
Abstract
Background:
C5 palsy is a serious complication after cervical decompression surgery in which the patient shows a deterioration in power of the deltoid or biceps brachii by at least one grade in the manual muscle test without aggravation of lower extremity function. Although there are several hypotheses regarding the etiology of C5 palsy, the pathogenesis and preventive measures remain unidentified and many other controversies remain.
Objective:
To systematically review the clinical features, risk factors, mechanism, and preventive measures of C5 palsy after posterior cervical decompression surgery.
Materials and methods:
PubMed was searched to identify eligible studies that contained more than 10 cases and focused on C5 palsy. Microsoft Excel was used to analyze the data. Statistical comparisons were made when appropriate.
Results:
Out of 718 papers involving C5 palsy, 28 met the inclusion criteria. The average incidence rate was 7.8% (range, 1.4–23.0%). Risk factors for C5 palsy included age, male gender, ossification of the posterior longitudinal ligament, and stenosis of the C4–C5 intervertebral foramen. C5 palsy occurred from immediately to 2 months after surgery, and recovery time ranged from 48 h to 41 months. Hypotheses for the mechanism of C5 palsy included root involvement and spinal cord impairment. Foraminotomy and intraoperative neuromonitoring were the two main methods used to prevent C5 palsy.
Conclusion:
C5 palsy is a serious complication occurring at the early stage after cervical decompression surgery. Foraminotomy and intraoperative neuromonitoring were the two main methods to prevent C5 palsy. The incidence of C5 palsy is low, but it can place a serious burden on the patients’ quality of life and finances. The risk factors and mechanism of C5 palsy are still controversial. However, under conservative therapy, the prognosis is usually good. Higher quality studies are necessary for drawing more reliable and convincing conclusions about this disease.
Introduction
Posterior cervical decompression surgery with laminectomy or laminoplasty is a well-established procedure that has been widely used for the treatment of cervical myelopathy caused by multilevel spondylosis and/or developmental spinal stenosis, or ossification of the posterior longitudinal ligament (OPLL). 1 The advantages of the posterior approach compared with the anterior approach include indirect decompression without destabilizing the disk space, intuitive operation while exposing multiple levels, and less risk of postoperative instability and adjacent level degeneration. 2–4 Studies have reported more satisfactory surgical outcomes using laminoplasty or laminectomy 5–8 ; however, postoperative problems, such as C5 palsy, axial pain, segmental instability, restriction of neck motion, perineural adhesions, and loss of lordotic curvature, have also been reported. 2–9
First described as a “dissociated motor loss” by Keegan, 10 C5 palsy is a serious potential complication after cervical decompression surgery in which patients show a deterioration in muscle power of the deltoid or biceps brachii by at least one grade in the manual muscle test (MMT) without aggravation of lower extremity function. Such a complication has been reported mainly after posterior cervical surgery, but has also been documented after surgery via the anterior approach. 11,12 Although many studies on C5 palsy after posterior cervical surgery have been published, the results are often inconclusive and even conflicting. 13,14
Here, we provide a systematic review of the current literature and attempt to analyze the conflicting results among studies to better understand the clinical features, influencing factors, and preventive measures of C5 palsy after posterior cervical surgery.
Materials and methods
A literature search was conducted on the PubMed database (http://www.ncbi.nlm.nih.gov/pubmed/) using the keywords “C5 palsy,” “laminectomy,” and “laminoplasty” with the limitations of human subjects and English language. We also included additional articles found by manual search methods from the references of the identified literature that contained relevant supporting information. The search was performed by two independent reviewers.
After excluding identical papers, we selected only peer-reviewed articles for inclusion. The included articles met the following criteria: Literature published between 1998 and 2014. Studies that consisted of 10 or more cases and focused on C5 palsy using statistical analysis. Articles referring to the posterior surgical approach, or both the posterior and anterior approaches.
Studies with one or more of the following criteria were excluded: Studies without a clear description and analysis of C5 palsy. Literature pertaining only to the anterior approach. Animal, cadaver, and biomechanical studies.
Articles with duplicate information. If more than one article was reported by the same authors from the same institution, the most recently reported article with detailed and complete clinical data was included. If an equal number of patients were reported by the same authors, the articles with the most information were selected.
