
Abstract
Purpose:
This study aimed to evaluate the accuracy of the picture archiving and communication system (PACS) method in order to select the correction angle and gap in open-wedge high tibial osteotomy (HTO) and clinical results of the patients.
Material and methods:
This retrospective study analyzed 27 consecutive patients (30 knees) underwent open-wedge HTO using the PACS method between April 2013 and March 2015. Full-length lower limb radiographs obtained preoperatively and at the final follow-up were used to the percentages of crossing points of the weight-bearing line and tibial plateau with respect to the medial border and mechanical femur-tibia angle. Preoperatively predicted and postoperatively measured wedge angles and gaps were compared. The clinical results were evaluated using the Hospital for Special Surgery (HSS) knee score and the Knee Society score.
Results:
At the 20.5 months (12–26.5) follow-up, the weight-bearing line on the tibial plateau was corrected from 17.3% to 61.3%, and the mechanical femur-tibia angle was corrected from 7.3° varus to 3.1° valgus. No significant difference in preoperative and postoperative measured values was observed (p = 0.440 and p = 0.505). The mean HSS score increased from 66.7 to 88.8 (p < 0.001). The knee score and function score of Knee Society increased from 62.0 to 88.7 (p < 0.001) and from 60.2 to 91.7 (p < 0.001), respectively.
Conclusion:
In open-wedge HTO, correction of angular deformity based on the PACS method could be an accurate correction method and the good clinical results could be obtained.
Introduction
High tibial osteotomy (HTO) is usually performed in patients with medial knee osteoarthritis with varus deformity, and excellent clinical results have been reported by many studies. 1 –4 Preoperative planning for determining the correction gap and angle has a significant effect on the postoperative results of HTO; therefore, planning is one of the most important processes in HTO. 5 –7
One method of preoperative planning is identifying the intraoperative mechanical axis of the lower limb using the radiopaque line or electrocautery cord (cable method). Another is calibration using preoperative full-length weight-bearing lower extremity radiographs, especially with a picture archiving and communication system (PACS) or specialized software, such as PreOPlan or mediCAD. 8 –10 The cable method is feasible for real-time monitoring to locate the center of the hip and ankle joint; however, it can give different results due to non-weight-bearing status and increased radiation exposure to the surgeon and patient. In contrast, the PACS method calculates the correction angle and gap in weight-bearing status, where values that are more accurate could be obtained with less radiation exposure compared to those obtained by the cable method.
The purpose of this study was to evaluate the accuracy of the PACS method in order to decide the correction angle and gap in open-wedge HTO in patients with medial knee osteoarthritis by comparing the preoperatively planned values to the ones obtained postoperatively. In addition, we evaluated the relationship between the preoperative severity of varus deformity and the outcome of correction. We also evaluated the clinical results of the patients.
Materials and methods
In this retrospective study, we analyzed 27 consecutive patients (30 knees) with varus deformity and medial knee osteoarthritis who underwent open-wedge HTO with the PACS method between April 2013 and March 2015. The male-to-female ratio was 3:27, and the mean age of the patients was 54.4 years (33–61 years). The mean follow-up period was 20.5 months (12–26.5 months). All patients underwent medial open-wedge HTO with a TomoFix plate (Synthes GmbH, Solothurn, Switzerland). The inclusion criteria were (1) age <65 years, (2) body mass index (BMI) <30 kg/m2, (3) only medial-side pain, (4) high level of activity except running and jumping, (5) varus angle <15°, and (6) <10 of knee extension loss and >90° of knee flexion. The exclusion criteria were (1) flexion contracture >25°, (2) bicompartmental disease, (3) elderly patients with difficulty mobilizing, (4) BMI >30 kg/m2, and (5) meniscectomy in the compartment that is near the osteotomy site.
