
Abstract
Purpose:
To introduce the intraoperative O-arm-assisted pedicle screw insertion without any navigation system in the treatment of thoracic vertebrae fracture and compare it to conventional fluoroscopy (C-arm)-assisted pedicle screw insertion technique.
Methods:
About 156 pedicle screws were inserted in 23 patients (C-arm group), and 208 pedicle screws were inserted in 30 patients (O-arm group). The postoperative computed tomography images were analyzed for pedicle violation based on Gertzbein classification. The total surgery time, the average time required for inserting a screw, the mean action times of adjusting guide probe and pedicle screw, and the hospitalization time were compared in both groups, respectively. The American Spinal Injury Association (ASIA) was used for evaluating the health outcomes pre- and postoperatively.
Results:
There are the higher accuracy rate of satisfactory pedicle screw placement (grades 0 and 1) and the less incidence of medial perforation in the O-arm group compared to the C-arm group (p < 0.05). The average time required for inserting a screw, the action times of adjusting the guide probe and pedicle screw, and the hospitalization time in the O-arm group are less than the respective ones in the C-arm group (p < 0.05). There was no significant difference for the total surgery time between both groups. No further damage of the nerve function postoperatively is found according to the ASIA grade.
Conclusion:
The O-arm-assisted pedicle screw insertion without navigation we described provides higher accuracy of pedicle screw placement and better clinical efficacy compared to conventional fluoroscopy (C-arm) technique.
Keywords
Introduction
Pedicle screws have become a common applied treatment in spine surgery resulting from the instrumentation constructs with high biomechanical strength offered by three-column fixation. However, inserting thoracic pedicle screws is more technically challenging than placing lumbar ones. The diameters of thoracic pedicles are so smaller (compared with lumbar pedicles) that it is difficult to insert pedicle screws through the narrow trajectory without any breach. 1,2 In addition, the dislocation of the thoracic pedicle screws may increase the incidence of serious complications including injuring nearby vital vessels, the spinal cord, and pleural cavity. 3
The most commonly used image-assisted forms in spine surgery include two-dimensional (2-D) images, in which a fluoroscope or plain radiography is used, and three-dimensional (3-D) navigation, making use of cone-beam computerized tomography (O-arm) or isocentric-C-arm 3D navigation system. 4,5 Conventional pedicle screw placement focused on the anatomical landmarks, entry point, and insertion angle with or without intraoperative 2D imaging can be performed by experienced surgeons. However, in the treatment of thoracic vertebrae fracture, especially upper and middle thoracic vertebrae, 2D imaging can be influenced by the structures of shoulders, scapulas, and ribs, which decreases the accuracy of thoracic pedicle screw placement. 6 Progressively, the 3D system provides intraoperative imaging in axial, coronal, and sagittal planes and tracks the pedicle screw trajectory to match with the anatomic structures, which decreases the perforation rate of pedicle screws.
Since the 1990s, intraoperative navigation techniques have progressed tremendously and reduced the number of misplaced screws significantly, which improved the accuracy of pedicle screw insertion and minimized the risk of neurovascular injuries. 7 The O-arm navigation, one of the latest intraoperative imaging platforms, has been well acknowledged for its superiorities in surgeries for trauma or degenerative spinal diseases. 8 –10 Shin et al. have reported a decrease in pedicle perforation rates from 15% in nonnavigated screws to 6% in navigated pedicle screw insertions. 11 However, the intraoperative navigation pitfalls could eventually cause a loss of operative time, prolonged anesthesia, blood loss, intraoperative pedicle screw errors, and inadvertent neurological complications. 4 Poor planning in the pre- and intraoperative stages will obviate any advantage of an intraoperative navigation system. Moreover, according to the published reports, the accuracy of navigated surgery has not been superior to conventional techniques. 12
Till now, few studies have introduced the intraoperative computed tomography (CT)-assisted (O-arm) insertion of pedicle screws without any navigation system in the treatment of the fracture of thoracic vertebrae. We retrospectively reviewed and analyzed the accuracy and safety between intraoperative O-arm and conventional fluoroscopy (C-arm)-assisted pedicle screw insertion technique.
