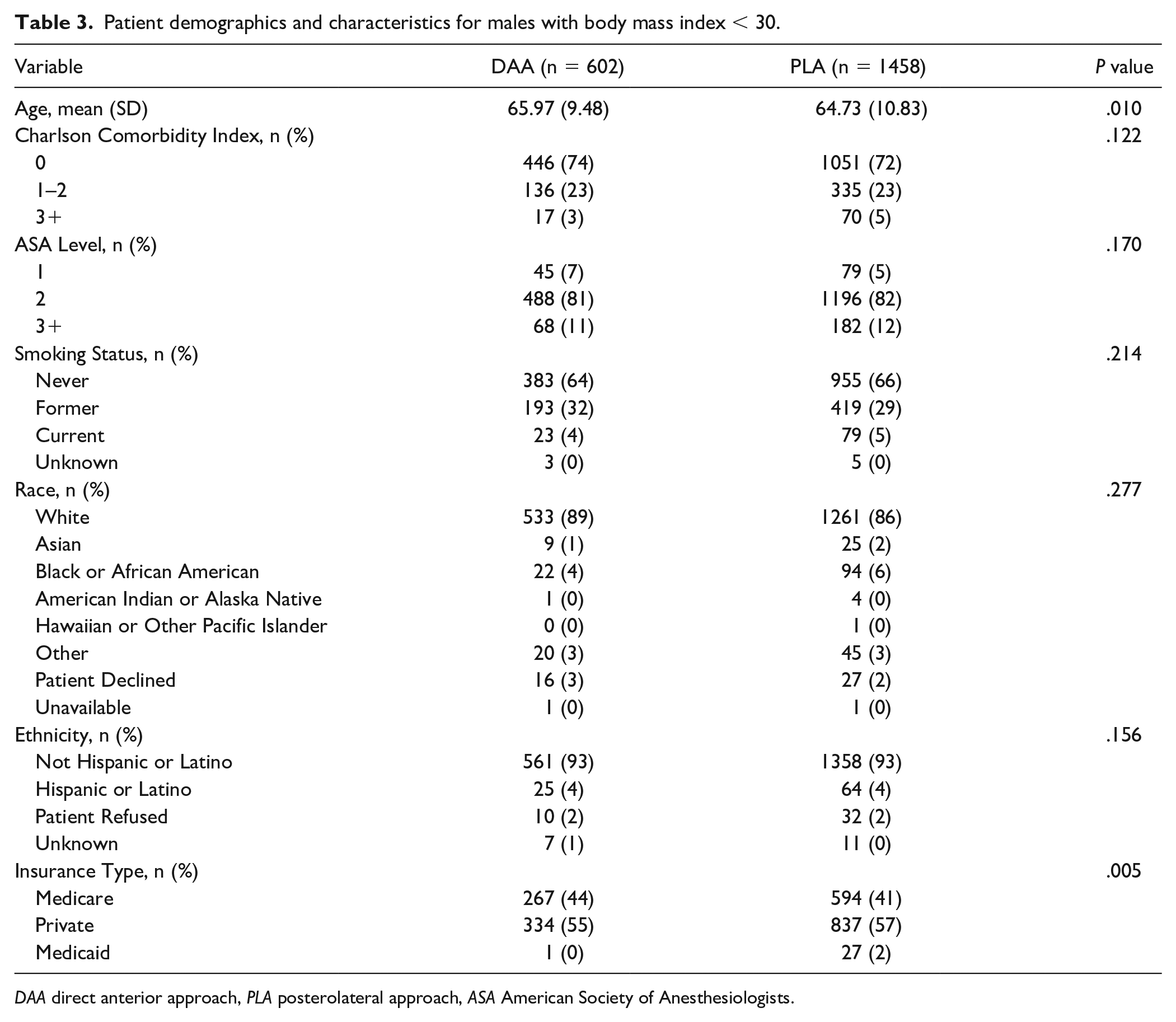
DAA direct anterior approach, PLA posterolateral approach, ASA American Society of Anesthesiologists.
