
Abstract
Object:
To investigate the efficacy of debridement, open drainage, and early feeding to treat early esophageal fistula complicated with anterior cervical surgery.
Methods:
Retrospective analysis was conducted on data from 3154 patients who had undergone anterior cervical surgeries for cervical vertebra diseases between January 2006 and January 2013, in which eight patients had esophageal fistula with five males and three females. Four patients had cervical spinal injuries and four patients had cervical spondylosis. All of whom had postoperative esophageal fistulas and underwent debridement and drainage. The wounds were left open for natural drainage. No drainage devices were placed in surgical sites, and no gastric tubes were placed after surgeries. Such normal food as rice balls but not liquid or semiliquid diet was recommended. Local pressurization was conducted with fists during feeding to prevent food overflowing from orificium fistulae.
Results:
Healed esophageal fistulas were achieved in all of the patients after 1–2 weeks treatment. There weren’t recurrent esophageal fistulas and delayed infection found during 2–5 years follow-up. Good swallowing functions and stable cervical vertebrae were achieved in all of the patients. The satisfactory therapeutic effects were achieved in patients with previous neck diseases. Frankel classifications were increased by 1–2 grades in patients with cervical spinal injuries. JOA scores were increased from 9.5 before surgery to 15.5 after surgery in patients with cervical vertebra diseases.
Conclusions:
Early postoperative esophageal fistula complication after anterior cervical surgery can successfully be treated by debridement, drainage without gastric tube, and with early oral postoperative feeding but without fluids.
Introduction
Anterior cervical decompression, bone graft fusion, and internal fixation are the common surgical methods to treat cervical spine injuries and cervical spondylosis, of which postoperative esophageal fistula is one of the rare but serious complications with 0.04–0.25% of incidence and 9–45% of mortality. 1 –3 Esophageal fistula can cause incision infection, osteomyelitis, and even intraspinal canal infection in severe patients, in whom esophageal secretions and food debris will accumulate in surgical sites and flow downward and outward along areolar connective tissues, resulting in mediastinal and pulmonary infection. Late sequelae may occur, such as strictures and diverticula after perforation. 4 –6 Therefore, early diagnosis and timely treatment are of important significance for the whole treatment of this disease. At present, there are conservative treatment, simple fistula repair, and complex tissue reconstruction for the treatment of esophageal fistula. 7 –10 Successful management of perforations depends on prompt recognition of the symptoms and immediate institution of therapy. In both conservative treatment and surgical treatment, these authors have emphasized the importance of fasting without exception. Is fasting necessary for long time? We employed debridement, drainage, and early feeding to treat eight patients with esophageal fistula after anterior cervical surgeries between January 2006 and January 2013. Our different experiences were summarized as follows.
Materials and methods
General data
Retrospective analysis was conducted on data from 3154 patients who had undergone anterior cervical surgeries between January 2006 and January 2013, in which eight patients had esophageal fistula with five males and three females; age 24- to 50-years old, average 39.5-years old. All of the eight patients had esophageal fistula at 5–10 days (average 7 days) after surgeries, in which one patient was transferred to our hospital due to esophageal fistula found at 10 days after anterior cervical surgery in another hospital. Four patients had cervical fractures and four patients had cervical spondylosis. Regarding spondylosis, index diagnosis is as follows: in cases of severe neck or arm pain that does not get better with treatment; there is weakness or numbness in the arms or hands; the reflexes are reduced; the MRI features of spinal canal are narrowed and spinal cord is compressed. In the eight patients, three patient underwent cervical discectomy, bone graft fusion, and internal fixation with titanium plate; five patients underwent corpectomy, bone graft fusion, and internal fixation with titanium plate (Table 1).
General information of all patients.

ACCF: anterior cervical corpectomy with fusion; ACDF: anterior cervical discectomy with fusion; Y: yes; N: no.
aCase comes from another hospital.