Materials and methods
Patients
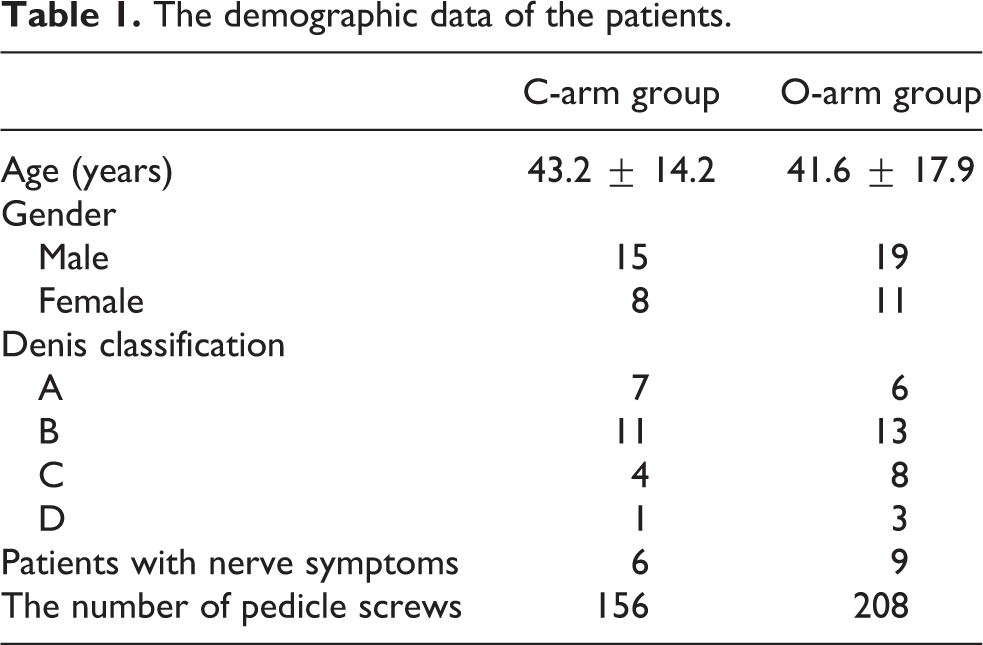
From January 2014 to February 2015, the 53 patients suffering from thoracic spine fractures who accepted thoracic pedicle screw placement (T3–T12) were enrolled in this study. The cases involving cervical or lumbar pedicle screw were excluded from the study. The choice of surgery method (O-arm or C-arm-assisted pedicle screw insertion) was up to patients’ decision without regard to surgeons’ preference. Among the fixation surgeries, 23 cases were under the conventional C-arm (Arcadis Varic mobile C-arm system, Siemens AG, Munich, Germany)-guided method and 30 cases were under the O-arm (SEDECAL, C/Pelaya 9, Pol. Ind., Spain)-guided method. The demographic data are recorded in Table 1. The mean ages were 43.2 ± 14.2 years old (range 21–64 years old) and 41.6 ± 17.9 years old (range 19–61 years old) for the C-arm and O-arm groups, respectively. Six cases in the C-arm group and nine cases in the O-arm group were associated with nerve symptoms. All surgeries were done by two senior surgeons with at least 10 years of operative experience in spinal surgery.
The demographic data of the patients.
The study was approved by the Institutional Ethics Committee, and all patients provided written informed consent for participation.
Surgery
All patients were informed about the usual risks and the rare but serious risks associated with the surgical treatment, including anesthetic hazards, pulmonary embolism, infection, and spinal cord or nerve root injury.
The surgery was performed under general anesthesia, with the patient placed in the prone position, with padding beneath the upper chest and pelvic regions, on a carbon fiber radiolucent table. All the 53 operations were open procedures for open reduction and internal fixation.
The screws were inserted in accordance with the procedure described by Yang et al. 13,14 and Roy-Camille et al. 15 First, identification of the entry point, followed by opening with the awl, and then the blunt end of a 1.5 mm Kirschner wire was tapped by hand for making a guide canal through the pedicle into the vertebral body. If the end of the Kirschner wire touched the pedicle cortices, the Kirschner wire was tapped gently by a hammer to change the direction slightly into the cancellous bone of the pedicle. The guide canal was expanded by a 2.5 mm Kirschner wire then filled by a guide probe. Then, the C-arm (anteroposterior and lateral) or 3-D CT operated by the O-arm was used to check the position of the probe. The 3-D intraoperative images were automatically reformed and visualized on the O-arm imaging screen (see Figure 1). If the probe position was not satisfactory, the direction would be revised and checked again. After the screw with the appropriate length and diameter was inserted, the C-arm (anteroposterior and lateral) or O-arm was used to make sure that the screws were not in the spinal canal.

A male patient, 41 years old, who suffered from T4 fracture without a nerve symptom caused by a car accident, accepted open reduction and internal fixation with O-arm-assisted pedicle screw insertion technique. Preoperative CT (a), intraoperative probe position (b), and pedicle screw position (c) on the O-arm imaging screen, and postoperative CT for T3–T5 (d, e, f) were finished. CT: Computed tomography.