Patient demographics and characteristics for males with body mass index 30–40.
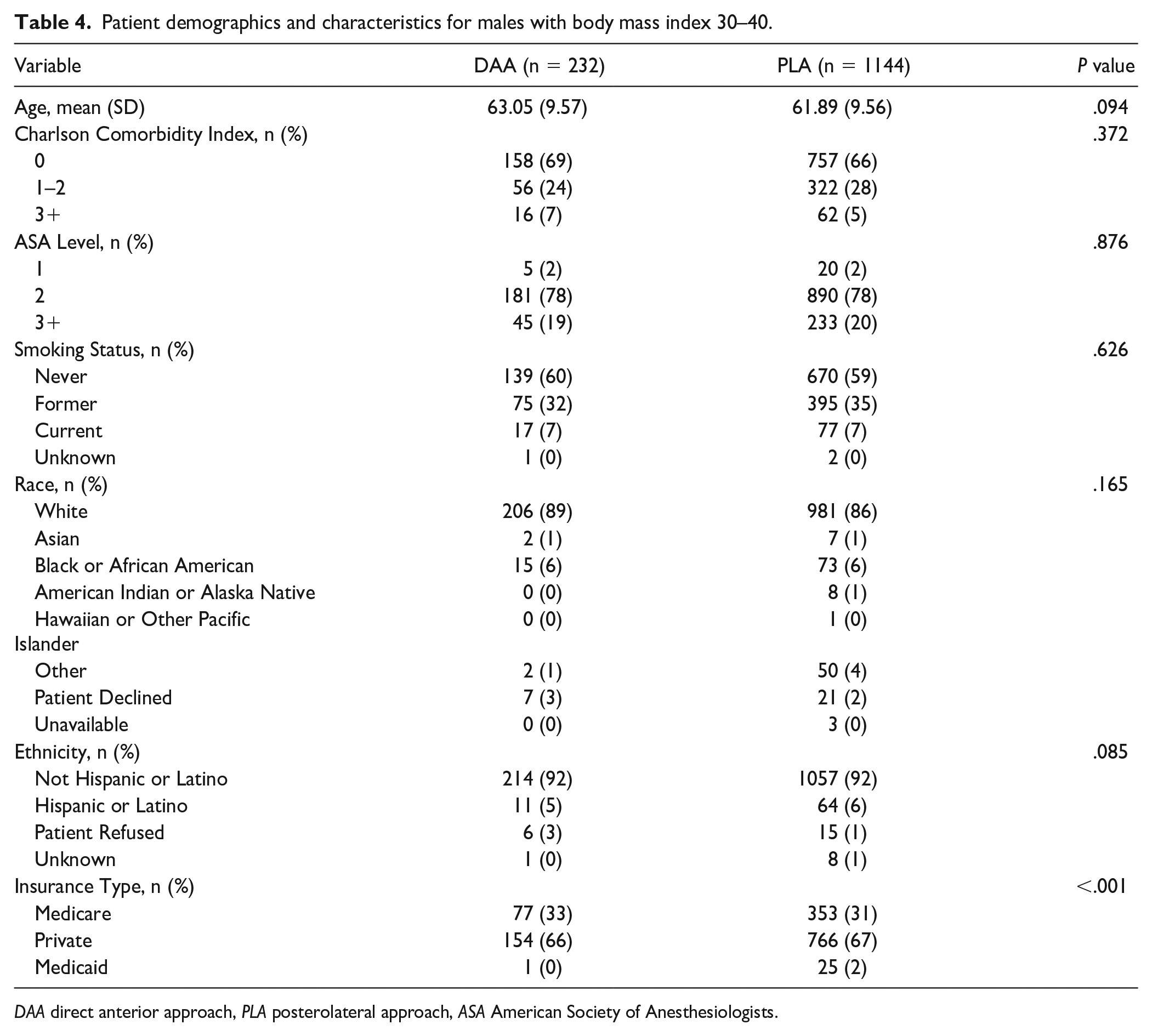
DAA direct anterior approach, PLA posterolateral approach, ASA American Society of Anesthesiologists.