Preoperative planning and surgical techniques
In the planning stage, the patients underwent full-length anteroposterior lower limb radiography. The goal was to achieve target alignment passing through the Fujisawa point, that is, realigning the mechanical axis of the limb at the 62.5% point from the medial border along the longest medial-to-lateral width of the tibial plateau. 11
In order to compensate for the widening of the lateral joint space according to the laxity of the ligament, we performed full-length anteroposterior lower limb radiography while applying a valgus force to the knee joint with a hammer or hand. By using preoperative radiographs, we drew the lower limb weight-bearing line (line 1, S). After calculating the 62.5% point from the medial border along the mediolateral width of the tibial plateau, we drew an extension line connecting the center of the hip and the calculated point (line 2, S′). Subsequently, we drew a line connecting the lateral tibial osteotomy site (D) and the center of the ankle joint (line 3, DS) and a line connecting the osteotomy site and line 2 (line 4, DS′). The angle formed by lines 3 and 4 was determined to be the predicted correction wedge angle (α). A predicted osteotomy line (O) was drawn from the proximal extremity of the proximal tibiofibular joint to the predicted medial osteotomy site (approximately 4-cm inferior to the medial border of the tibial plateau), and a predicted opening line (O′) was drawn from line O at the determined correction angle (wedge angle, α). Using the triangle formed, we measured the predicted correction gap (wedge gap) at the cortical bone of the posteromedial tibia (Figure 1). 12
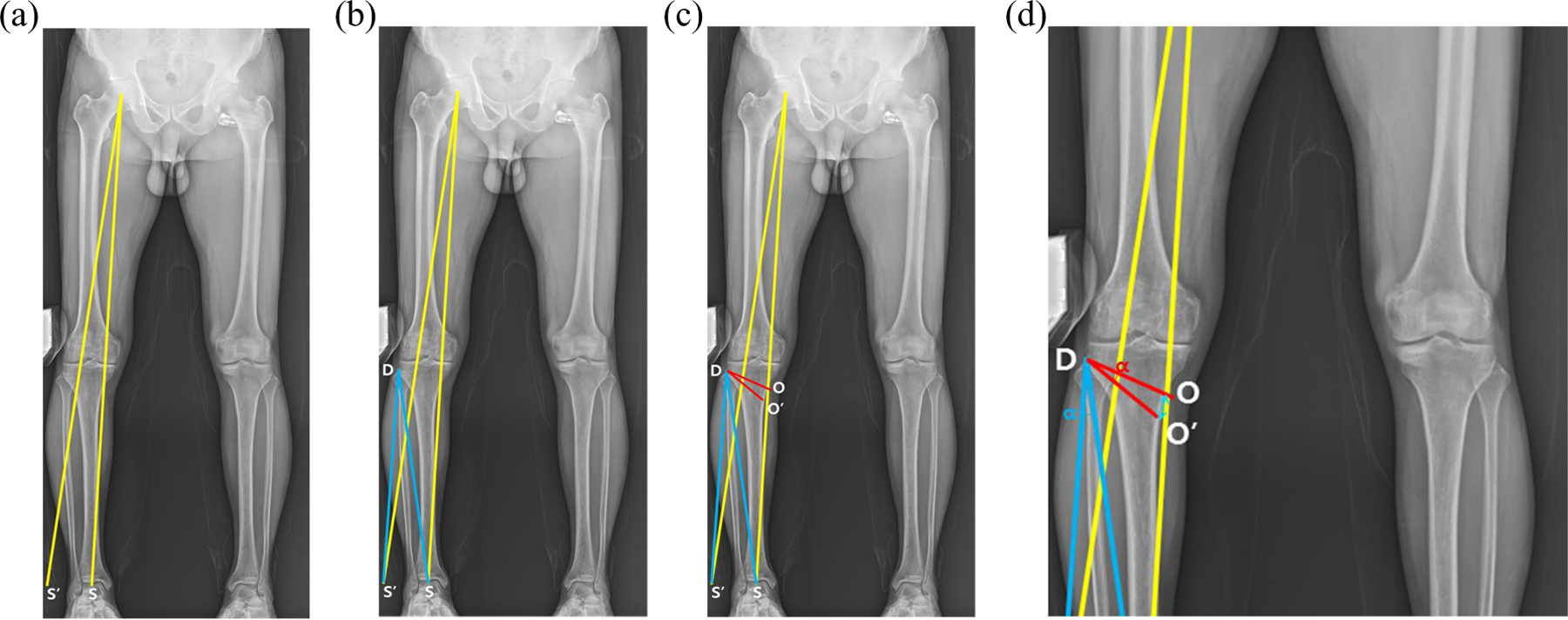
Planning performed using the PACS method. (a) First, using preoperative full-length anteroposterior lower limb radiographs obtained while applying valgus force around the knee joint, we drew the lower limb weight-bearing line (line 1, S). After calculating the 62.5% point from the medial border along the longest mediolateral width of the tibial plateau, we drew an extension line connecting the center of the hip joint and the calculated point (line 2, S′). (b) Then, we drew a line connecting the lateral tibial osteotomy site (D) and the center of the ankle joint (line 3, DS) and a line connecting the osteotomy site and line 2 (line 4, DS′). The angle formed by lines 3 and 4 was determined to be the predicted correction angle (α). (c) and (d). A predicted osteotomy line (O) was drawn from the proximal extremity of the proximal tibiofibular joint to the predicted medial osteotomy site (approximately 4-cm inferior to the medial border of the tibial plateau), and a predicted opening line (O′) was drawn from line O at the determined correction angle (wedge angle, α). Using the triangle formed, we measured the predicted correction gap (wedge gap) at the cortical bone of the posteromedial tibia. PACS: picture archiving and communication system.
