
Abstract
Study Design
Retrospective cohort study.
Objective
To compare patterns in opioid usage and prescriptions between patients who undergo cervical laminectomy with instrumented fusion (LF) vs cervical laminoplasty with reconstruction (LP) within single surgeon and national database cohorts.
Methods
We identified patients with cervical myelopathy undergoing primary LF or LP in both a single-surgeon series cohort (2004-2018) and a nationally representative cohort drawn from the IBM® Marketscan® database (2014-2016). We recorded opioid usage within 6 months of surgery and identified differences in unadjusted opioid use rates between LF and LP patients. Multivariable logistic regression was used to evaluate the association between procedure type and postoperative opioid use.
Results
Without adjusting for covariates, LF patients had a higher rate of 6-month opioid use in the single-surgeon cohort (15.7% vs 5.1%, P = .02). After adjusting for covariates, LF patients had higher odds of 6-month postoperative opioid use (OR 2.8 [95% CI 1.0-7.7], P = .04). In the national cohort, without adjusting for covariates, there was no significant difference in 6-month opioid use between LF and LP patients. Even after adjusting for covariates, we found no significant difference in odds.
Conclusions
Findings from a single-surgeon cohort reveal that LF is associated with a higher rate of 6-month opioid use than LP. This is at odds with findings from a national database cohort, which suggested that LP and LF patients have similar rates of opioid usage at 6-months postoperatively. To prevent overuse of narcotics, surgeons must consider the distinct pain requirements associated with different procedures even in treatment of the same condition.
Introduction
Degenerative cervical myelopathy (DCM), previously known as cervical spondylotic myelopathy (CSM), is a very common cause of chronic neck pain and neurologic dysfunction, with an estimated incidence of 41 per million and prevalence of 605 per million in North America. The most common treatment for moderate to severe multilevel DCM is spinal decompression with cervical laminectomy and fusion (LF), which has generally been associated with positive pain relief outcomes. 1 However, some patients who undergo LF may experience persistent axial pain for several years following surgery, akin to the “post-laminectomy” syndrome that is sometimes observed following lumbar spine procedures.2,3 Pain control after cervical spine surgery is often achieved using a multimodal regimen which includes opioid-containing medications. However, long-term narcotic use has been associated with increased risk of dependence, addiction, and overdose. In addition, overprescription of opioids creates an economic burden for the healthcare system and also the potential for illicit use of the drugs amongst other individuals.4-6 Consequently, efforts amongst spine surgeons have already begun to curtail opioid prescription rates through increased usage of non-opioid alternatives (ex. acetaminophen, NSAIDs) and the introduction of new surgical techniques that reduce tissue insult and subsequent pain.
Cervical laminoplasty with reconstruction (LP), developed in Japan in the 1970s, has become an increasingly popular alternative to LF among American spine surgeons. Despite being a more technically demanding procedure, LP has comparable outcomes to LF 7 while also resulting in less restriction of motion, stiffness and postoperative pain compared to LF.8-10 Considering the relative decrease in tissue trauma during LP, we believe that LP may result in a reduced necessity for postoperative opioids. However, no clinical studies to date have compared rates of postoperative opioid usage or patterns of opioid prescription between LP and LF patients.
The purpose of this study was to compare opioid medication use and opioid prescription patterns between DCM patients undergoing cervical LP and LF. The specific aims were to (1) compare rates of opioid use at 6 months postoperative between LP and LF patients in a single-surgeon cohort, (2) compare how frequently patients undergoing each procedure received a 6-month supply of opioid medications vs a more than 6-month supply of opioids in a nationally-representative multicenter cohort, and (3) compare patterns in opioid prescribing between the single surgeon and national database patient cohorts.
