
Abstract
We evaluated the risks and success rates of the three major techniques for compartment syndrome fasciotomy closure by reviewing all literature published to date. Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, we systematically evaluated the Medline (PubMed) database until July 2015, utilizing the Boolean search sting “compartment syndrome OR fasciotomy closure.” Two authors independently assessed all studies published in the literature to ensure validity of extracted data. The data was compiled into an electronic spreadsheet, and the wound closure rate with each technique was assessed utilizing a proportion random model effect. Success was defined as all wounds that could be closed without skin grafting, amputation, or death. The highest success rate was observed for dynamic dermatotraction and gradual suture approximation, whereas vacuum-assisted closure had the lowest complication rate.
Introduction
Fasciotomy is the standard treatment for acute compartment syndrome (ACS). 1 Historically, fasciotomy incisions were either left open or immediately closed; however, the rates of infections and recurrent compartment syndrome were unacceptably high. 2 In an attempt to improve outcomes, there is a plethora of different wound closure techniques published, which includes immediate closure, delayed primary closure, and ultimately utilizing a skin graft to fill the void. 1,3 Immediate or delayed primary wound closure may help decrease the infection rates and improve the cosmetic outcomes when compared with secondary closure and skin grafts. 3 However, primary closure is not always possible, due to tissue edema. 4
Currently, there is no consensus regarding which technique should be used when closing fasciotomy incisions. 1 As a result, wound closure technique is based on the surgeon’s preference and the requirements of each clinical scenario. 5 Different techniques have diverse success rates, times to closure, and complication rates. 1,6,7 If an initial attempt of closure is unsuccessful, subsequent reoperation with another closure technique and/or grafting may be required. However, grafting itself is associated with significant morbidity, poor cosmetic results, and pain at the graft donation site. 8 Furthermore, regardless of which closure technique is used, it is always important to understand the complications associated with the underlying cause of compartment syndrome or the fasciotomy itself, such as infection, delayed bone healing, amputation, or even death. 7,8
Although multiple wound closure techniques are described in the orthopedic literature, there is limited data regarding the efficacy and safety of these techniques following a fasciotomy. In addition, due to the heterogeneity in the type and quality of studies, the relatively high complication rates, and the clinical burden, there is a need for a systematic review of the literature to assess the current evidence regarding fasciotomy closure techniques. The goals of this study are to (1) determine the current techniques available for fasciotomy wound closure; (2) assess the overall success of these techniques in achieving wound closure in the extremities; and (3) evaluate the effectiveness of these techniques in minimizing the time required for fasciotomy wound closure and complication rates.
Methods
We performed a systematic search of the literature using the Medline (PubMed) library to identify all studies that have evaluated fasciotomy wound closure. This was performed following utilizing the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 9 Two authors independently assessed all studies published in the literature until July 2015 using the following search strings: “compartment syndrome OR fasciotomy closure,” which returned a total of 8577 abstracts.
These studies were carefully evaluated to determine those that were relevant. The following inclusion criteria were utilized: (1) full-text reports; (2) randomized controlled trials (RCTs), cohort studies, case–control studies, and case series with two or more patients; (3) studies involving patients with ACS of the extremities treated with fasciotomy; (4) studies describing the method of fasciotomy closure; and (5) studies that reported time to closure as an outcome measure. Studies published in languages other than English, single case reports, articles regarding exercise-induced compartment syndrome, and articles whose outcome measures did not include time to closure for each closure technique were excluded.
A total of 90 potential studies were determined to be potentially relevant. These were cross-referenced to identify an additional 17 potential studies. These 107 studies were carefully evaluated and 52 met inclusion criteria. Of these 52 studies, 29 were excluded due to the following reasons: 3 studies did not stratify the time to wound closure according to the technique used 10 –12 ; 2 studies did not separate wound closure following fasciotomy from wound closure following other procedures 13,14 ; 2 studies explored only static tension techniques (Steri-Strips) 3,15 ; and 22 studies examined only split thickness skin graft (STSG) and/or conservative treatment. 2,4,8,16 –34 Figure 1 displays a summary of the research methodology. The 23 remaining studies were included in the final analysis and are described in Tables 1–6.