The data extraction was done independently to minimize selection bias and errors. All abstracts that met our search terms were printed and thoroughly studied by two experienced spine surgeons. Different information extracted from the same article was compared and discussed. Discrepancies were resolved by a third reviewer where necessary. A final total of 28 studies were included in this systematic review. The full text of each study was carefully read, and data extraction was done independently by the authors mentioned above. All extracted data were imported into an electronic Microsoft Excel spreadsheet. A meta-analysis was not conducted, because very few studies specializing in C5 palsy were found, and there was too much clinical heterogeneity among studies. Hence, we have chosen to provide a qualitative descriptive analysis instead.
Results
Clinical features
Twenty-eight papers out of the initial 718 identified in PubMed met the inclusion criteria. This gave a total of 5115 cases, with the number of patients enrolled ranging from 19 to 630 in each study and a mean age of 40.25–70 years at the time of surgery. The duration of follow-up was approximately 9 months to 12 years. The incidence of postoperative C5 palsy varied markedly from 1.4% to 23.0%, with an average incidence of 7.8%. C5 palsy often occurred in the early postsurgical stage (from immediately to 2 months after surgery). The recovery time ranged from 48 h to 41 months (Table 1). Most patients experienced palsy of the deltoid muscle in the early postoperative stage, with symptoms subsiding gradually. 15–18 However, a palsy with MMT ≤ 2 was sometimes irreversible, 19 and often decreased patients’ quality of life and put a burden on their financial status by delaying their return to work after surgery. 18,20 The method employed to diagnose C5 palsy was the MMT, which divides the strength of the muscle into six grades from 0 to 5. Twenty-six out of the 28 included studies reported the risk factors for C5 palsy development (see Table 1).
Clinical features of C5 palsy after posterior cervical surgery.

CP: C5 palsy; FU: follow-up; yrs: years; mos: months; NA: not available; A and B group: A and group B in comparative study; MMT: manual muscle test; CSM: cervical spondylotic myelopathy; CSA: cervical spondylotic amyotrophy; CDH: cervical disk herniation; OPLL: ossification of longitudinal ligament; FG: foraminotomy group; NFG: non-foraminotomy group; LP: laminoplasty; CSR: cervical spondylotic radiculopathy; HIZ: high intensity; MVP: motor-evoked potential.
Risk factors
Age
The mean age at time of surgery was 40.25–70.00 years (Table 1). Of the 28 included studies, 5 listed age as the main risk factor. These five studies found that older age increased the risk of developing C5 palsy after posterior cervical surgery. 16,20–23 However, another five studies found no relation between age and the development of C5 palsy after surgery. 2,5,24–26 None of these studies further analyzed the relationship between this potential risk factor and C5 palsy development.
Gender
Seven out of the 28 included studies discussed whether sex influenced the incidence rate of C5 palsy (Table 1). Two out of these seven studies found that male gender was a risk factor for C5 palsy. Nassr et al. determined that the incidence of C5 nerve palsy after cervical spine decompressive procedures was 6.7%, with an increased risk in male patients 22 ; Nakamae et al. found that the incidence was 3.8% in males, which was significantly higher than the incidence in females of 1.9%. 16 The remaining five studies found no correlation between gender distribution of patients and C5 palsy after surgery. 2,5,24,26,27
Type of disease
The top three diagnoses were cervical spondylosis myelopathy (CSM), OPLL, and cervical disk herniation (CDH; Table 1). However, eight studies reported that patients diagnosed with OPLL had a higher tendency to develop C5 palsy than those with multilevel CDH or CSM. 3,6,16,21,24,28–30 Therefore, the type of disease had a significant relationship with postoperative C5 palsy development.
Preoperative foraminal stenosis
Foraminal stenosis is a recognized risk factor for C5 palsy, especially stenosis at the C4–C5 level (Table 1). The width of the foramen can be measured by a computed tomography (CT) scan of the cervical spine. Ten studies supported the concept of a relationship between C5 palsy and foraminal stenosis. 2,7,26,30–35 This adds the possibility that the etiology of C5 palsy is impairment of the C5 nerve root induced by a preexisting foraminal stenosis in patients who undergo posterior cervical surgery.
