
Abstract
Chronic exertional compartment syndrome can be a debilitating cause of lower leg pain that typically affects young, healthy people during a variety of aerobic activities. Conservative management has produced a poor success rate and numerous techniques for surgical decompression have been described. Many of these, however, involve blind fascial dissection which increases the risk of direct nerve injury or insufficient fascial release. We describe a novel technique of mini-open fasciotomy using a lighted retractor which enables direct visualization of the fascia and the superficial peroneal nerve using a single, small incision. By the use of a 3- to 4-cm laterally based incision, a lighted retractor with fiber-optic illumination is introduced into the subcutaneous plane and advanced distally and proximally. The retractor gently elevates the subcutaneous tissues while focusing light directly into the surgical area and a long Metzenbaum scissors is then used to release the fascia under direct vision. Fasciotomy using this technique avoids the risks of blind fascial release and is a straightforward, safe, and effective method for compartment decompression.
Keywords
Introduction
Chronic exertional compartment syndrome (CECS) is an effort-induced pathological elevation of pressures within a noncompliant osteofascial space, resulting in inadequate tissue perfusion and ischemic-type pain. Although most commonly seen in the lower leg, CECS has also been described in the thigh, the forearm, and the medial compartment of the foot. 1 –3 The condition typically affects young, healthy people and can be particularly debilitating for high-level athletes who are prevented from participating in sports and other activities.
Nonoperative treatment using stretching protocols and activity modification has proved largely unsuccessful, 4 and the majority of patients will ultimately require surgical compartment release. A variety of approaches to decompressive fasciotomy have been described. The traditional technique of open fasciotomy, although necessary in the acute setting, involves an incision along the entire length of the leg, requires a long recovery time, and is undesirable in patients who are keen to regain their normal activity level as soon as possible. As in other specialities, minimally invasive approaches have gained popularity in orthopedics, and subcutaneous fascial releases through one or more limited incisions are the current mainstay of treatment; however, these all involve the blind passage of a scissors or fasciotome along the affected compartment, which may result in incomplete fascial release or injury to neurovascular structures that cannot be visualized. Endoscopically assisted techniques attempt to improve visualization, but these can be time-consuming, technically demanding procedures that require special instrumentation. We describe a novel technique of mini-open fasciotomy using a lighted retractor which avoids the complexity of endoscopic release while still allowing a minimally invasive approach and optimum visualization of the fascia and superficial peroneal nerve (SPN).
Operative technique
Under general anesthesia and with the patient supine, the lower limb is prepared and draped in a sterile fashion. Although we apply a tourniquet, we prefer not to inflate it so that any bleeding can be controlled at the time of surgery, reducing the risk of postoperative hematoma. A 3- to 4-cm longitudinal incision is made approximately in the middle of the lower leg, midway between the tibial crest and the anterior fibular border. This allows the anterior and lateral compartments to be accessed through a single mini-incision which is centered on the SPN. Once the skin is incised, the subcutaneous tissues are bluntly dissected and gently undermined proximally and distally. The deep fascia overlying the muscle is exposed, and the anterior intermuscular septum and any subcutaneous portions of the SPN are identified. Using a No. 15 scalpel blade, two small fascial incisions are made, one in the anterior compartment and one in the lateral compartment. A single-blade lighted retractor (Tebbetts™ Fiberoptic Lighted Retractor, Empire Medical, UK; blade length 15 or 19 cm options, diameter 3 cm; Figure 1) is then inserted into the subcutaneous plane and advanced distally (Figure 2). The broad blade gently elevates subcutaneous tissues of the fascia, while an LED mounted on the tip of retractor delivers white cool light directly into the surgical area. This provides an excellent view of the entire fascial compartment without compromising the field of vision. A long Metzenbaum scissors is then used to release the fascia under direct visualization down to the level of the ankle with the SPN in direct view throughout its course. The technique is repeated proximally and the fascia of the anterior compartment can be released in a similar manner. The fascial incisions are completed, care is taken to assess for bleeding and after irrigation, the wound is closed in layers with absorbable sutures. A compressive wrap is applied for the initial 48 h to reduce the risk of hematoma formation. Full weight-bearing as tolerated is allowed, but crutches are typically required in the immediate postoperative period for comfort. Patients are advised to limit their activity until their wounds are fully healed and a full return to sports is generally accomplished within 8–10 weeks after surgery.