The medical record was queried for relevant variables including patient demographics, preoperative diagnosis, and operative details. Patients were evaluated on the basis of sex and further divided into four cohorts: females with BMI <30 kg/m2, females with BMI 30 to 40 kg/m2, males with BMI <30 kg/m2, and males with BMI 30 to 40 kg/m2. Going forward, BMI units will be excluded for simplicity. Patients were divided by surgical approach and the following outcomes were compared: operative time, LOS, in-hospital opioid consumption, 90-day opioid prescription patterns, and PROMs.
Operative time was calculated as procedure start time to end time. The LOS was defined as the time from post-anesthesia care unit (PACU) admission to hospital discharge measured in hours. Ninety-day opioid prescription patterns were calculated based on inpatient opioid administration in milligram morphine equivalents (MMEs), in addition to opioid medications prescribed at the time of discharge and refills within 90 days. We also separately calculated intraoperative MME, postoperative inpatient MME, total in-hospital MME (intraoperative and postoperative inpatient), average hourly postoperative inpatient MME, and average hourly total in-hospital MME.
The PROMs evaluated included the HOOS JR, Patient-Reported Outcomes Measurement Information System (PROMIS) 10 Mental and Physical Component Scores, Veterans Rand 12 Mental and Physical score, and the Lower Extremity Activity Scale. For HOOS JR, the proportion of patients achieving the minimum clinically important difference (MCID), substantial clinical benefit (SCB), and patient acceptable symptom state (PASS) were compared between preoperative and 1-year postoperative time points [9,19]. Values previously determined through anchor-based methods were used including a HOOS JR MCID (18), SCB (22), and PASS (76.7) [18,25].
Statistical Analysis
Descriptive statistics were reported with mean and SD or median and interquartile range [IQR] based on the normality of the data. Categorical variables were reported with counts and proportions. The DAA and PLA cohorts were compared in terms of demographic variables using t-tests for continuous variables and Pearson χ2 or Fisher exact test for categorical variables. The Wilcoxon rank sum test was used to determine if there was evidence of a difference in the distributions of opioid use between DAA and PLA. The difference in medians of opioid consumption between cohorts was described using nonparametric bootstrapping using 1000 resamples. Linear regression using demographic covariates was performed for operative time, LOS, and opioid consumption/prescribing patterns to account for baseline differences in each cohort. T-tests were used to investigate if there were significant differences between the means of PROMs between DAA and PLA. Differences in achievement of HOOS JR MCID, SCB, and PASS were compared using the Pearson χ2 test. Significance was set at α = .05. All data analyses were conducted using R: A Language and Environment for Statistical Computing (R Core Team, Vienna, Austria) version 4.1.0 (2021-05-18).
Results
When evaluating patient sex overall regardless of approach (Supplemental Tables 1–3), females had a longer median LOS than males (33 vs 27 hours, P < .001). Female patients also demonstrated higher total postoperative inpatient MME (45 vs 38, P = .002). In contrast, total 90-day MMEs were significantly lower in female patients (255 vs 270, P < .001). We found no difference in achievement of MCID, SCB, and PASS at 1-year for HOOS JR between males and females.
When further stratifying by approach, median operative time was longer for DAA in all 4 cohorts by 6 to 11 minutes (Supplemental Table 4). The difference in operative time (DAA–PLA) included females with BMI <30 (9 minutes, P < .001), females with BMI 30–40 (6 minutes, P = .032), males with BMI <30 (11 minutes, P < .001), and males with BMI 30–40 (10 minutes, P < .001). Regression analysis revealed no clinically significant influence of age, ASA, CCI, or insurance type on operative time (Supplemental Table 5).