Diagnosis of esophageal fistula
Pharyngalgia, fever, wound redness, and swelling appear at 5–10 days after anterior cervical surgery, and food debris or overflowed liquids are found in the wounds after feeding in some patients (Table 1). All of the eight patients in this group had some or all of the abovementioned clinical symptoms, six of whom had food debris or overflowed liquids in the wounds after feeding (Table 1). One patient with C5 fracture underwent anterior cervical C5 subtotal vertebrectomy and plate fixation with titanium mesh and autogenous bone particles in another hospital, who had redness and swelling in posterior neck skin incision, significant pain, fever, 39°C of body temperature, yellow purulent secretions around the incision, and wound disruption occurred at 7 days after surgery. It was considered as incision infection at first but the wound was not healed 2 months after debridement and catheter drainage under general anesthesia. At last, it was diagnosed as complicated esophageal fistula by esophagography, so exploration was performed by debridement and removal of internal fixation, and no sinus was found during the surgery. In this operation, ilium grafting and halo vest external fixation were conducted. The drainage tube was placed in the surgical site. The sinus opening was not healed after fasting, nasal feeding, anti-infection, and nutritional management for 2 months. Therefore, this patient was transferred to our hospital (Figure 1(a) to (d)). Seven patients in our hospital were administered oral methylene blue solution immediately after neck incision disrupted, and blue effusion was shown in the incision. The contrast medium showed limited leak from esophageal fistula in all patients. The disrupted neck incision could be seen in one patient when he was transferred to our hospital from another hospital, who had an approximately 0.8-cm-long orificium fistulae located posterior wall at pharyngoesophageal junction shown in esophagoscopy. All patients were confirmed esophageal fistula in operation.
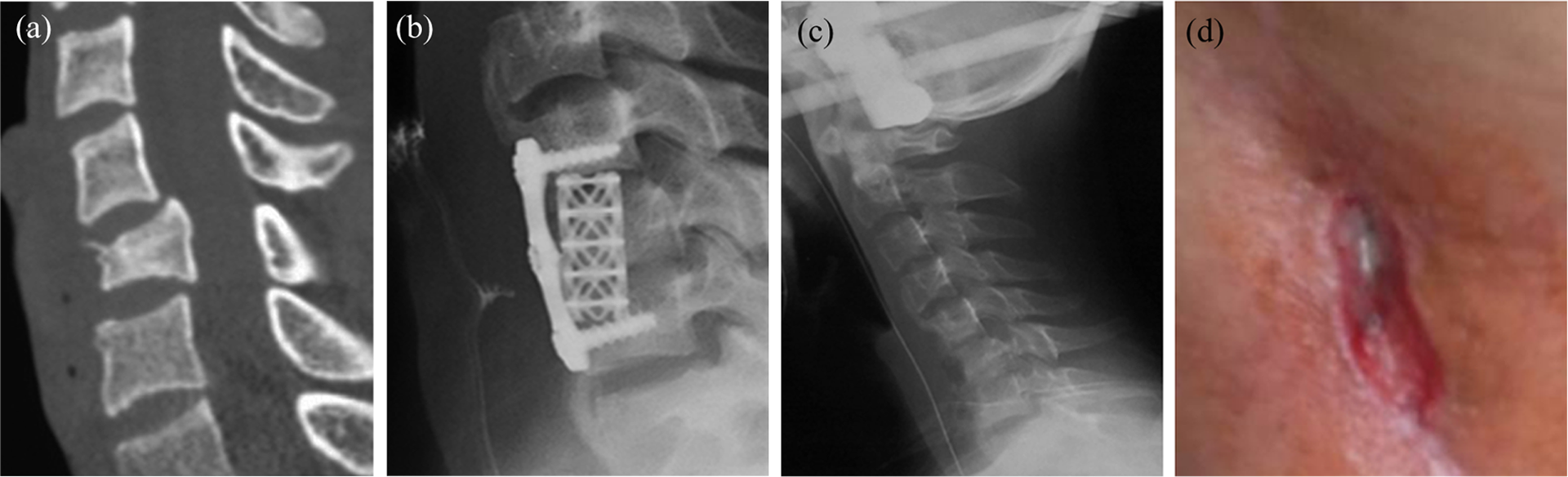
(a) C5 veterbera fracture shown in CT. (b) After C5 veterbera fracture surgery. (c) Removal of internal fixation, halo vest external fixation. (d) Unhealed orificium fistula after removal of internal fixation.
Early debridement treatment for esophageal fistula
Emergent debridements were performed under local anesthesia or general anesthesia referring to experiences in treating esophageal fistulas after cervical esophagus anastomosis from the thoracic surgeons in our hospital (Table 2). All sutures were removed from the incision. Then, adhered soft tissues in the incision were carefully separated and food debris was physically flushed and cleaned to expose cervical plates. Three percent hydrogen peroxide and normal saline were used to repeatedly wash wounds. Some necrotic prevertebral fascia and other soft tissues were eliminated. There are esophageal mucosal edema and valgus around fistulas, about 0.4–0.6 cm length. Don’t trim the esophagus tissue, let esophageal fistula putting-aside. The incisions were opened for natural drainage after debridements were completed. There were not drainage devices placed inside the incisions, and the incisions were covered with sterile dressings.