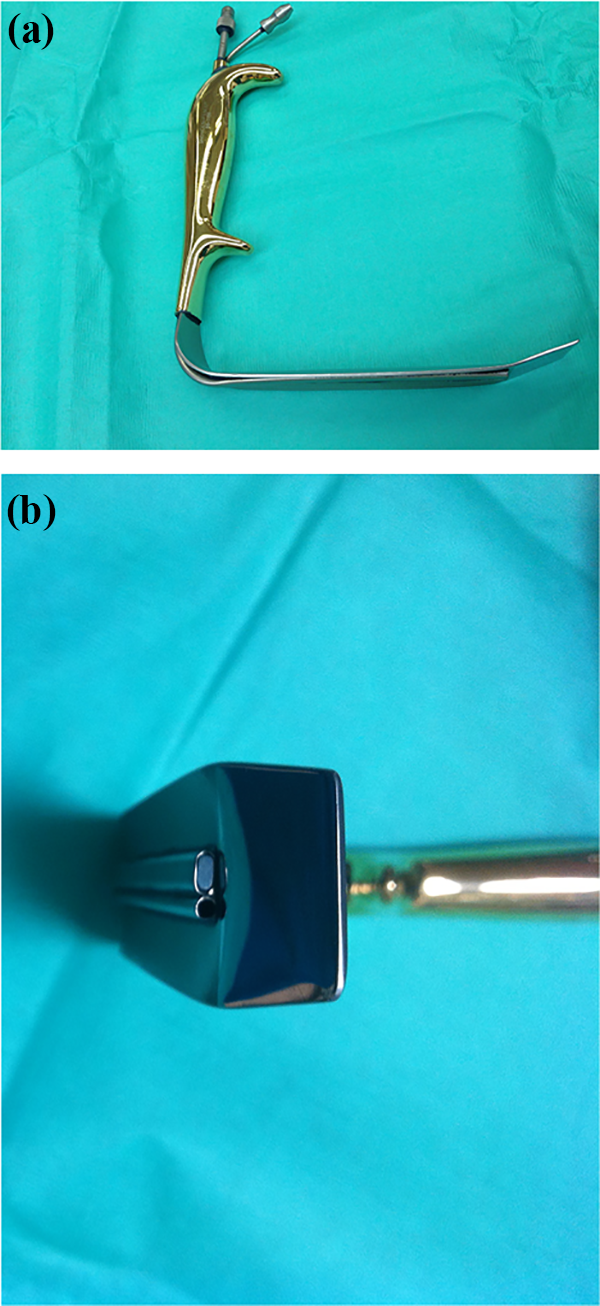
(a) Lighted surgical retractors can be used to optimize visibility in a small incision setting. Features include an ergonomic handle, is a broad blade that is not traumatic to subcutaneous vessels and nerves, and (b) an LED mounted on the retractor tip which delivers light via a fiber-optic cable from a high-intensity light source.

A lighted retractor is introduced into the subcutaneous space and advanced distally to provide excellent visualization of the fascia and SPN. SPN: superficial peroneal nerve.
Discussion
First described by Mavor in 1956, 5 CECS can be a debilitating and often undiagnosed cause of lower leg pain in young, healthy patients. Although most commonly seen in athletes, particularly those involved in running or endurance sports, CECS can also occur in nonathletic or sedentary individuals who have activity-related leg pain. 6 The anterior compartment is most commonly involved (45%), followed by the deep posterior (40%), lateral (10%), and superficial posterior compartments (5%). 7
The etiology of the process remains incompletely understood, but it is generally accepted that symptoms are related to an abnormal increase of compartmental pressure during exercise, leading to vascular occlusion and ischemic-type pain. The characteristic presentation is of recurrent, exercise-induced pain that occurs at a well-defined and reproducible point during exercise. Patients typically describe a dull aching, tightness, or burning over a specific compartment that increases in intensity to the point at which exercise must be stopped. Relief of symptoms only occurs with discontinuation of the activity. Patients classically have no pain or symptoms while at rest and assessment after exercise must be performed to complete the examination. Findings include pain and firmness over the involved compartment and muscle herniations through fascial defects can be palpated in up to 40–60% of patients. 8 Common sites include the anterior tibial border and the junction of the middle and distal one-thirds of the leg where the SPN exits the lateral compartment.
Nonoperative management of CECS has proved largely unsuccessful. 4 Conservative measures include activity modification, physiotherapy, ice, massage, and ultrasound, but the majority of patients experience symptom recurrence and ultimately require surgical decompression. Multiple types of fascial release have been described: open fasciotomy, 5,9 subcutaneous fasciotomy through a single incision, 6,10 a double incision, 11,12 or several small incisions 13 as well as fasciotomy with partial fasciectomy. 14 The traditional technique of open fasciotomy has the advantage of full visualization of the compartment, but it involves a long, invasive incision which can significantly damage subcutaneous tissues. Currently, the mainstay of treatment involves subcutaneous fasciotomy, with the majority of techniques now described involving one or more small incisions along the leg. All these procedures, however, require the surgeon to “blindly” pass a scissors or fasciotome along the compartment and the complication profile of elective fasciotomy is not insignificant (4–17%). 15,16 Persistent postoperative symptoms may be traced to inaccurate diagnosis but can also highlight the potential dangers of a blind technique of fascial release: failure to adequately decompress the compartment, nerve injury, unrecognized muscle herniations, and residual nerve entrapment. More recently, endoscopically assisted techniques have been described which seek to overcome these problems through improved visualization. However, they often require special equipment and can involve considerable technical difficulty with the surgeon being challenged to fit an arthroscope, a retractor, and long scissors into a tight space (Table 1).
Literature review of endoscopically assisted fasciotomy for CECS of the lower leg.

CECS: chronic exertional compartment syndrome; Nr: not recorded; PDS: polydioxanone.
a One patient did not resume preoperative activities due to subsequent ankle injury.
Mini-open fasciotomy using a lighted retractor represents a step down from the complexity of endoscopic procedures while still allowing a minimally invasive approach and optimum visualization of the tissues. We have performed this technique in five patients with excellent results. Three patients were affected on both sides and two patients were unilaterally affected. All patients returned to sport after 12 weeks and have had no further pain episodes. Postoperatively, there were no surgical complications. The technique requires only one small incision and involves no special equipment other than a lighted retractor and a long Metzenbaum scissors. The retractor focuses light directly into the surgical area without compromising the field of vision to provide excellent visualization of the fascia and the SPN. To the best of our knowledge, no other method has been described that allows for fascial release under direct vision through a small incision. Access to the entire length of the compartment is provided by the long blade of the retractor, while its broad surface minimizes damage to the soft tissues. Moreover, it is inexpensive, quick, and relatively easy to perform. We believe that this technique offers an additional choice to the surgeon which avoids the complications of blind fascial release and is a straightforward, safe, and effective treatment for CECS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.