Median LOS was significantly shorter for DAA in all cohorts, by 2 to 4 hours in the male cohorts and 19 to 20 hours in the female cohorts (Supplemental Table 6). The difference in LOS (PLA–DAA) included females with BMI <30 (19 hours, P < .001), females with BMI 30–40 (20 hours, P < .001), males with BMI <30 (4 hours, P < .001), and males with BMI 30–40 (2 hours, P < .001). All 4 cohorts had significantly longer median LOS with the PLA approach, but in females (both BMI <30 and 30–40) this difference was more pronounced with median LOS with DAA of 26 to 27 hours, and median LOS with PLA of 45 to 47 hours. Regression analysis revealed ASA levels 2 and 3+ to be associated with longer LOS by 3 hours (95% CI: 1–6, P = .020) and 12 hours (95% CI: 9–15, P < .0001), respectively. Regression analysis revealed CCI 1–2 and 3+ to be associated with longer LOS by 4 hours (95% CI: 2–5, P < .0001) and 22 hours (95% CI: 19–25, P < .0001), respectively. Finally, regression analysis revealed Medicare insurance to be associated with a shorter LOS by 15 hours (95% CI: 20–10) when compared with private insurance (P < .0001).
Median postoperative inpatient MMEs consumed was lower for DAA in all cohorts by 8 to 17 MMEs (Table 5). The difference in median postoperative inpatient MMEs (PLA–DAA) included females with BMI <30 (15 MMEs, P < .001), females with BMI 30–40 (17 MMEs, P < .001), males with BMI <30 (8 MMEs, P < .001), and males with BMI 30–40 (8 MMEs, P = .010). The DAA had a higher hourly median total postoperative inpatient MME in all cohorts but was only significant for females with BMI <30 (1.3 vs 1.15 MME/hour, P = .001) and males with BMI 30–40 (2.0 vs 1.8 MME/hour, P = .044). Regression analysis revealed ASA levels 2 and 3+ to be