Search methodology flowchart.
Studies evaluating gradual suture approximation, demographics, and success rate.
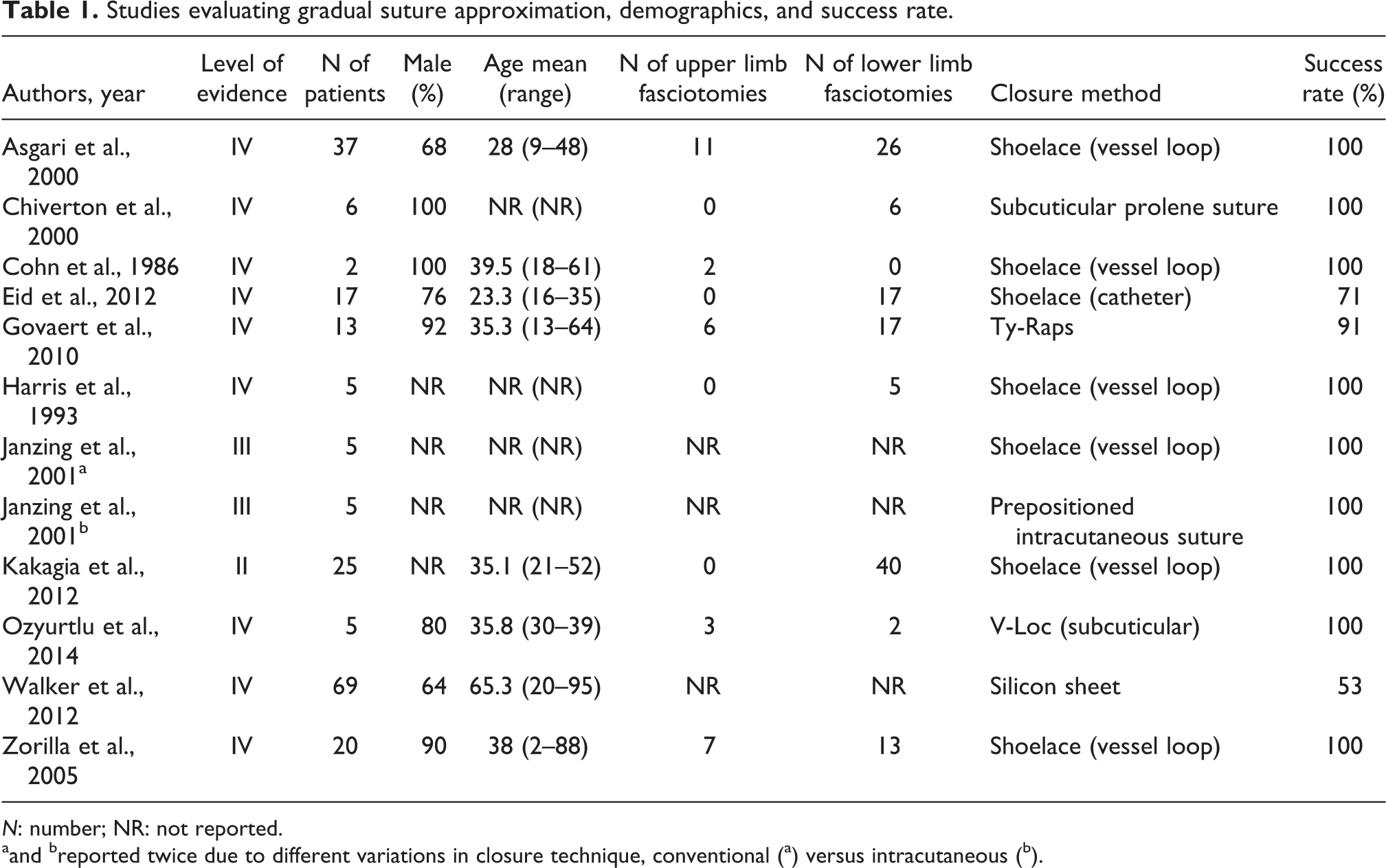
N: number; NR: not reported.
aand breported twice due to different variations in closure technique, conventional (a) versus intracutaneous (b).