Methods
Study Design and Cohort Selection
The study was designed as a retrospective analysis of 2 separate data sets: a single-surgeon cohort and a cohort drawn from a national inpatient database. This was intended to leverage the unique advantages of both data sets, in that the single-surgeon series would contain spine surgery-specific data that could only be obtained by reviewing the records of individual patients whereas the national inpatient sample would allow for comparison of our institutional results to national trends despite lacking spine surgery-specific data.
The single-surgeon opioid use cohort was selected through a retrospective chart review of patients diagnosed with multilevel (3-5 levels) DCM who underwent cervical LF or LP by a single surgeon at our center (Mount Sinai Hospital, New York, NY) from 2004 to 2018. Institutional review board (IRB) approval was obtained prior to commencing chart review and a waiver of informed consent was granted (IRB approval number 00006145). Included patients were at least 18 years old, had a diagnosis of multilevel DCM with or without radiculopathy, and received treatment with primary LP or LF with or without concomitant C2 dome laminectomy or foraminotomy (1 or more levels, unilateral or bilateral). Patients were excluded if their surgery was a revision, performed via an anterior approach, or was a cervical decompression procedure other than LF or LP (ex. laminectomy without fusion, laminotomy, discectomy).
The nationally-representative opioid prescription cohort was selected using the IBM MarketScan Commercial Claims and Encounters database to identify patients who underwent cervical LP or LF from 2013 to 2017. The database collects medication prescription data for over 203 million individuals in the U.S. covered by employer-sponsored private health insurance each year. LP patients were identified in the database using CPT codes 63 050 and 63 051. LF patients were identified using CPT codes 63 001, 63 015, and 63 045 for laminectomy along with 22 600 or 22 614 for a concomitant spinal fusion. Inclusion and exclusion criteria as outlined above were also used for the national cohort.
For both cohorts, we recorded demographic and perioperative variables including, but not limited to: age at time of surgery, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status, and comorbidities. Since preoperative opioid use is a known risk factor for long-term postoperative opioid use, this variable was recorded in both cohorts. 11 For the single-surgeon cohort, preoperative opioid use was defined as any use of opioid pain medication in the 1 month prior to surgery. For the national cohort, preoperative opioid use was defined as receiving a prescription for at least 120 pills or filling 10 or more prescriptions for opioids 1 year prior to surgery.
Outcomes Measured
We considered “opioid pain medications” to include both pure opioids (ex. oxycodone, tramadol) and combination medications containing both an opioid and acetaminophen (ex. oxycodone-acetaminophen). For the single-surgeon cohort, the primary outcome measured was the use of 1 or more opioid pain medications at 6 months after surgery, as determined using 6-month follow-up notes obtained from the EMR. For the national cohort, we measured 2 primary outcomes: prescription of a 6-month supply of opioid medications and prescription of opioids past 6 months postoperative.
Statistical Analysis
All statistical analyses were performed in SAS version 9.4 (SAS Institute, Cary, NC). Within each cohort, demographic characteristics were compared between LP and LF patients using two-sample Student’s t-test for continuous variables and chi-squared test or Fisher’s exact test for categorical variables. Demographic characteristics were also compared between the single-surgeon and national inpatient cohorts using the same analyses. Multivariable logistic regression was used to determine if procedure type (LF or LP) was an independent predictor of opioid-related outcomes, with LF patients acting as the control group. Co-predictors for the regression model were selected based on characteristics that differed significantly between the LF and LP groups as well as known predictors of postoperative opioid use reported in the literature. All P-values <.05 were considered significant.
Result
Opioid Use in Single-Surgeon Cohort
Characteristics of a Single-Surgeon Cohort (n = 264) of Degenerative Cervical Myelopathy (DCM) Patients Who Underwent Cervical Laminectomy with Fusion (LF) or Cervical Laminoplasty with Reconstruction (LP). Means are Reported with Standard Deviations.