Treatment information of eight patients in our hospital.

aCase comes from another hospital.
Diet and care after debridement
Referring to experiences in treating esophageal fistulas after cervical esophagus anastomosis from the thoracic surgeons in our hospital, the wounds were left open for drainage; meanwhile, the wound drainage fluid was closely observed. It should be timely replaced if the wet dressings were seen on the wounds. There were no gastric tubes placed after surgery. Such normal foods as rice balls but not liquid or semiliquid diets were recommended for feeding at the second day or third day. Local pressurization was conducted with a fist made by five fingers at wound during feeding to prevent food overflowing from orificium fistulae (Figure 2(a)), and this feeding method was kept for 4 weeks. Antibiotics were used for 7–10 days after surgery to prevent wound infection. Compound amino acids were intravenously administered for 2–3 weeks. No secretions were found in the incisions and inflammations subsided after 10 days–2 weeks, and the wounds healed naturally after 2 weeks. The healed esophageal fistulas were confirmed by esophagography after 4 weeks.

(a) With fist press to close fistula when eating. (b) Healed neck orificium fistula and no recurrence during follow-up. (c) Healed fracture shown in CT for reconstruction during follow-up.
All patients informed and agreed to these treatment.
Results
Esophageal fistulas and neck incisions were well healed in all of the eight patients. The healing time was 10–18 days (Table 2). One patient from another hospital had the longest healing time, and the wound healed 18 days after debridement was performed in our hospital (Figure 2(b) and (c)). All eight patients had a follow-up at 2–5 years postoperatively by a clinical visit with radiography. The neck skin in previous incisions was healed. There weren’t recurrent esophageal fistulas, delayed infections, dysphagia, or neck pains occurred. Results of previous neck diseases were satisfactory in all of the patients, without instability or neurological dysfunction deterioration occurred in any patients. The Frankel classification increased 1–2 grades (Table 3) for all of the patients with cervical spinal injuries, and JOA scores increased from 9.5 before surgeries to 15.5 after surgeries for those patients with cervical spondylosis (Table 4).
Frankel classification of four cases (fracture) of preoperation and postoperation.

JOA of four cases (spondylosis) of preoperation and postoperation.

Discussion
Analysis of esophageal fistula causes
Although there are many causes resulting in esophageal fistula complicated with anterior cervical surgery, they are still unclear. Its anatomical bases are lack of serosas in esophaguses, thinner posterior walls, and poorer blood supply for muscle layers. 5,11 Patients with cervical spinal injuries often suffer from esophageal fistulas mainly because of the compression of veterbera fracture segments as well as traumatic stretching and twisting that could cause esophageal wall injuries, ischemia, and responses to traumas. 3,12 The different retractor types utilized in anterior cervical surgery. The design and handling of these may be of importance to esophagus injury. Esophagus may be stretched or accidently injured during exposure and operation in anterior cervical surgeries, and thus results in esophageal dysfunctions. As esophagus and esophageal walls are thinner, mechanical entrapment will easily result in esophageal ischemic necrosis. If electrotomes were used improperly during anterior cervical surgeries, electric currents can injure esophagus by the conduction of metal hooks, retractors, or other conductors. 5,13 With the improvement of surgical techniques, other factors reported in literature have become uncommon, such as dislodged block bone grafts, surgical devices directly injuring esophagus, compressing on esophagus caused by dislodgements of anterior cervical titanium plates, artificial vertebrae, and other implants. 5,14,15 In this group, no apparent direct injuries were found in esophagus during the whole surgery. No compression on esophagus was found around plates when the incisions were closed at the end of surgeries. Therefore, it was considered that esophageal fistulas are possibly smaller which can’t be found.