associated with greater median total postoperative inpatient MMEs consumed by 11 MMEs (95% CI: 5–19, P = .001) and 17 MMEs (95% CI: 9–25, P < .0001), respectively (Supplemental Table 7). Regression analysis revealed CCI 1–2 and 3+ to be associated with greater median total postoperative inpatient MMEs consumed by 10 MMEs (95% CI: 6–13, P < .0001) and 23 MMEs (95% CI: 14–32, P < .0001), respectively. Finally, regression analysis found Medicare insurance to be associated with lower median total postoperative inpatient MMEs consumed compared with private insurance (34 MMEs, 95% CI: 45 to 22, P < .0001).
Primary total hip arthroplasty in-hospital opioid consumption and 90-day prescribing patterns stratified by patient cohort.
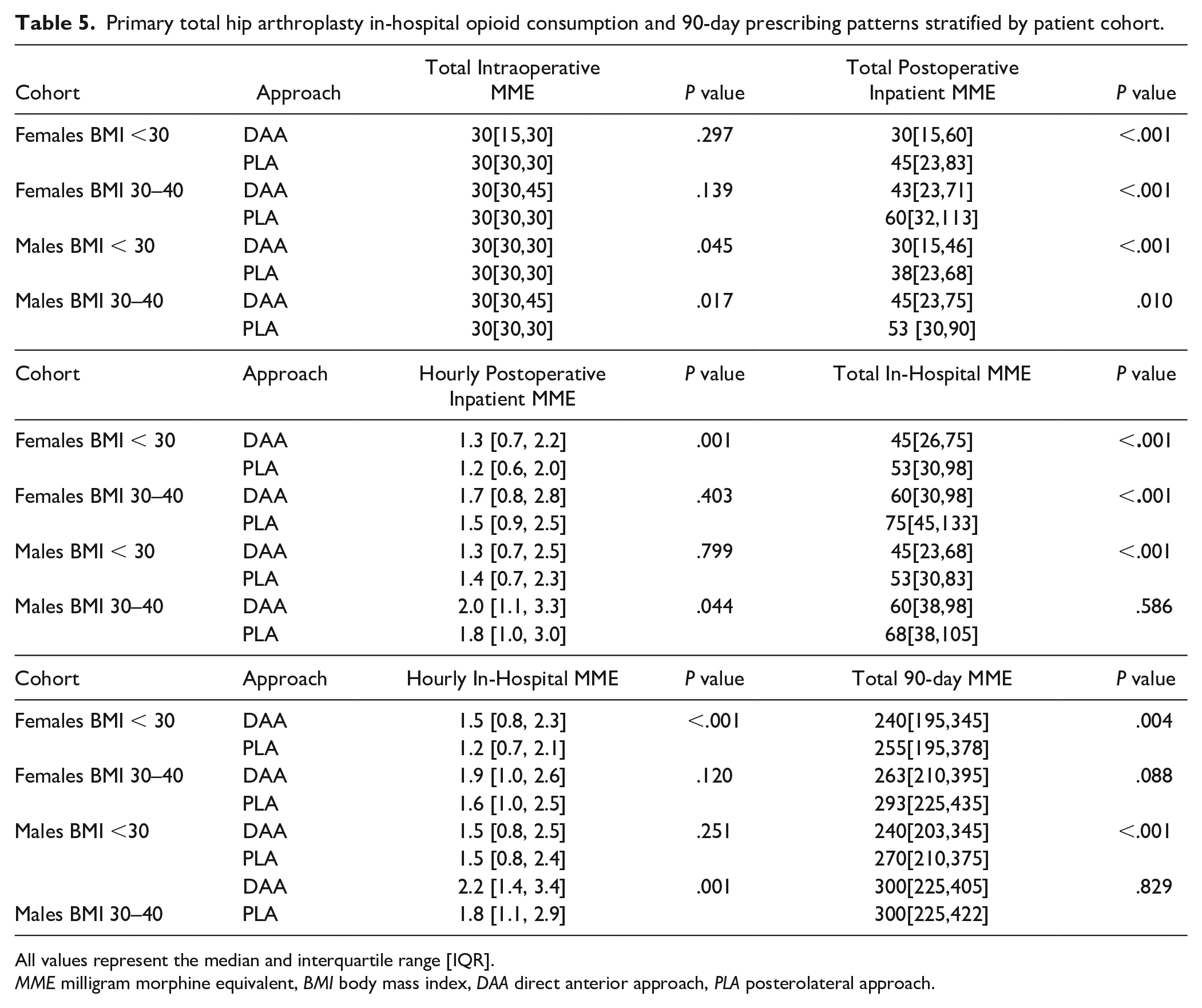
All values represent the median and interquartile range [IQR].
MME milligram morphine equivalent, BMI body mass index, DAA direct anterior approach, PLA posterolateral approach.
Regarding differences in median total 90-day MME prescribed, statistically significant differences existed for two cohorts, with lower MMEs prescribed for DAA in men with BMI <30 (240 vs 270, P < .001) and females with BMI <30 (240 vs 255, P = .004). Regression analysis revealed no clinically significant influence of age, ASA, CCI, or insurance type on the median total 90-day MME prescribed.
There were no significant differences between DAA and PLA in the proportion of patients achieving HOOS JR MCID, SCB, or PASS (Supplemental Tables 8–10) for any cohort at 1 year postoperatively (P > .124). The percentage of patients achieving MCID ranged from 80% to 86%, the percentage of patients achieving SCB ranged from 70% to 85%, and the percentage of patients achieving PASS ranged from 81% to 90%.