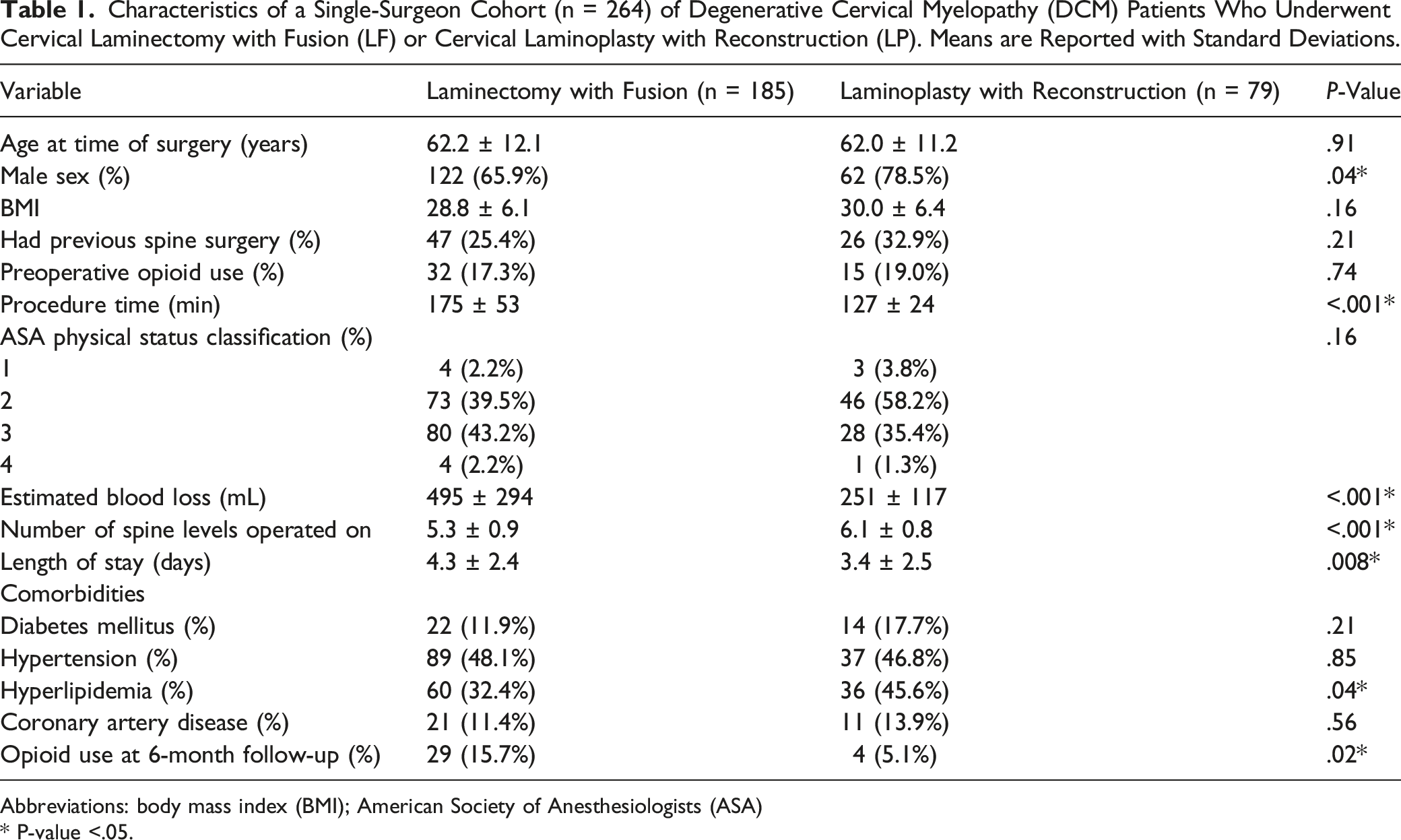
Abbreviations: body mass index (BMI); American Society of Anesthesiologists (ASA)
* P-value <.05.
