
Abstract
Purpose
Acute compartment syndrome often requires additional surgery to achieve wound closure. Little information exists regarding the expected number of surgeries, techniques and complications after closure in paediatric patients.
Methods
A retrospective chart review identified patients treated for acute compartment syndrome at four hospitals over a ten-year period. The cause of injury, type of dressing, number of surgeries, type of closure and complications were recorded.
Results
In all, 32 patients (mean 10.9 years, 1 to 17) who underwent 18 lower and 14 upper extremity fasciotomies met inclusion criteria. Definitive wound closure technique was delayed primary in 72%, split thickness skin graft in 25%, and primary in 3% of patients. Closure required a mean 2.4 surgeries (0 to 4) over a mean 7.7 days (0 to 34). Days to closure and number of surgeries required were not significantly affected by mechanism of injury, fasciotomy location or type of dressing used. A total of 23.1% of patients with upper extremity and 0% with lower extremity fasciotomies had concerns about the scar appearance. Other complications included neurapraxia (6.7%), stiffness (6.7%), swelling (3.3%), scar pain (3.3%) and weakness (3.3%).
Conclusions
The most common complication after paediatric compartment syndrome is an unpleasant scar. Wound closure after upper or lower extremity fasciotomies in paediatric patients requires a split thickness skin graft in approximately one in four patients. However, avoiding a skin graft does not guarantee the absence of cosmetic concerns, which are more likely following upper extremity fasciotomies.
Level of Evidence
IV
Introduction
Acute compartment syndrome (ACS) occurs in 1% of paediatric forearm fractures 1 and up to 12% of adolescent tibia shaft fractures. 2 Without proper treatment, the clinical complications can be devastating. Medicolegal implications of ACS are also important, as physicians are found negligent in > 50% of cases.3,4
Previous reports in paediatric patients have focused on the diagnosis and outcomes of ACS, with less attention towards the number, type and complications of surgeries required for wound closure.5–7 With little information available, it is difficult to provide families with evidence-based expectations regarding the need for skin grafting and the number of additional surgeries after a fasciotomy is performed.
Our objective was to describe the methods and complications of wound closure after fasciotomy for paediatric ACS in order to provide more accurate expectations for families when a diagnosis of ACS is made. Our hypothesis was that closure of upper extremity fasciotomies would require less surgeries and be more amendable to delayed primary closure than lower extremity fasciotomies.
Patients and methods
Institutional Review Board approval was obtained in order to initiate the study. A combination of Current Procedure Terminology codes for fasciotomy and International Classification of Diseases-9 codes 8 for compartment syndrome were utilized to identify patients treated for ACS over a ten-year period (2006 to 2016) at four different hospitals. The physicians treating patients at these hospitals are part of a single hospital system and share an electronic medical record. Two of the hospitals are teaching hospitals and one hospital is a level 1 trauma centre. Prophylactic fasciotomies prior to the development of ACS (e.g. elective surgery, fracture surgery, vascular repair) and fasciotomies for necrotizing fasciitis were excluded.
A retrospective chart review was performed to confirm the diagnosis and treatment codes, identify injury ACS characteristics including the aetiology and treatment of the underlying cause. In addition, fasciotomy location, compartments released, time from injury to fasciotomy and dressing type were recorded. Wound closure data included postoperative dressings, final closure technique, number of surgeries and days until closure. Outcome measures included functional limitations, scar concerns and other complications related to the ACS or the underlying cause.
Patients were divided into seven mechanism categories (bicycle/car/all-terrain vehicle accident, fall, sports injury, infection, laceration and postoperative/post-procedure). Analyses were descriptive based on distributions of results. Descriptive statistics were performed and data expressed as mean and standard deviation. Comparisons between groups were done using two-tailed unpaired t-tests, Mann-Whitney U if data were not normally distributed or single factor analysis of variance. Correlation coefficients were calculated using the Pearson r test. Significance was defined as p < 0.05. All statistics were done using GraphPad InStat version 3.00, GraphPad Software (San Diego, California).
Results
Patient characteristics
In total, 32 patients, mean age 10.9 years (1.0 to 17.0) underwent fasciotomy for ACS during the study period. There were 19 male and 13 female patients. In all, 25% of patients (8/32) had a positive past medical history, including two with skeletal dysplasias.
ACS characteristics
There were 18 lower extremity and 14 upper extremity fasciotomies. Compartment syndrome was secondary to a fall in ten patients, a postoperative or post-procedural complication in seven patients, a sports injury in six patients, an all-terrain vehicle/bicycle/motor vehicle accident in five patients, an infection in three patients and a laceration in one patient.