Esophageal fistula treatment and postoperative diet
Although some patients with esophageal fistula can be healed by conservative measures including fasting, broad-spectrum antibiotic, and nutritional support, the authors do not agree with only use of conservative measures; this is because in the initial diagnostic consideration for patients with esophageal fistula, we won’t be able to accurately determine whether can meet the requirements of conservative treatment, and conservative treatment itself has failure rate. Twenty percent of patients treated conservatively experienced a bad outcome with the development of an abscess or an osteomyelitis, and the mortality rate is 18%. 16 The role of delayed diagnosis and treatment as bad factors regarding prognosis. If the infection hasn’t been found and controlled in time, it will be downward and outward along areolar connective tissues, resulting in mediastinal and pulmonary infection. As soon as possible to prevent infection downward, open drainage is necessary to give priority to the intervention measures.
Without a doubt, the size of fistula and the extent of damage of esophagus are important factors for choice of treatment. In this report, since esophageal fistula is smaller, and discovery and treatment is in time, local infection has been easily controlled, and debridement surgery obtained satisfactory effect. Current treatment for esophageal fistula is as follows: (1) for esophageal injuries found during surgeries, invite respirologists to held a consultation and perform esophageal repair. 7 Primary closure has been successful in select cases. However, high rates of recurrence led to the development of reinforced primary repairs with vascularized tissue flaps incorporated into the reconstruction 16 –18 ; (2) for esophageal fistulas found at postoperative, many authors perform esophageal repair with a myriad of flaps such as sternocleidomastoid muscle, pedicled pectoralis major, sternocleidomastoid, free radial forearm, longus colli muscle, and omental flaps. The gastric tubes were placed and nasogastric feeding were applied until the orificium fistulae were healed 10,19 –22 ; (3) for concurrent cervical vertebral osteomyelitis and loosened or dislodged internal cervical fixation, internal fixation devices need to be taken out. 23 All these methods include gastric tube placement, fasting, nasogastric feeding, intravenous nutrition, and other steps in postoperative treatment. It is reported that the healing time is 3–12 weeks. 3,4,9,11,13,14,21 But these methods have some shortcoming such as bigger traumatic and complex operation. Direct suture after debridement may fail because of the local soft-tissue infection, edema. Some authors described cases of failed pectoralis flaps, requiring reoperation. Sometimes, use of the sternocleidomastoid flap puts the spinal accessory nerve at risk during the dissection. 21,24,25 The methods described in this article are from experiences of the thoracic surgeons in our hospital in treating anastomotic fistulas. Compared to the methods reported in literature, the healing time and hospital stays and duration are shorter, and no esophageal repairs required. In the treatment of esophageal fistulas, the importance of nutrition therapy has also been mentioned in many literatures. 22,26,27 Nasal feeding cannot meet nutritional requirement for wound healing, while gastric tube placement may stimulate locally orificium fistulae, inimical to wound healing. Some authors 28,29 recommended to use jejunostomy or gastrostomy so as to avoid long-term placement of nasogastric tubes injuring mucous membranes but this method has a poorer patient compliance. For patients undergoing more drainage, compound amino acids can be administered intravenously when necessary to prevent negative nitrogen balance, which is favorable to wound healing. So, sufficient drainage and good nutritional support are the keys to success.
Experiences of success in this group of patients
The authors gain experiences: to ensure sufficient nutrition and avoid orificium fistulae stimulation are important conditions for esophageal fistulas to heal sooner. If no significant esophageal injuries are found before incisions were closed in the surgeries, it may be smaller postoperative esophageal orificium fistulas formed. Due to no significant esophageal defects present, good healing can be achieved and no esophageal repairs or other more invasive surgeries are required by employing this method. Additionally, nasal feeding provides poorer nutrients and stimulates esophaguses; it is inimical to orificium fistula healing compared to oral feeding. Such normal foods as rice balls but not liquid diet are recommended to prevent food debris stimulating sinus openings. Pressurization should be applied with hands during feeding to prevent food overflowing out of sinus openings. Our technique uses less invasive operation mode and anesthetic mode to treat these complications, providing smaller traumas in patients and higher patient compliance.
Shortcomings of this study
All of the patients in this group were at the early postoperative stage. However, we have not gained experiences for patients with esophageal fistulas resulted from internal fixation at late stage yet. Additionally, not all of the patients have undergone routine esophagoscopy in this group, so, the sizes of their esophageal fistulas have not been defined at preoperation.
Footnotes
Author Contribution
Haifeng Yuan and Huiqiang Ding contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by The National Natural Science Funds of China (no. 81160220), Ningxia Natural Science Funds (no. NZ11197), and China Scholarship Council Funds (no. 201208645084).