The same surgeon operated on all patients, and they all underwent diagnostic knee arthroscopy before osteotomy for the verification of the conditions of the medial, lateral, and patellofemoral articular surfaces, followed by debridement. They underwent biplanar osteotomy behind the tibial tuberosity. Subsequently, the posteromedial tibial osteotomy site was opened using a chisel and bone spreader. We spread the osteotomy site matching the predicted wedge angle and gap and fixed the TomoFix plate. For maintaining the posterior tibial slope, the predicted wedge gap was matched at the posterior end of the osteotomy site, and two-thirds of the predicted gap was matched at the middle of the osteotomy site. Rotation was controlled by contacting the osteotomy site of tibial tuberosity. The superficial medial collateral ligament and pes anserinus were fully separated, and allogeneic bone and autologous bone marrow harvested from the anterior superior iliac spine on the same side were mixed and grafted onto the bone defect. The grafted site was covered with the superficial medial collateral ligament, and the pes anserinus was resutured to the periosteal membrane. An active exercise program for joint rehabilitation began in the second postoperative week, and the patients were allowed to commence body-weight-bearing at the same time.
For comparative evaluation, full-length lower limb weight-bearing radiographs obtained preoperatively and at the final follow-up were used to compare the percentages of crossing points of the weight-bearing line and tibial plateau with respect to the medial border. The acceptable postoperative range was set at 62.5 ± 5% (range: 57.5–67.5%), and percentages lower or higher than this range were defined as undercorrection or overcorrection, respectively. Preoperative and postoperative mechanical femorotibial angles (mFTAs) were compared. The acceptable postoperative range was set from 3 to 6° valgus. 13 Angles lower or higher than this range were defined as undercorrection or overcorrection. In addition, preoperatively predicted and postoperatively measured wedge angles and gaps were compared, and preoperative and postoperative posterior tibial slope angles were compared. The absolute differences between the preoperatively predicted and postoperatively measured wedge angles and gaps were analyzed. We also analyzed the relationship between the preoperative severity of the varus deformity and outcome of correction.
All patients were evaluated clinically preoperatively and, at final follow-up, using the Hospital for Special Surgery (HSS) knee score and the Knee Society score (knee score and function scores). 14,15
The radiographic measurements were performed by two observers. The correlation between the measurements by the two observers, determined using Spearman’s ρ test, was 0.85. We used the mean of the two measurements and conducted paired t-test to compare the preoperative and postoperative variables and clinical scores and logistic regression analysis to evaluate the relationship between the preoperative severity of the varus deformity and the outcome of correction. The absolute differences between the preoperatively predicted and postoperatively measured wedge angles and gaps were analyzed using the one-sample t-test. The null hypothesis of this test was the mean of the absolute difference greater than 2.5, while the alternative hypothesis was the mean of the absolute difference less than 2.5, which indicates an acceptable absolute difference. All statistical analyses were performed using the SPSS software version 19.0 (IBM Co., Armonk, New York, USA), and a p value <0.05 was considered statistically significant.
This study was approved by the institutional review board of our institution (no. 2015-05-022).
Results
The weight-bearing line on the tibial plateau was corrected from a preoperative mean of 17.3 ± 11.1% to a postoperative mean of 61.3 ± 6.3% (p < 0.001). The mFTA was corrected from a mean preoperative varus of 7.3 ± 2.7° to a mean postoperative valgus of 3.1 ± 2.0° (p < 0.001) (Figure 2(a) and (b)). Twenty-one cases of correction were within the acceptable range (70%, 63.4 ± 2.4%), six cases were undercorrections (20%, 51.2 ± 4.6%), and three cases were overcorrected (10%, 70.7 ± 2.5%) based on the weight-bearing line on the tibial plateau. Twenty cases of correction were within the acceptable range (66.7%, 4.0 ± 0.9°), nine cases were undercorrected (30%, 0.6 ± 1.6 valgus), and one case was overcorrected (3.3%, valgus 6.1°) based on the mFTA.

(a) Preoperative weight-bearing whole extremity AP radiograph shows a varus deformity in both knees, the weight-bearing line passes through 34.7% from the medial border along the medial-to-lateral width of the tibial plateau, and the mFTA was 5.9° under valgus force from the lateral side. (b) Postoperative weight-bearing whole extremity AP radiograph shows that weight-bearing line passes through 63% from the medial border and the mFTA was 4.7° valgus, which was corrected within the acceptable range. (c) and (d) Postoperative lateral X-ray shows 1° increase in the posterior tibial slope compared to the preoperative angle. mFTA: mechanical femorotibial angle.