Surgical procedure
Two studies demonstrated that the use of internal fixation with fusion might add to the risk of C5 palsy. This was because iatrogenic foraminal stenosis may develop from an anterolisthetic vertebra being pulled posteriorly by the “lag correction effect” of the instrumentation. The cervical alignment correction with instrumentation may also increase tension of the roots and cord by posteriorly shifted cord more than those without the correction. 36,37
One study showed significant evidence indicating a higher risk of postoperative C5 palsy in open-door laminoplasty than in double-door laminoplasty; asymmetric decompression by open-door laminoplasty might introduce imbalanced rotational movement of the spinal cord and thus result in C5 palsy. 28 Two studies found that an increasing number of corpectomy levels had a higher incidence of C5 palsy. 21,23 One study reported that the incidence of C5 nerve palsy was highest for the laminectomy and fusion group, followed by the anterior corpectomy with posterior fusion group, the anterior-corpectomy-alone group, and finally the laminoplasty group. 22 However, another study found no differences in the incidence of C5 palsy among the surgical procedures when investigating anterior decompression and fusion laminoplasty versus laminectomy, or anterior versus posterior procedures. 21
Radiological assessment
Radiological examination included plain radiography, CT, and magnetic resonance imaging (MRI). The measurement parameters were defined as cervical alignment (C2–C7 Cobb angle), anteroposterior diameter (APD) of the spinal canal, cord-lamina angle (CLA), and high intensity areas (HIZ). One study reported that the cervical alignment was changed by traction of the internal fixation during surgery, which caused a significant cervical curvature index change rate between the palsy group and the non-palsy group 37 ; this study indicated that cervical alignment and cervical curvature index change rate were risk factors for C5 palsy. Another study found that a postoperative increase in cervical lordosis might be the cause of postoperative nerve root palsy. 6 Using CT scan results, one study suggested that greater CLA and APD can lead to posterior bowing and stretching following decompression. 35 Patients that have higher CLAs are theoretically predisposed to having more tethering of the C5 root following posterior decompression, which leads to the development of C5 palsy. Preoperative and postoperative MRI may also be able to predict C5 palsy; two studies found that the detection of HIZ in preoperative MRI and the expansion of this HIZ after surgery might be the reason for C5 palsy. 9,32 However, three other studies found no correlation between HIZ and the development of C5 palsy. 2,8,24
Discussion
Posterior cervical decompression surgery is generally considered safe and effective for cervical compressive myelopathy, but postoperative problems, such as C5 palsy, axial pain, restriction of neck movement, and loss of lordotic curvature, are also reported. 2 Although the incidence of C5 palsy is generally low, affected patients suffering from persistent muscle weakness, brachialgia, or numbness are dissatisfied with their surgery. It also puts a substantial burden on the patients’ economy and quality of life. 18,20,38 Hence, we conducted a systematic review to further investigate the risk factors for C5 palsy.
C5 palsy is recognized as a serious complication after cervical surgery. However, there are still several separate definitions of the condition. Takemitsu et al. defined postoperative C5 palsy as paresis of the deltoid muscle that develops after cervical spine surgery with no deterioration of myelopathy, with the deltoid muscle showing one or more grades of deterioration after surgery. 36 Katsumi et al. defined C5 palsy as deltoid muscle weakness of MMT grade 3 or less without any deterioration of myelopathic symptoms after surgery. 25 Liu et al. defined postoperative C5 palsy as paresis of the deltoid muscle that develops after cervical spine surgery with no deterioration of myelopathy. 37 Nakashima et al. defined C5 palsy as postoperative deterioration of muscle strength in the deltoid by one or more grades (determined by MMT on the deltoid muscle, with or without involvement of the biceps muscle), but no loss of strength in other muscles. 29 Yang and Fuh defined C5 palsy as upper extremity palsy weakness of grade 4 or less of the key muscles in the upper extremity by MMT without any deterioration of myelopathic symptoms after surgery. 38 A unified definition should be put forward in the future.
As mentioned above, C5 palsy is usually an early complication after posterior cervical surgery. Our systematic review found that the time of C5 palsy occurrence ranged from immediately to 2 months after surgery. Some studies also reported the occurrence of delayed onset C5 palsy. Yone et al. reported two cases of C5 palsy that occurred 5 and 7 years after surgery; they suggested that nerve roots may occasionally be compressed by degenerated facet joints and spurs that have developed at the entrance of root canal, resulting in segmental motor paralysis several years after laminoplasty. 39 Hence, careful long-term observation is necessary after cervical surgery.
C5 palsy is a common complication of postoperative cervical surgery, and although there have been several hypotheses regarding its etiology over the past years, the pathogenesis remains unidentified and many controversies remain. Two main pathogeneses were included in previous studies: the root involvement hypothesis and the spinal cord impairment hypothesis.