Without adjusting for covariates, there was a significantly higher rate of opioid use at 6 months postoperative in the LF group compared to the LP group (15.7% vs 5.1%; P = .02). However, there were also differences between the 2 groups in the following characteristics: sex (P = .04), procedure time (P < .001), estimated blood loss (P < .001), number of spine levels operated on (P < .001), length of stay (P = .008) and comorbid hyperlipidemia (P = .04). There was no significant difference in preoperative opioid use between the 2 groups (P = .74). Multivariable analysis with age, sex, preoperative opioid use, estimated blood loss, procedure time, number of spine levels operated on, length of stay, and hyperlipidemia as co-predictors found that procedure type was a significant predictor of 6-month opioid use (P = .04) with LP patients having .36 times lower odds of opioid use compared to LF patients as controls (95% CI .13 – 1.00).
Opioid Prescriptions in National Cohort
Characteristics of the IBM MarketScan Database National Cohort (n = 1816) of Degenerative Cervical Myelopathy (DCM) Patients Who Underwent Cervical Laminectomy with Fusion (LF) or Cervical Laminoplasty with Reconstruction (LP). Means are Reported with Standard Deviations.
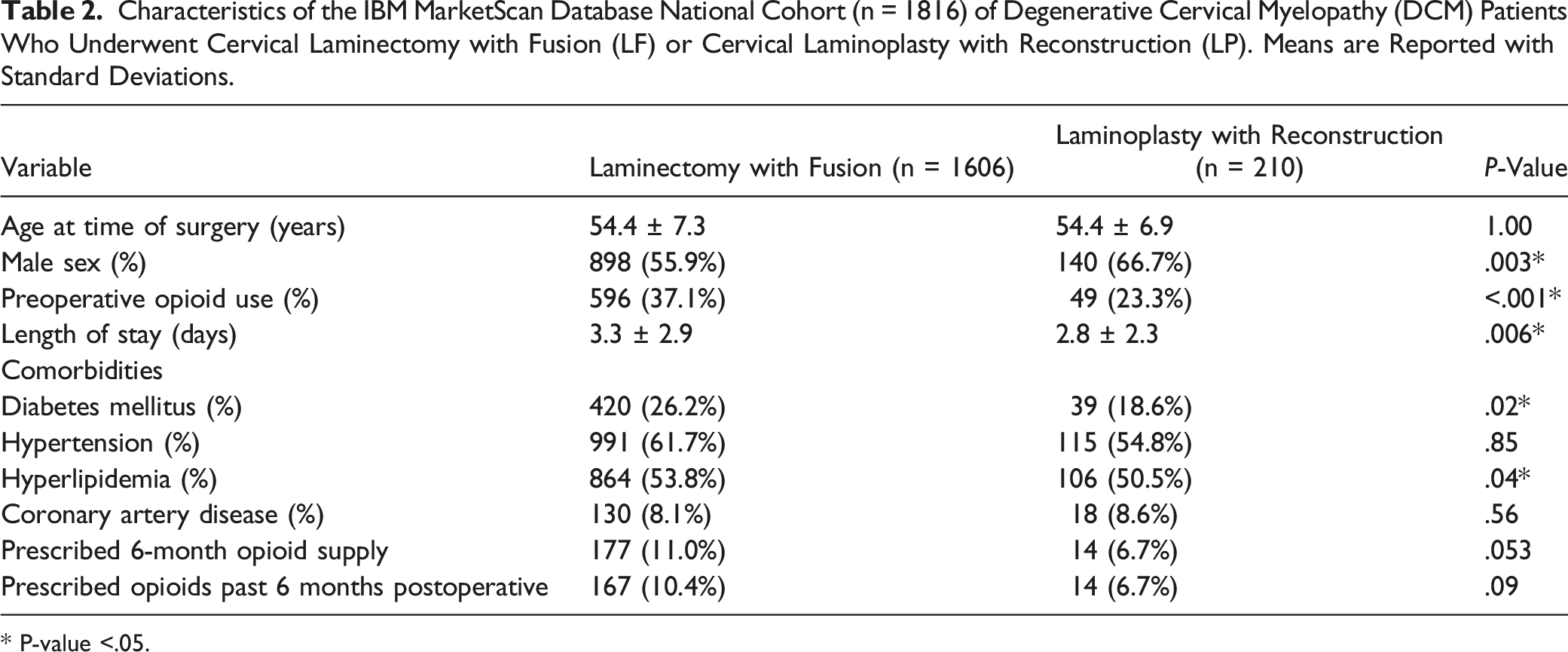
* P-value <.05.