Studies evaluating dynamic dermatotraction, demographics, and success rate.

N: number; NR: not reported.
Studies evaluating vacuum-assisted closure, demographics, and success rate.

N: number; NR: not reported.
Studies evaluating gradual suture approximation, complications.

N: number; NR: not reported.
aand breported twice due to different variations in closure technique, conventional (a) versus intracutaneous (b).
Studies evaluating dynamic dermatotraction, complications.

N: number.
Studies evaluating vacuum-assisted closure, complications.

N: number.
The data for the studies were compiled into an electronic spreadsheet (Microsoft Excel, Microsoft Office, Redmond, Washington, USA). Statistical analysis was performed using a statistical software (Med Calc, MedCalc Software bvba, Ostend, Belgium). We performed forest plots of the proportion of wounds that were successfully closed with each technique. Success was defined as all wounds that could be closed without skin grafting, amputation, or death.
This study was performed with no external funding.
Description of each technique
Conservative
Conservative treatment generally consists of wet-to-dry dressings, followed by delayed primary closure (DPC). Healing by secondary intention is employed if DPC is not possible. 3,35
Split-thickness skin graft
Historically, STSG was the only alternative if conservative treatment failed or was deemed impossible due to the size of the fasciotomy wound. 2,12 However, STSG is associated with significant morbidity, including risks associated with an additional surgery under general anesthesia, pain at the graft donor site, infection, lack of sensation in the grafted area, risk of graft nonadherence, and poor cosmetic outcomes. 1 Despite the significant risks associated with STSG, it is still frequently used when alternative methods fail.
Gradual suture approximation
Several variations of the “shoelace” technique have been used to gradually approximate the wound edges. 36 The technique, as initially proposed by Cohn et al., involves the placement of staples along the wound edges, followed by threading a vessel loop through the staples like a shoelace. 37 Several variations on this technique have been proposed, such as the use of nylon sutures 36,38 or subcuticular K-wires 39 instead of a vessel loop in the same shoelace pattern. Govaert and van Helden proposed a similar technique utilizing several Ty-Raps (Thomas & Betts, Memphis, Tennessee, USA), which are stapled to the skin and individually tightened each day. 40 Gradual suture approximation techniques generally have low costs, as they use inexpensive materials that are generally readily available.
Dynamic dermatotraction
Several different proprietary devices have been used to close fasciotomy wounds by applying continuous tension to the wound edges until they can be closed by DPC, which are classified as “dynamic dermatotraction devices” by Kakagia et al. 1 These devices are described in Table 7. One major drawback to these devices is the significant costs, which can be US$500–US$1000 per device. 41
Dynamic dermatotraction devices.

Vacuum-assisted closure
Vacuum-assisted closure (VAC; Kinetic Concepts, Inc., San Antonio, Texas, USA) therapy involves use of a foam dressing, covered by an adhesive drape, which is connected to a vacuum pump in order to create sub-atmospheric pressure on the wound, until the wound edges are approximated enough to permit DPC. 35 This process, known as negative pressure wound therapy (NPWT), removes excess fluid, thus reducing edema and ideally accelerating wound healing. 1 VAC therapy may also decrease bacterial count and stimulate angiogenesis. 50 The equipment required for VAC costs approximately US$96.51 per day. 51
Results
In total, we evaluated 23 studies with a total of 606 patients, ranging in age from 0.92 to 95 years, who underwent 118 upper compartment and 621 lower compartment fasciotomies. 1,5,35,37,38,40,41,43 –49,52 –60 Tables 1–3 display the demographic information of the included patients.