In all, 59.4% (19/32) of cases were associated with fractures (Table 1), all of which were treated surgically. A total of 31.6% (6/19) underwent fasciotomy at the time of fracture surgery while 68.4% (13/19) required fasciotomy a mean 0.9 days (0.05 to 2.0) after surgical treatment. A total of 40.6% (13/32) of cases were not associated with fracture (Table 2).
Fractures with subsequent acute compartment syndrome
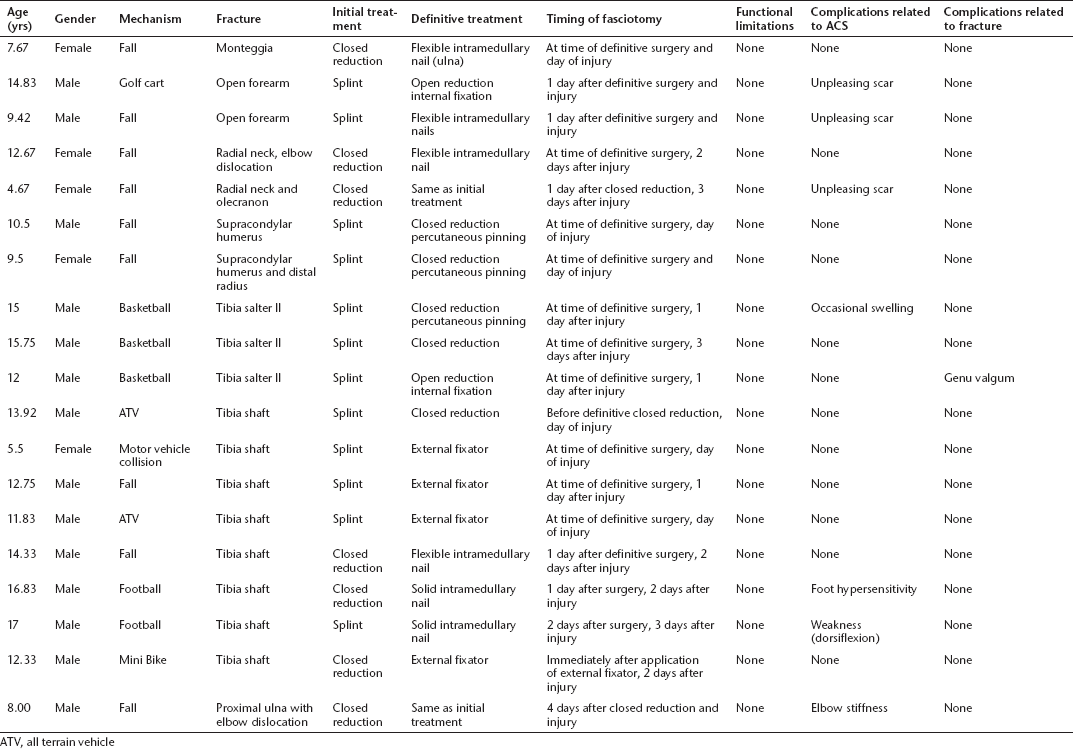
ATV, all terrain vehicle
Nonfracture causes of compartment syndrome
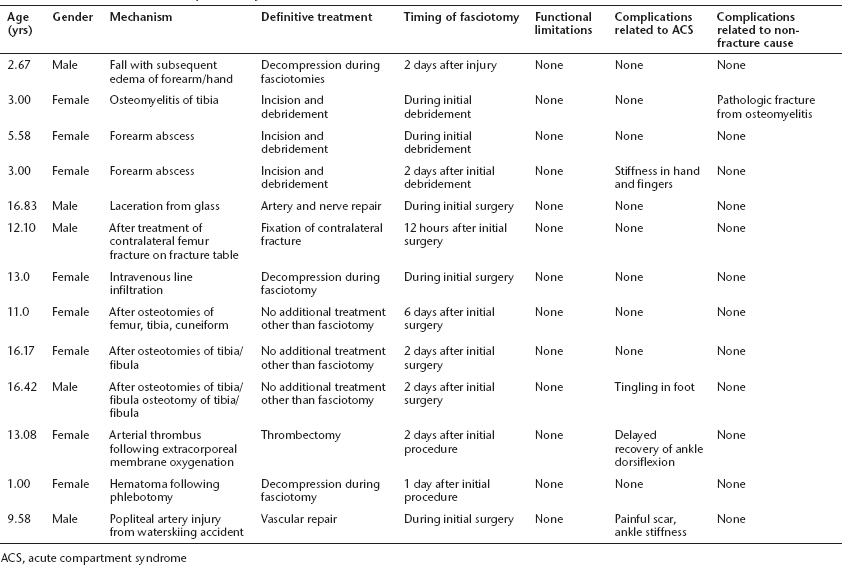
ACS, acute compartment syndrome
Wound closure
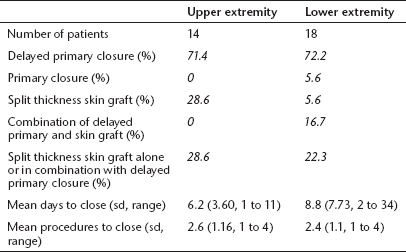
Wound closure required a mean 2.4 surgeries (0 to 4) at a mean 7.7 days (0 to 34) after fasciotomy (Table 3). The average number of days between surgeries was 3.0 (0 to 8.5). In all, 84.3% of closures were performed by an orthopaedic surgeon and 15.6% by a plastic surgeon. A full-time paediatric plastic surgeon was not available at all four hospitals. The final wound closure technique was delayed primary in 71.9%, split thickness skin graft (STSG) in 15.6%, a combination of delayed primary and STSG in 9.4% and primary (closed at the time of fasciotomy) in 3.1%. One fasciotomy wound was able to be closed before the other in seven lower extremities (four medial before lateral, three lateral before medial) and two upper extremities (hand before forearm) cases. Fasciotomies amendable to delayed primary closure were similar for the upper (71.4 %) and lower (72.2%) extremities. There was no significant difference between upper and lower extremity fasciotomies for days to closure (p = 0.58) or number of surgeries required (p = 0.69).