There were no significant differences between the rate of prescription of a 6-month supply of opioids (P = .053) or rate of prescription of more than 6 months of opioids (P = .09) between LF and LP patients. However, there were differences between LF and LP patients in the following characteristics: sex (P = .003), prior opioid use (P < .001), length of stay (P = .006), comorbid diabetes (P = .02), and comorbid hyperlipidemia (P = .04). Multivariable analysis with age, sex, comorbidities, and prior opioid use as co-predictors found that procedure type was not a significant predictor of prescription of a 6-month opioid supply (P = .10) with LP patients having similar odds to LF patients as controls (OR 1.61, 95% CI .91 – 2.85). The same analysis also found that procedure type was not a significant predictor of opioid prescription past 6 months (P = .10) with similar odds between LP patients and LF controls (OR 1.50, 95% CI .84 – 2.65).
Comparison of Single-Surgeon and National Inpatient Cohorts
Characteristics of Cervical Laminectomy with Fusion (LF) Patients from the Single-Surgeon Cohort vs the IBM MarketScan Database National Cohort.
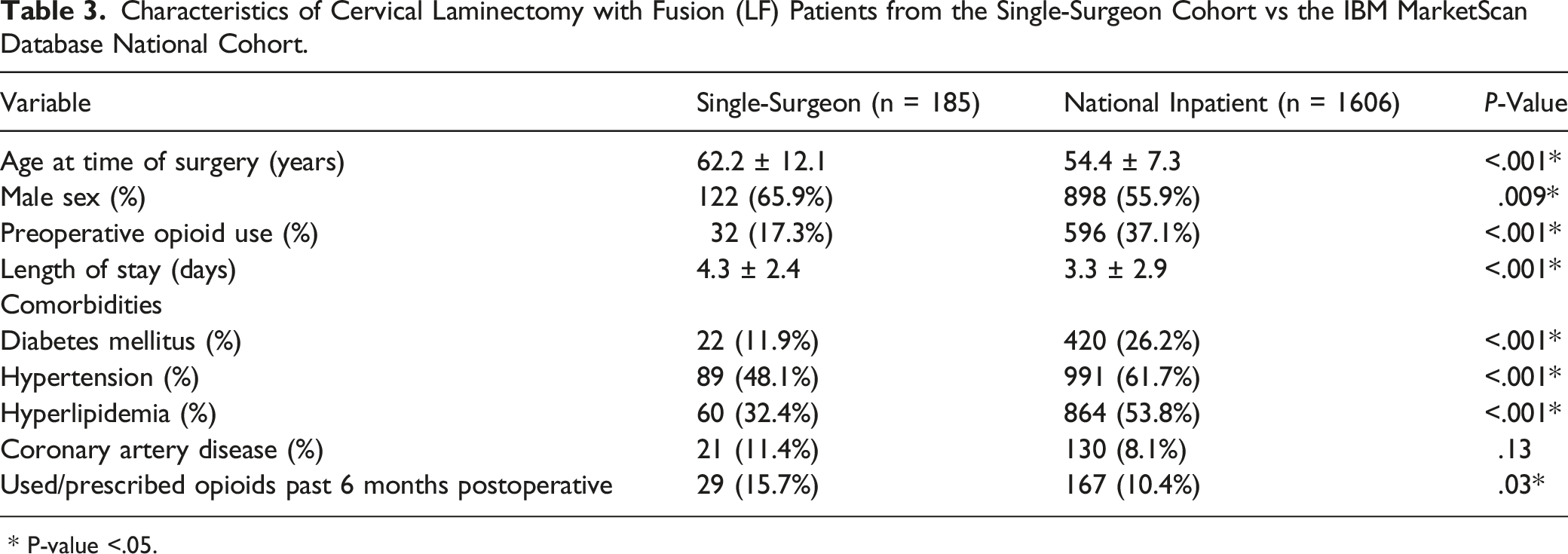
* P-value <.05.