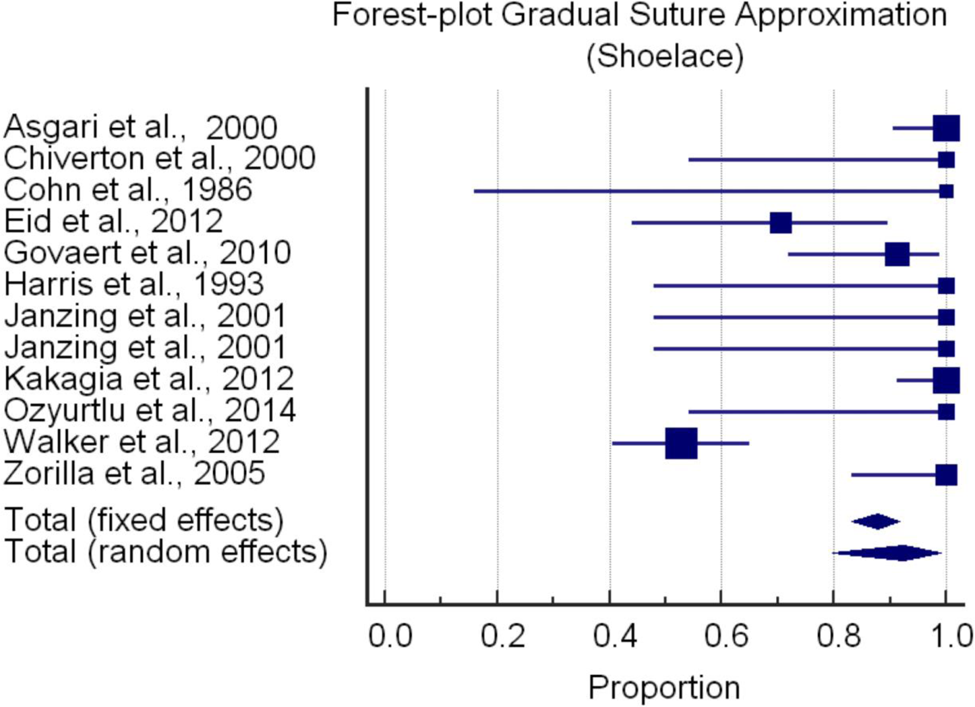
Dynamic dermatotraction had the highest success rate at 92.7% (95% confidence intervals (CI) of 85.1 to 97.7%), as shown in Figure 2. Gradual suture approximation followed with a success rate of 92.4% (95% CI of 79.8 to 99.1%), as shown in Figure 3. VAC had the lowest success rate of 78.1% (95% CI of 74.6 to 81.4%), as shown in Figure 4.
Proportion of patients who achieved closure with dynamic dermatotraction.

Proportion of patients who achieved closure with gradual suture approximation.
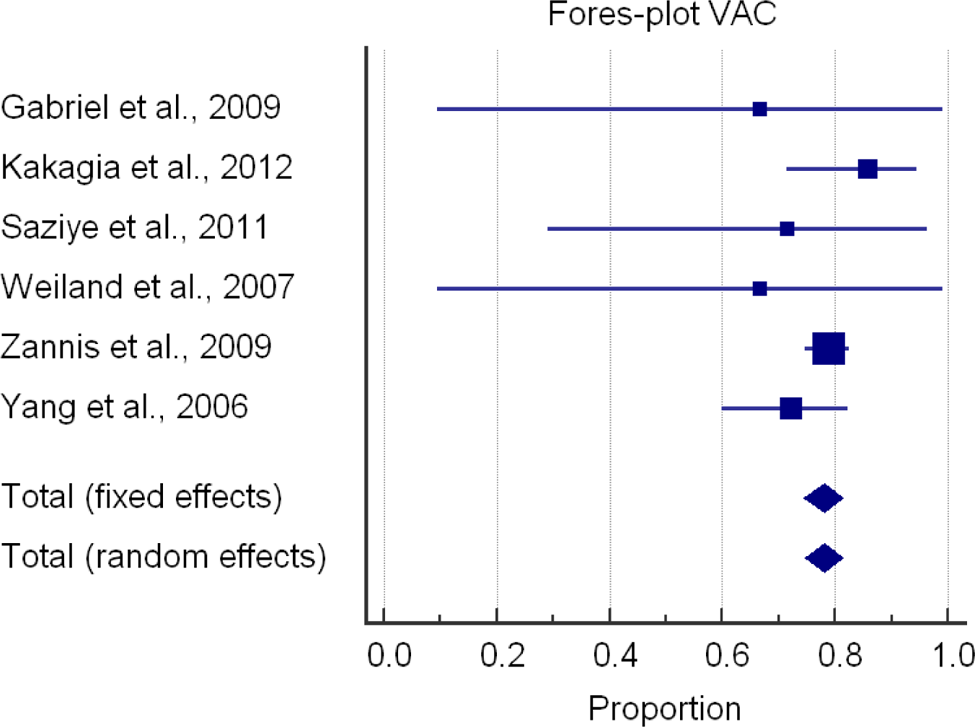
Proportion of patients who achieved closure with vacuum-assisted closure (VAC).