The root involvement hypothesis
Until the early 1990s, postoperative C5 palsy was considered to result from surgical trauma to the nerve root caused by instrumentation. 11,36,37 Another hypothesis concerns a tethering phenomenon in which a nerve root lesion might be produced by traction because of a posterior shift of the spinal cord in association with anchoring of the nerve root at the edge of the uncovertebral joint and/or the superior facet. 3,15,24,25,36,37 This hypothesis appears compatible with the anatomical features of C5 and the tendency toward unilateral shoulder pain and weakness of the deltoid muscle, 11 but it cannot explain why some cases occur several days and even months after surgery. Hence, the spinal cord impairment hypothesis was developed.
The spinal cord impairment hypothesis
The spinal cord impairment hypothesis involves segmental spinal cord disorder, spinal cord ischemia, and reperfusion injury to the spinal cord.
Segmental spinal cord disorder
HIZ in the spinal cord were seen on postoperative T2-weighted MRIs and were observed to expand after surgery on C3–C4 and C4–C5 in patients with C5 palsy. 2,9,32 Hence, researchers have postulated that C5 palsy may be associated with pathological damage to anterior horn cells at the gray matter of the spinal cord.
Spinal cord ischemia
Komagata et al. proposed that postoperative C5 palsy may result from ischemia of the spinal cord due to decreased blood supply from the radicular artery. They reported that the cervical cord is mainly perfused by the radicular arteries, and that the radicular artery at the C5 segment is the major source of blood supply. The fact that C5 palsy generally has a good prognosis for a functional recovery might support this idea. 31
Reperfusion injury of the spinal cord
Rapid reperfusion by oxygenated blood to the ischemic tissue might cause cellular injury and a paradoxical decrease in blood flow after surgery. Chiba et al. proposed that postoperative upper extremity paresis may be caused by deterioration of gray matter, and that local reperfusion injury in the spinal cord could be the pathomechanism. 8
Every theory remains hypothetical because of non-availability of reliable evidence for verifying their proposed mechanism.
Several preventive measures have been put in place to address the issue of postoperative C5 palsy, including intraoperative monitoring and modified surgery. In an effort to reduce postoperative C5 nerve root palsy, Fan et al. suggested the clinician should consider intraoperative deltoid and biceps transcranial electrical motor-evoked potential (MEP) and spontaneous electromyography monitoring whenever there was potential for iatrogenic C5 nerve root injury. 5 Yanase et al. reported a significantly higher incidence of waveform pattern changes in the paralytic muscle group than in the non-paralytic muscle group on monitoring of the intraoperative MEP. 33 However, Tanaka et al. observed no abnormalities on transcranial electric MEP monitoring, even in those patients who developed postoperative transient C5 palsy. 40 Therefore, intraoperative MEP monitoring is not an infallible way to prevent C5 palsy.
As to the surgical technique, several modified surgeries have been put forward to avoid the development of C5 palsy (Table 2). After a retrospective review of 305 patients, Komagata et al. declared that bilateral partial foraminotomy was effective for preventing C5 palsy. 31 Chiba et al. suggested that expansive open-door laminoplasty is the treatment of choice for cervical compressive myelopathy, giving favorable surgical outcomes and reduced prevalence of C5 palsy. 8 Radcliff et al. declared that a wider laminectomy at C5 was associated with an increased risk of postoperative C5 palsy. 27 Elective cervical laminectomy and fusion might be useful in avoiding C5 palsy. Dai et al. and Bydon et al. both proposed that longitudinal durotomy during cervical decompression surgery could reduce the prevalence of C5 palsy. 3,26 Since the use of internal fixation with fusion might add to the risk of C5 palsy for iatrogenic foraminal stenosis that develops from the cervical alignment correction with instrumentation, some studies suggested prophylactic foraminotomy is recommended to prevent this complication if foraminal stenosis exists preoperatively. 36,37 However, some modified surgery techniques also have their shortcomings. Ohashi et al. reported that prophylactic bilateral C4–C5 foraminotomy might affect cervical alignment and stability, hinge problems, and axial pain. 34 Thus, we recommend an individualized surgical plan for patients with cervical degenerative disease.
Modifications of posterior cervical surgery techniques for reduction of C5 palsy.