Characteristics of Cervical Laminoplasty with Reconstruction (LP) Patients from the Single-Surgeon Cohort vs the IBM MarketScan Database National Cohort.
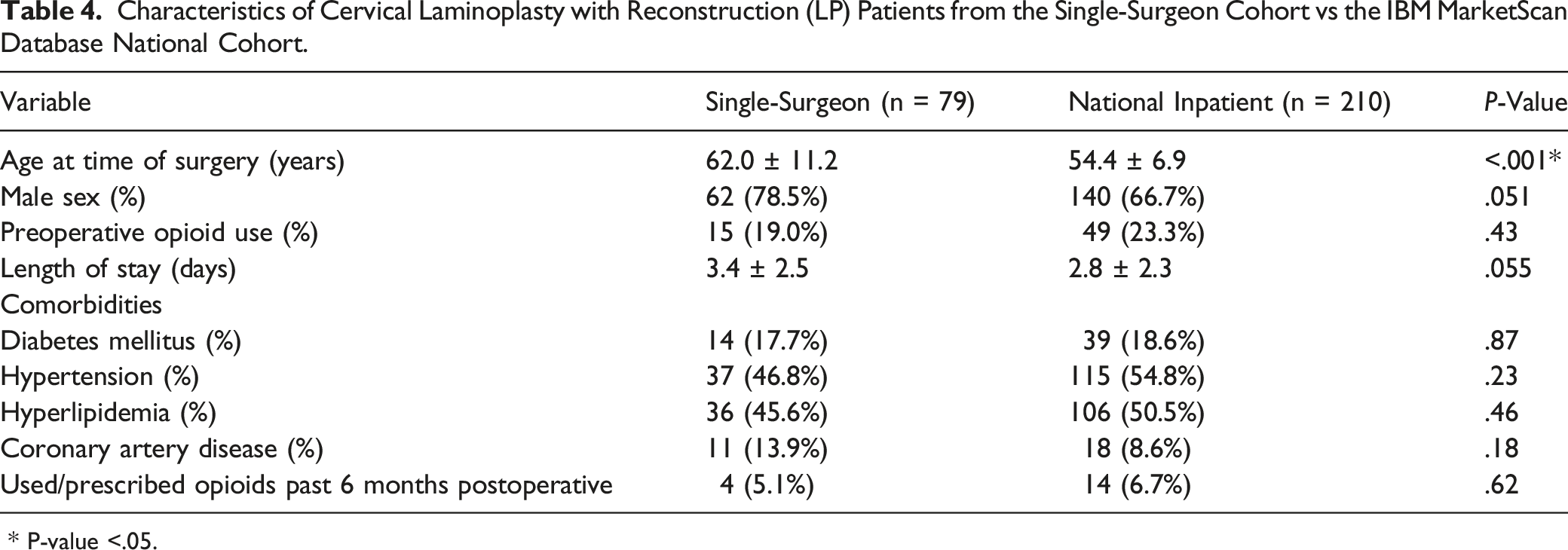
* P-value <.05.
Fewer differences were observed between the single-surgeon and national LP cohorts. LP patients in the national cohort were significantly younger than those in the single-surgeon cohort (P < .001). The national LP cohort also had a lower percentage of males, but this difference did not reach statistical significance (P = .051). Unlike the LF cohorts, there was no significant difference between LP patients in the single-surgeon vs national cohorts in the rate of opioid use/prescription past 6 months postoperative (5.1% vs 6.7%; P = .62).