Discussion
With an increasing volume of THA, surgeons have an important responsibility to improve patient outcomes and perioperative efficiency [22,28,37]. National selection trends have shown that healthier patients tend to undergo DAA, but as surgeons gain experience with DAA, their technical skills will allow them to use this approach with a wider patient population [13,30,39]. There is little evidence on the effect patient demographics have on perioperative outcomes following primary THA [32]. The objective of this study was to compare perioperative outcomes after primary THA via DAA versus PLA when stratified by patient sex and BMI. In this large series of primary THA patients, we found longer operative times for DAA but shorter LOS. However, the shorter LOS was especially pronounced among female patients with a median difference of 19 to 20 hours compared with PLA, whereas in male patients the difference in LOS was only 2 to 4 hours. These findings emphasize that the difference in median LOS between the 2 approaches is most clinically relevant in females. We also observed a significant difference with higher postoperative inpatient opioid usage in the PLA approach groups for both female cohorts, and in the male cohort with BMI <30. Otherwise, there were no clinically significant differences in in-hospital opioid consumption, 90-day opioid prescribing patterns, or achievement of HOOS JR MCID, SCB, or PASS at 1 year.
The present study is not without potential limitations. Given its retrospective nature, it is susceptible to bias, including the fact that DAA is marketed as a less invasive surgery and consequently patients may be more inclined to be discharged the day of surgery. Our cohorts had several differences in baseline demographics that may have influenced our results. Regression analysis helped to elucidate the potential impact of each covariate. In addition, due to small sample sizes, we did not evaluate those patients with a BMI >40 but recognize the importance of further study on the implications that increasing BMI has on primary THA outcomes. Regarding operative time, there were multiple surgeons, and surgical technique was not standardized, but this does increase the generalizability of the study results. We did not account for the presence of a trainee as first assistant or the possibility that surgeons may have been within their learning curve for DAA, which is associated with increased operative time [23]. We did not consider the use of computer or robotic navigation, which has learning curves of their own [16,31] and could have influenced the operative time [17]. For opioid prescription pattern variables, we relied on the electronic medical record, and thus, it is possible that not all prescriptions were captured. All patients discharged to acute rehabilitation facilities were excluded for this reason. Furthermore, utilizing prescriptions after discharge instead of MME consumed does not account for the actual opioid consumed by the patient.
Operative time was significantly longer for DAA in all cohorts. The difference in median operative time ranged from 6 minutes in females with BMI 30–40 (P = .032) to 11 minutes in males with BMI <30 (P < .001). Unsurprisingly, we also found that patients in the larger BMI cohorts, both male and female, had longer operative time irrespective of approach. Our results were similar to previous literature reporting, as we found increased operative time for DAA. Peng et al [29] in their meta-analysis of 6 randomized controlled trials (RCTs), found DAA to have a significantly longer surgical duration than PLA by 13.74 minutes [6,10,24,34,42,43]. While the differences of 6 to 11 minutes found in the present study may be less than in other reports, this is still an important consideration for case scheduling. We did not separately evaluate case set-up, which may have resulted in larger median differences between approaches when accounting for special equipment commonly utilized during DAA (e.g., fracture tables and intraoperative fluoroscopy).
The LOS was significantly shorter for DAA in all patient cohorts (P < .001). Males with BMI <30 and 30–40 saw small differences in median LOS of 4 and 2 hours, respectively, which are unlikely to be clinically relevant. Females with BMI <30 and 30–40 had median differences of 19 and 20 hours, respectively, despite these cohorts having a smaller proportion of patients with Medicare. Our regression analysis revealed Medicare to be associated with shorter LOS, which could be seen as a surrogate for socioeconomic status. Females with BMI <30 undergoing PLA did have a greater proportion of ASA 2 or 3+ and CCI 1–2 or 3+ which could have contributed to their increased LOS as reflected by our regression analysis, but these baseline differences were not seen in the females with BMI 30–40 cohort who also had a significantly shorter LOS after DAA. This may help explain why females undergoing PLA, as a group, had an overall longer LOS. Inherent bias in discharge planning may have also played a role, and DAA is marketed as a less invasive surgery potentially accelerating discharge in female patients. DAA patients may be more encouraged to be discharged the same day because of this. However, this would not explain the large difference in median LOS between women and men undergoing PLA. Nonetheless, these differences are clinically relevant and may be important during preoperative surgical planning. Future prospective research could further explore how sex, comorbidity burden, and surgical approach interact to influence discharge timing.