Wound closure technique for upper and lower extremity fasciotomies
The mean number of days to closure was 4.5 (1 to 11) in 11 patients with gauze dressings, 7.2 (2 to 12) in 15 patients with vacuum-assisted closure (VAC) device dressings and 15.8 (6 to 34) in five patients with a combination of dressings. The mean number of wound closure surgeries was 1.9 (1 to 4) in the gauze group, 2.6 (1 to 4) in the VAC group and 3.4 (3 to 4) in the patients with mixed dressings. Vessel loops secured to skin staples were typically used to decrease wound size in both VAC and gauze cases. The differences between dressing types for days to closure (p = 0.06, r = 0.34) or number of surgeries required (p = 0.53, r = 0.12) were not significant. There was also no significant difference between mechanisms of injury for days to closure (p =0.43) or number of surgeries required (p = 0.52).
Outcomes
In all, 30 patients (93.6%) were followed for more than one month, a mean 11.1 months (1.6 to 41.7). Outpatient follow-up did not occur after ACS in one patient with an upper extremity intravenous line infiltration and one patient with a closed tibia fracture. Both were treated with delayed primary closure.
In all, 36.6% (11/30) of patients developed a complication related to the ACS. A total of 10% of patients had concerns about the scar appearance; 23.1% of upper extremity and 0% of lower extremity fasciotomies (p = 0.081). Scar concerns after upper extremity fasciotomy occurred in 22.2% (2/9) after delayed primary closure and 25% (1/4) after STSG. While none of the lower extremity fasciotomies had cosmetic concerns, one patient (5.8%) closed with a STSG had a painful scar which required surgery. None of the other seven patients treated with STSG required resection or other types of reconstructive surgery. These scar-related complications occurred in 12% (3/25) of wounds closed by orthopaedic surgeons and 20% (1/5) closed by plastic surgeons (p = 0.54). Other complications included neurapraxia in 6.7% (2/30), stiffness in 6.7% (2/30), swelling in 3.3% (1/30) and weakness in 3.3% (1/30). There were no postoperative infections.
There were no complications related to the underlying cause in 93.1% of patients. One patient (3.4%) with a proximal tibia fracture developed genu valgum and one patient (3.4%) with osteomyelitis sustained a pathologic fracture. No patients developed any functional limitations related to the ACS or underlying cause.
Discussion
Our review of ACS treated at four centres included fracture (59%) and non-fracture (41%) causes with subsequent upper (44%) and lower (56%) extremity fasciotomies. We focused our analysis on timing, methods and complications of wound closure in order to provide families with more accurate expectations after the development of ACS. We anticipate that providing realistic expectations can improve the patient experience after fasciotomy, as has been demonstrated for satisfaction with surgery for spinal stenosis 9 and outpatient orthopaedic visits. 10
We found that patients and families can expect approximately two additional surgeries for wound closure. Shore et al 2 also reported an average of two additional surgeries for closure in a series of 25 teenagers with ACS associated with a tibial shaft fracture. We found that time until wound closure was approximately seven days. This finding is similar to a series of three cases of upper extremity ACS after intramedullary nailing with a mean 7.7 days (5 to 8) to closure via delayed primary closure or STSG. 11
We found approximately 25% of patients required a skin graft procedure for wound closure. Our rate of skin graft procedures was higher than Bae et al 12 who reported 12% of 33 children with upper or lower extremity fasciotomies for ACS required STSG. Of those 33 patients, 58% of patients underwent delayed primary closure and 30% were closed primarily. 12 Our rate of skin graft procedures was also higher than 39 cases of non-fracture ACS reported by Livingston et al 13 that required a skin graft in 15% and a tissue expander in 5%. These differences in the need for skin grafting may be secondary to surgeon training regarding closure at the time of fasciotomy and the threshold to proceed with delayed primary closure. Differences between the injuries included in the studies may be a factor as well.