The mean preoperatively planned wedge angle and gap were 10.8 ± 2.6° and 13.2 ± 3.2 mm, respectively. The mean postoperative achieved wedge angle and gap were 11.1 ± 2.1° and 12.9 ± 2.3 mm, respectively. The overall difference between the preoperatively planned and postoperatively achieved wedge gap and angle was statistically insignificant (p = 0.440 and p = 0.505; Table 1). The mean preoperative and postoperative posterior tibial slope angles were 9.8 ± 2.6° and 10.5 ± 2.3°, respectively. The difference between the two values is 0.7° (p = 0.002) (Figure 2(c) and (d)). The mean of the absolute differences between the preoperatively predicted and postoperatively measured wedge angles and gaps was 1.6 and 2.0, respectively; both values were significantly lower than our acceptable values (p < 0.001 and p = 0.030, respectively). The preoperative severity of the varus deformity has no significant effect on the outcome of correction based on the weight-bearing line on the tibial plateau (p = 0.593) and the mFTA (p = 0.262).
Results of HTO using the PACS methods.

HTO: high tibial osteotomy; PACS: picture archiving and communication system.
The clinical scores were all improved postoperatively. The mean HSS score increased from 66.7 ± 13.6 to 88.8 ± 5.6 (p < 0.001). The knee score and function score of Knee Society increased from 62.0 ± 16.3 to 88.7 ± 7.4 (p < 0.001) and from 60.2 ± 14.2 to 91.7 ± 6.5 (p < 0.001), respectively (Table 2).
Clinical results of the patients.

HSS: Hospital for Special Surgery.
Discussion
In this study, no differences between the preoperatively planned wedge angle and gap using the PACS technique in HTO and the postoperatively achieved values were found. The absolute differences between the preoperatively predicted and postoperatively measured wedge angles and gaps also showed satisfactory results. Clinical results were also improved postoperatively. Using HTO for the treatment of arthritis is based on the concept of realigning the mechanical axis, so that the weight-bearing stress can be distributed through correction of the deviated knee joint angle. Therefore, preoperative planning is highly important and affects the results of the surgery. 16,17 Many planning methods are reported by several authors. 11,17 –19
A method using a navigation technique has been recently published, and accurate and good clinical results were achieved in many studies. 18 –21 However, this method was applied under the non-weight-bearing status, which could cause differences under weight-bearing conditions. However, it was reported that it had no advantage over the conventional method regarding its efficacy in relation to medical costs. 22
The criteria used vary depending on the method. Amendola and Bonasia 2 reported planning using the mechanical axis as criteria, whereas Kettelkamp et al. 6 and Miniaci et al. 12 used the mechanical axis, and Marx et al. 10 and Sabharwal and Zhao 23 used the weight-bearing line. The weight-bearing line reflects the instability around the knee joint and deviates from the mechanical axis.
Many surgeons still conduct intraoperative monitoring by using the radiopaque line. This can cause undercorrection by non-weight-bearing measurement and increased radiation exposure to both surgeons and patients due to increased fluoroscopy duration for identifying the center of the hip and ankle joints and the degree of correction. Lee et al. 24 and Marx et al. 10 reported that methods using PACS are reliable.
We planned the preoperative angle and gap using PACS and found no significant differences between the preoperative planning and postoperative values. Moreover, satisfactory results were also obtained based on the weight-bearing line and mFTA, with 70 and 66.7% within the acceptable range, respectively, whereas the conventional intraoperative cable method showed unsatisfactory accuracy and increased variability of the mean correction. 18 Therefore, this technique could be effective for reducing radiation exposure, without significant differences compared to preoperative planning.
In this study, the severity of varus deformity did not affect the outcome of correction, which indicates that preoperative accurate planning is more important for the outcome of correction compared to the severity of varus deformity.
This study had some limitations. First, the number of cases was small. Second, the design of the study was retrospective and the follow-up period was short. Therefore, a long-term clinical study should be conducted in a large series. The thickness of the saw blade can affect the postoperative results; therefore, it should be considered during planning. In this study, the operation was performed as planned while applying valgus force around the knee joint, whereas postoperative measurements were performed without applying the valgus force. There was no point to apply the valgus stress because the load shift to the lateral side should already solve the problem of lateral laxity.
Conclusion
In open-wedge HTO, correction of angular deformity using PACS could be an accurate method, supported by the absence of significant differences between the preoperatively planned and postoperatively achieved values. The preoperative severity of the varus deformity had no significant effect on the outcome of correction. In addition, satisfactory clinical results were obtained.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.