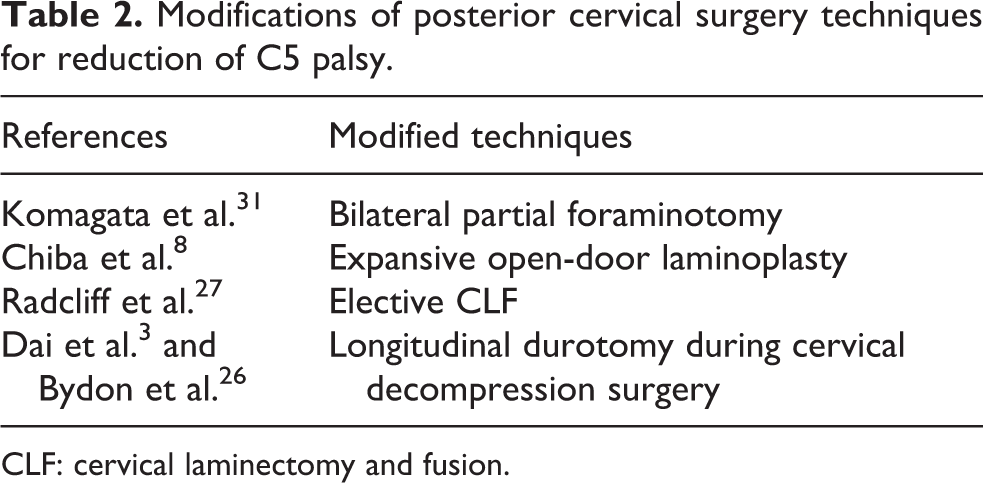
CLF: cervical laminectomy and fusion.
Previous studies have shown that conservative therapy methods, such as rest, muscle strength rehabilitation, range of motion exercises in bed, hyperbaric oxygenation, and low-frequency sound waves, are usually successful in treating C5 palsy. 11,17,19,21,23 However, some cases require additional surgery such as foraminotomy to achieve better results. 7,8,29,30,35 Considering these cases, there might not be a single reliable treatment for postoperative C5 palsy because of its multifocal pathology.
Patients who developed C5 palsy generally had good recovery from neurological and functional deficits. Our review found that the full recovery time ranged from 48 h to 41 months. However, not every patient who experienced C5 palsy recovered from the deficit; irreversible cases of C5 palsy were also reported, especially in the severely paralyzed cases (MMT ≤ 2). Greiner-Perth et al. reported two cases of only partial recovery in 10 patients with C5 palsy, with duration of complete recovery related to the degree of motor impairment. 41 Severely paralyzed cases (MMT ≤ 2) required significantly longer recovery periods than mildly paralyzed cases, especially in patients with OPLL and patients experiencing persistent muscle weakness. 3,34 Residual deficits were defined as failure to return to full motor strength in either the deltoid or biceps brachii, sensory deficit in the C5 distribution, or increased pain in the C5 distribution compared to preoperative status. 22
C5 palsy has been reported mainly after posterior cervical surgery, but can also be seen after surgery using the anterior approach. Kim et al. reported that 6 of 134 patients suffered from C5 palsy after anterior cervical discectomy fusion, and 2 patients with C5 palsy had significant weakness of the deltoid muscle (MMT grade 1) 11 ; the authors conducted foraminotomy on these two patients and only one showed full recovery. Hashimoto et al. also reported that 17 of 199 patients who underwent anterior decompression surgery and spinal fusion suffered from C5 palsy. 12 Thus, surgeons should also consider the possibility of postoperative C5 palsy occurrence when conducting anterior cervical surgery.
Two previous systematic reviews have been conducted regarding C5 palsy. Sakaura et al. from Osaka University mainly focused on the mechanism of C5 palsy, 13 whereas the review published by Gu et al. from Changzheng Hospital concentrated on its risk factors. 14 In contrast, our systematic review is a complete review of C5 palsy that includes discussion of its clinical features, risk factors, mechanism, and preventive measures. Owing to methodological shortcomings in studies included in this systematic review, the results from different studies may vary because of differences in study design, evaluation criteria, sample size, and incidence or severity of C5 palsy.
Conclusion
The result of this systematic review suggests that patients with older age, male gender, preexisting intervertebral foraminal stenosis, and/or OPLL are at high risk for postoperative C5 palsy. Risk reduction options should be considered for such patients. Further study is needed to clarify the etiology and pathological mechanisms underlying C5 palsy after laminoplasty, and consequently to establish effective measures for prevention of this serious complication.
Footnotes
Authors’ Note
No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by The National Natural Science Foundation of China (81201418, 81572181).