Discussion
While LP and LF patients from a national inpatient cohort had similar opioid requirements after surgery, cervical LP was associated with significantly lower odds of using opioid pain medication at 6 months postoperative compared to LF in a single-surgeon cohort of patients. However, while demographic characteristics were generally similar between LP patients in both cohorts, there were significant differences in age, sex, preoperative opioid use, and other characteristics between LF patients in the single-surgeon cohort vs the national cohort.
While our single-surgeon analysis found a significantly lower rate of 6-month postoperative opioid use among LP patients vs LF patients, it is difficult to verify this finding against the existing spine literature since few studies have directly compared opioid use rates between the 2 procedures. However, several prior studies have compared postoperative pain severity and duration between LP and LF and also commented on opioid medication use. For example, Kaminsky et al. (2004) performed a matched-cohort analysis that found that LP patients experienced greater pre-to-postoperative improvement in analog scale-reported pain at 5-year average follow-up than LF patients (57% vs 8%, P = .0036). 9 Similar to our findings, Kaminsky et al. noted that at latest follow-up there was no opioid pain medication use in the LP cohort whereas 18% of the LF cohort was taking opioids. 9 Manzano et al. (2012) conducted a prospective randomized trial comparing LP to LF for multilevel DCM and found that LP patients showed statistically-significant improvement in Nurick grade and self-reported neck, interscapular, and arm pain at 1-year follow-up (P < .05) whereas LF patients did not. 12 Unlike our analysis, Manzano et al. reported no difference in opioid use between the groups but did not specify the time point at which opioid use was assessed. 12 With regard to differences in opioid use during the immediate postoperative period, Hardman et al. (2010) conducted a retrospective cohort study that found that fewer LP patients than LF patients needed intravenous opioids more than 48 hours after surgery, though this difference did not reach statistical significance (47% vs 63%, P = .17). 10 While much of the available evidence suggests that LP patients have a lower need for opioid pain medications during the postoperative period compared to their LF counterparts, this has not been borne out in all studies. Heller et al. (2001) performed a matched-cohort study comparing LP to LF patients, and although the study was limited to 13 patients in each cohort, the group found that only 1 patient in each cohort was using opioid medication at average 2-year follow-up. 13 Furthermore, it should be noted that the available studies comparing opioid use between LP and LF are limited in their conclusions due to small sample size (<100 patients) and variability in follow-up time.
Our analysis of the IBM MarketScan database found no significant difference in 6-month postoperative opioid prescription patterns between LP and LF patients. Our study defined prolonged prescription patterns in 2 different ways: as prescription of a 6-month supply of opioid medications and as prescription of opioids past 6 months postoperative. Prior retrospective studies in the spine literature have also used this database to assess national patterns of opioid prescription and use, but their definitions of long-term opioid use and/or prescription have differed from our own. Harris et al. (2020), who studied opioid prescribing patterns among adolescent idiopathic scoliosis patients who underwent posterior spinal fusion, used a criterion of ≥90 morphine milligram equivalents daily to identify patients at risk of opioid dependence per Centers for Disease Control and Prevention guidelines. 14 Another definition of prolonged opioid use came from Kowalski et al. (2021), who set a threshold of opioid use after 6 weeks postoperative and also excluded opioid use up to 1 month after surgery to avoid misclassifying standard postoperative opioid prescriptions as “prolonged use” in their analysis. 15 Using this definition, the authors assessed opioid use at different postoperative time intervals (6 weeks - 3 months, 3-6 months, 6-12 months, >1 year) and found that pre-operative narcotic use and several comorbidities (ex. tobacco use, mental health diagnosis) were associated with prolonged opioid use. 15 Jain et al. (2021), who studied the effects of preoperative opioid use on chronic opioid use following single level lumbar discectomy, defined “chronic opioid use” as receiving >6 opioid prescriptions/refills between 3 months and 1 year after the index procedure. 16 This definition of chronic opioid use is somewhat similar to our own definitions of prolonged opioid prescription, albeit with a specific postoperative interval (3 months - 1 years) instead of a cutoff time point (6 months). Other national datasets have also been utilized in the cervical spine surgery literature. For example, Pugely et al. (2018) conducted a retrospective analysis of the Humana Inc. claims dataset that found that preoperative opioid use was a major predictor of opioid use at 1 year following anterior cervical fusion. 17