In terms of complications following wound closure, VAC had the lowest rate of 2.49% (8 of 321 closures). This was followed by gradual suture approximation, with a complication rate of 14.83% (31 of 209 closures). The highest complication rate was observed with dynamic dermatotraction, in which 18.4% of the limbs developed a complication (14 of 76 closures). The specific details of the complications observed with different methods are displayed in Tables 4–6.
Discussion
There is no consensus in the literature regarding the best method for the closure of fasciotomy wounds in ACS. Different techniques carry their own inherent complications. 7,8 In addition, the underlying mechanisms of injury leading to the compartment syndrome may result in further wound-related complications and may result in amputation or death. The purpose of this study was to systematically review the current literature to assess the current evidence regarding fasciotomy closure techniques. After evaluating 23 studies, we were able to determine that the highest success rate was observed for dynamic dermatotraction (93%) and gradual suture approximation (92%), followed by VAC (78%). However, VAC had the lowest complication rate (2%), followed by gradual suture approximation (15%), and then dynamic dermatotraction (18%).
There are several limitations to this study. Many of the studies were case series with small sample sizes. Small samples sizes are due to a number of factors, including the heterogeneity of the patient populations in each study. This is partly due to the fact that ACS is caused by many factors, resulting in surgeons reporting their outcomes based on a wound closure technique employed on a mixed patient population.
Even for those studies with larger sample sizes, many were retrospective and/or uncontrolled. Study designs may have contributed to this bias. For example, larger or more severe wounds may have been closed more commonly with one technique over another, leading to higher failure or complication rates for that technique. For similar reasons, we were unable to determine if there is a correlation between mechanism of injury and risk of complications. For example, amputations following fasciotomy closure are generally due to the underlying mechanism of injury that precipitated the compartment syndrome, rather than the closure method itself. Thus, more severe mechanisms of injury that are more likely to result in amputation would be expected to have higher complication rates, regardless of the closure method. This could not be separately analyzed here due to lack of individual patient data. In addition, due to the lack of studies supporting the use of static tension techniques with plaster strips or Steri-Strips (3 M Surgical Products, St Paul, Minnesota, USA), these were not evaluated in this study. 3,15,61
Currently, there are many surgeons who prefer VAC systems. In this meta-analysis, these systems had the lowest success rate but also had the lowest complication rate. In our study, defining success as closure without STSG may not be an accurate representation of what a surgeon deems successful, following a severe extremity injury requiring fasciotomies. Furthermore, in a patient who is already at high risk for complications due to the severe nature of the injury that lead to ACS, VAC systems may be the best choice. The choice of using a VAC system, however, also depends on the resources available, as these systems are expensive. Whether this up-front expense is a cost-effective means to avoid complications is outside the scope of this study.
Conclusion
Following a fasciotomy, wound closure is a topic that is controversial. The preference of the orthopedic community for one technique over another varies over time, is influenced by the availability of resources, and institutional familiarity with certain techniques. We believe that the ultimate decision should be individually based, according to the specific clinical situation. The purpose of our study was never to recommend one device over another. However, when primary closure is the main goal, devices that produce dynamic dermatotraction could be beneficial. When the patient is at high risk for complications, vacuum-assisted systems may be a better alternative.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.