Conversely, Peng et al found no difference in LOS between DAA and PLA in their meta-analysis of 6 RCTs (mean difference [MD] -1.52 days, 95% CI: -3.75 to 0.71, P = .18) [6,10,11,30,34,42,43]. Others have shown DAA to have shorter LOS [14,27]. Miller et al [27] performed a meta-analysis of 5 RCTs and reported a shorter LOS for DAA by 0.5 days (P = .05). Higgins et al [14] in their meta-analyses of 7 prospective and retrospective comparative studies found a shorter LOS for DAA, WMD: -0.53 days (95% CI: -1.01 to -0.04). Sub-analysis of LOS after primary THA via DAA or PLA based on patient demographics has not been reported in the literature and it is difficult to make direct comparisons.
In our study, total in-hospital MME consumption was significantly lower when undergoing DAA for males with BMI <30 (45 vs 53, P < .001), females with BMI <30 (45 vs 53, P < .001), and females with BMI 30–40 (60 vs 75, P < .001). However, it is unlikely that these results are clinically significant. The DAA had higher hourly MME consumption, which is likely explained by a shorter LOS for DAA cohorts, with most MMEs administered earlier postoperatively. Previous work has established a 24-hour MME MCID of 10 MMEs [20]. We reported hourly in-hospital MME consumption and when multiplied by 24 hours, no cohort had a difference larger than 10 MMEs (Table 5). Similarly, the statistically lower total 90-day MME prescribed after DAA in females with BMI <30 (240 vs 255, P = .004) and males with BMI <30 (240 vs 270, P < .001) becomes clinically insignificant in the same context. While there is no longer-term MME MCID established, it is unlikely that differences of 15 and 30 MMEs over 90 days would reach its threshold.
The existing literature on opioid consumption after THA via DAA versus PLA is mixed. Bovonratwet et al [8] retrospectively reviewed 447 DAA and 164 PLA patients from a single surgeon and found no differences in total inpatient MMEs (79.8 vs 100.1, P = .486). They also found no difference in the proportion of patients receiving an opioid prescription refill within 90 days (14.77 vs 20.73%, P = .077). Contrary to this, Miller and colleagues’ meta-analysis reported on in-hospital MME requirements from 2 RCTs [6,10] evaluating primary THA via DAA versus PLA [27]. They found a standardized mean difference (SMD) of -0.39 (95% CI: -0.70 to -0.08, P = .014) in favor of DAA, corresponding to 12 fewer MMEs per day of hospitalization [27]. Seah et al [36] reported on 179 DAA, 203 PLA, and 178 direct lateral approach [DLA]) and found DAA oral morphine equivalent daily dose (oMEDD) to be 16.8 lower than DLA (P < .01) and 14.5 lower than PLA (P = .02).
The PROMs evaluated in this study revealed several statistically significant but clinically unimportant differences between preoperative and postoperative time points. In addition, there were no significant differences in the proportion of patients achieving HOOS JR MCID, SCB, or PASS at 1 year. There are reports in the literature of improved short-term PROMs after DAA, but in this study, we did not find clinically significant benefits [5,21,26,35]. Rhee et al [32] retrospectively evaluated PROMs in 312 DAA and 383 PLA cases, reporting on the effect that sex and BMI had on improvement in the Oxford Hip Score (OHS). The OHS has an MCID of 5 [12,15,30,33]. They reported that for women with BMI ≤22, there was a difference in mean OHS improvement of >5 points in favor of DAA, while women with BMI ≥46 saw a difference in mean OHS improvement of >5 points favoring PLA. For men, a >5-point mean difference in OHS was only seen for BMI >50, which favored PLA. Rhee et al did not report the absolute change in OHS scores from preoperative to postoperative time points or the proportion of each cohort achieving OHS MCID.