In the present study, we found a significant discrepancy between the true opioid use rates following LF and LP procedures in our single surgeon cohort and national opioid prescription patterns associated with both surgeries. While our single-surgeon cohort analysis suggests that LP patients have a significantly lower rate of opioid medication use at 6-month follow-up compared to LF patients, our national cohort analysis suggests that both groups receive 6-month refills at a similar rate. This raises concern that surgeons may be overprescribing opioids to their LP patients even though they potentially have lower pain requirements than their LF counterparts. We posit that given the relative novelty of LP as a treatment for cervical myelopathy, surgeons likely have not adjusted pain protocols to account for the reduced postoperative pain and tissue trauma associated with LP. The LP is a motion preserving procedure with far fewer complaints of stiffness and pain. Therefore, surgeons should consider tailoring opioid prescription plans for specific cervical spine procedures in order to adequately control patients’ pain while also minimizing the risk of chronic opioid use, overdose, and medication diversion.18-22 Surgeons should also seek out alternative modalities for postoperative pain management including NSAIDs and acetaminophen, which may augment or even replace opioids in the acute phase of recovery. 23
We caveat these findings by noting that there were also significant differences in baseline demographics between LF patients in the single-surgeon and national cohorts, especially the rate of preoperative opioid use. LF patients in the national cohort had a higher rate of preoperative opioid use yet a lower rate of prescription past 6 months postoperative, while LF patients in the single-surgeon cohort had a lower rate of preoperative opioid use but a higher rate of use past 6 months postoperative. This raises the possibility that while LP patients at our institution may be prescribed opioids for a shorter duration than is observed at the national level, LF patients at our institution may be receiving opioids for a longer duration than the national average, thus leading to the observed difference in postoperative use rates in our single-surgeon analysis.
We acknowledge several limitations to our study. First, the retrospective design of the single-surgeon cohort and national-cohort analyses introduced selection bias into our results. Patients were not randomized to LF vs LP treatment in either cohort and thus surgeon preference for either procedure may impact the observed results. This may be particularly important if surgeons use different indications for LF and LP procedures. Second, different co-predictors were included in the multivariable regression models for the single-surgeon cohort vs the national inpatient cohort. This is due to the fact that certain variables specific to spine procedures (ex. BMI at time of surgery, spine levels operated) could be easily abstracted from individual patient records in the single-surgeon cohort, whereas the IBM MarketScan database is not a surgery-specific dataset and does not have comparable granularity. Third, the specific surgical techniques used for LP and LF procedures may differ between the single-surgeon cohort and national inpatient cohort. Differences in training, equipment used, and surgeon experience can affect LP and LF procedures and consequently the potential for postoperative pain.
Conclusion
The use of cervical laminoplasty with reconstruction for treatment of DCM was found to be predictive of lower odds of opioid use at 6 months postoperative compared to cervical laminectomy with fusion, which implies that patients undergoing LP may experience less postoperative pain and use opioid pain medication for a shorter period of time than their counterparts. However, national inpatient data suggests that LP and LF patients are prescribed opioids past 6 months postoperative at similar rates. These findings raise concern that opioids may be overprescribed among LP patients compared to their LF counterparts. Postoperative pain management should be tailored differently for different cervical decompression procedures in order to adequately control patients’ pain while minimizing the risk of opioid abuse.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.