Complications related to the compartment syndrome were not uncommon, occurring in 37% of patients. The most common complication was an unpleasant scar, all following upper extremity fasciotomies. While delayed primary closure avoids donor site morbidity associated with a STSG and should result in a better appearance, we found that avoiding STSG in the upper extremity does not guarantee a pleasing scar. It is important to forewarn patients and families that the upper extremity scars in particular may be displeasing. This finding is likely due to the more visible upper extremity, which makes the scar appearance more concerning, rather than differences in wound healing between upper and lower extremities.
Our hypothesis that closure of upper extremity fasciotomies would require less surgeries and be more amendable to delayed primary closure than lower extremity fasciotomies was false. The number of surgeries required for closure (mean 2.6 versus 2.4) and the percentage of fasciotomies treated with delayed primary closure (mean 71% versus 72%) were similar for upper and lower extremity fasciotomies, respectively.
We were unable to identify the optimal dressing after fasciotomy. While no infections were noted with any of the dressings in our series, other factors to consider are pain and cost. Daily wet to dry dressings are often too painful for young children to tolerate and can become moist and uncomfortable between changes. At one centre included in the study, the cost of a medium VAC sponge and canister is $85 compared with 32 cents for a 12 pack of 4 × 4 gauze sponges.
Despite the higher cost of the VAC sponge, these dressings may be more effective in facilitating closure of fasciotomy wounds.14,15 Zannis et al 15 retrospectively reviewed 804 fasciotomy wounds in adult patients over a ten-year period. There was a significantly higher rate of delayed primary closure using the VAC (83%) than wet-to-dry dressings (56%). The time to definitive closure was slightly shorter using the VAC (mean 5.2 days versus 6.5 days). Patient satisfaction was significantly greater in the wound VAC group. In a smaller retrospective series of 15 adult patients, Saziye et al 14 reported a lower mean number of days to closure in patients treated with a VAC (mean 11, 8 to 13) than those with gauze dressings (mean 15, 12 to 20). There were also more infections in the gauze group (three) than VAC group (none). 14 Although our data showed a shorter time to closure with gauze dressings, this finding did not reach significance. While further studies are needed in the paediatric literature, routine VAC placement before closure is worthy of consideration as the ability to avoid frequent gauze dressing changes seems to outweigh the increase in cost. 16
The rates of scar complaints were not significantly different in closures performed by orthopaedic and plastic surgeons. The need for a plastic surgeon to perform wound closure is likely best determined by the treating orthopaedic surgeon. Factors to consider include soft-tissue injury severity and the practice scope of both surgeons. For example, a paediatric orthopaedist in a general practice may have more experience with fasciotomy closure than a plastic surgeon in a cosmetic practice but less than a plastic surgeon in a trauma centre. Further study would be helpful to determine if routine consultation with plastic surgery is warranted.
Weaknesses of our study include those inherent to retrospective reviews. The use of formal outcome measures may have identified further differences between the closure methods. The use of functional outcome measures may also have identified limitations that the clinical exam and medical record did not. Similarly, as the hospitalization for an ACS is a stressful event, a satisfaction measure to evaluate the family experience may have identified useful information including preferences of the wound VAC over gauze dressings. Finally, longer follow-up may have demonstrated a change in the complication rate including patients treated with STSG that later required reconstructive surgery.
Many of the decisions made during the treatment of ACS are subjective and fall into a ‘grey area’. These decisions include when to proceed to fasciotomy, how many compartments to release, and when wound tension is satisfactory for closure. In addition, techniques such as measuring pressures during delayed closure and optimal soft tissue handling to achieve earlier closure in order to prevent infection may facilitate better outcomes. It would be very helpful to report knowledge gained and lessons learned from these decisions and techniques. Unfortunately, this information is better derived from a case-by-case oral review with the team involved rather than a retrospective review.
In summary, we found that wound closure for ACS requires approximately two additional surgeries over the course of one week. We found that approximately 25% of patients required a skin graft procedure but avoiding a STSG did not guarantee a pleasing scar in the upper extremity. These findings may facilitate the setting of appropriate expectations after an ACS is diagnosed. Further research is needed to identify techniques that minimize scar complications after fasciotomy closure.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.