In conclusion, this retrospective review found that DAA had a longer overall operative time in all sex and BMI cohorts and that female patients with BMI <40 had a clinically significant reduction in LOS following primary THA via DAA. Evaluation of in-hospital opioid consumption, 90-day opioid prescribing patterns, and short-term PROMs revealed slight statistical differences favoring DAA but overall minimal clinical benefit for men or women with BMI <40 following primary THA. These findings suggest that surgical approach may have implications for case scheduling and staffing needs as well as patient sex and BMI for discharge planning during primary THA.
Supplemental Material
sj-docx-1-hss-10.1177_15563316251323612 – Supplemental material for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review
Supplemental material, sj-docx-1-hss-10.1177_15563316251323612 for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review by Colin C. Neitzke, Pravjit Bhatti, Sonia K. Chandi, Ranqing Lan, Elizabeth B. Gausden, Peter K. Sculco and Brian P. Chalmers in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316251323612 – Supplemental material for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review
Supplemental material, sj-docx-2-hss-10.1177_15563316251323612 for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review by Colin C. Neitzke, Pravjit Bhatti, Sonia K. Chandi, Ranqing Lan, Elizabeth B. Gausden, Peter K. Sculco and Brian P. Chalmers in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316251323612 – Supplemental material for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review
Supplemental material, sj-docx-3-hss-10.1177_15563316251323612 for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review by Colin C. Neitzke, Pravjit Bhatti, Sonia K. Chandi, Ranqing Lan, Elizabeth B. Gausden, Peter K. Sculco and Brian P. Chalmers in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316251323612 – Supplemental material for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review
Supplemental material, sj-docx-4-hss-10.1177_15563316251323612 for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review by Colin C. Neitzke, Pravjit Bhatti, Sonia K. Chandi, Ranqing Lan, Elizabeth B. Gausden, Peter K. Sculco and Brian P. Chalmers in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316251323612 – Supplemental material for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review
Supplemental material, sj-docx-5-hss-10.1177_15563316251323612 for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review by Colin C. Neitzke, Pravjit Bhatti, Sonia K. Chandi, Ranqing Lan, Elizabeth B. Gausden, Peter K. Sculco and Brian P. Chalmers in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316251323612 – Supplemental material for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review
Supplemental material, sj-docx-6-hss-10.1177_15563316251323612 for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review by Colin C. Neitzke, Pravjit Bhatti, Sonia K. Chandi, Ranqing Lan, Elizabeth B. Gausden, Peter K. Sculco and Brian P. Chalmers in HSS Journal®
Supplemental Material
sj-docx-7-hss-10.1177_15563316251323612 – Supplemental material for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review
Supplemental material, sj-docx-7-hss-10.1177_15563316251323612 for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review by Colin C. Neitzke, Pravjit Bhatti, Sonia K. Chandi, Ranqing Lan, Elizabeth B. Gausden, Peter K. Sculco and Brian P. Chalmers in HSS Journal®
Supplemental Material
sj-docx-8-hss-10.1177_15563316251323612 – Supplemental material for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review
Supplemental material, sj-docx-8-hss-10.1177_15563316251323612 for Stratified Comparison of Short-Term Perioperative Outcomes in Direct Anterior Versus Posterolateral Primary Total Hip Arthroplasty: A Retrospective Review by Colin C. Neitzke, Pravjit Bhatti, Sonia K. Chandi, Ranqing Lan, Elizabeth B. Gausden, Peter K. Sculco and Brian P. Chalmers in HSS Journal®
Footnotes
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Colin C. Neitzke: Osgenic Oy; Elizabeth B. Gausden: BICMD, Stryker, Zimmer, American Association of Hip and Knee Surgeons, International Orthopaedic Education Network; Peter K. Sculco: Enovis, Zimmer, Intellijoint Surgical, Parvizi Surgical Innovation; Brian P. Chalmers: HSS Journal, Journal of Arthroplasty, Orthodevelopment, Smith & Nephew. The other authors declared no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Informed Consent
Informed consent was waived from all patients included in this study, per the Institutional Review Board at Hospital for Special Surgery.
Level of Evidence
Level III: Retrospective Therapeutic Study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.