The pedicle screw rod system (Medtronic, CO, USA) was used. According to the level operated, the diameter and length of the screws varied from 4.0 mm to 6.5 mm and from 45 mm to 55 mm, respectively.
Evaluation of clinical results
The operation time was evaluated by the total surgery time and the average time required for inserting a screw, respectively. The average time for inserting a screw = (the total time from puncture at the entry point by awl to complete all screw insertions into pedicle)/the number of pedicle screws. The mean action times of adjusting guide probe and pedicle screw and hospitalization time were recorded in both groups. The nerve function was assessed by the system of the American Spinal Injury Association (ASIA) 16 preoperatively, 1 day, 1 month, and 6 months after the surgery, which is a validated health outcome measure and is widely used in spinal surgery.
Radiographic assessment
Postoperative axial CT images obtained by a Brilliance CT 64-channel scanner (Philips medical systems, PC Best, the Netherlands) of the instrumented segments were used for analyzing screw positions in both groups. Perforation was graded according to the Gertzbein classification 17 : grade 0: screws were completely within the pedicle, grade 1: perforation less than 2 mm, grade 2: perforation between 2 mm and 4 mm, and grade 3: perforation over 4 mm. Additionally, grades 0 and 1 were considered satisfactory, while grades 2 and 3 were regarded as perforation.
Statistical analysis
All data were expressed as mean ± standard deviation. The comparison between the two groups was made by the Mann–Whitney U test. The results were considered significant when the p-value was less than 0.05. All statistics were performed using SPSS 19.0 software.
Result
Clinical result
In the C-arm group, 156 pedicle screws were inserted from T4 to T12 in 23 patients. In the O-arm group, 208 pedicle screws were inserted from T3 to T12 in 30 patients. The two groups were very similar before surgery with respect to the Dennis classification. The total surgery time was 178.6 ± 33.9 min in the C-arm group and 195.7 ± 41.6 min in the O-arm group (p > 0.05). The average time required for inserting a screw was 6.64 ± 3.57 min in the C-arm group and 5.32 ± 2.84 min in the O-arm group (p < 0.05). The action times of adjusting the guide probe and pedicle screw were 4.14 ± 2.36 min in the C-arm group and 2.24 ± 1.36 min in the O-arm group. The hospitalization time was 13.2 ± 3.5 days in the C-arm group and 10.9 ± 2.7 days in the O-arm group (Table 2). Statistical analysis showed that the average time required for inserting a screw and the action times of adjusting the guide probe and pedicle screw in the O-arm group was significantly less than that of the C-arm group and the hospitalization time was shorter in the O-arm group (p < 0.05).
The clinical result and distribution of screws position of the two groups.

Accuracy rate of the pedicle screw placement
Regarding the position of the screw, 114 (73.1%) and 27 (17.3%) screws of the C-arm group were observed as grades 0 and 1, whereas 162 (77.9%) and 39 (18.8%) were observed as grades 0 and 1 in the O-arm group. The distribution of the position of the placed screws in each group is figured out in Table 2. The overall accuracy rate of satisfactory pedicle screw placement (grades 0 and 1) in the O-arm group was 96.6%, significantly higher than 90.4% of the C-arm group (p < 0.05).
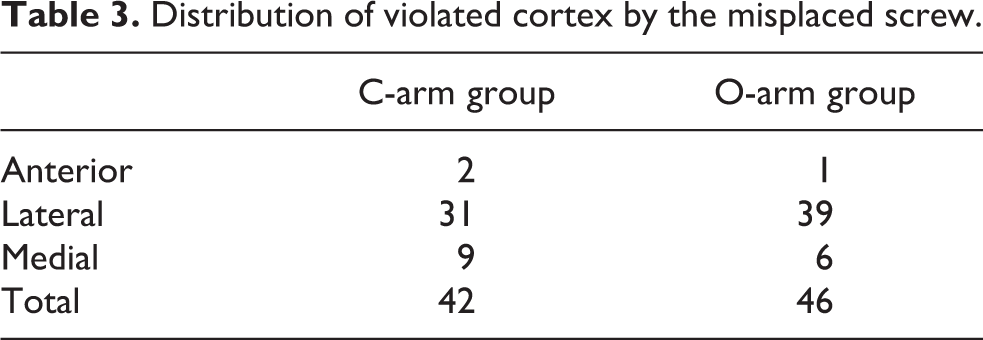
Overall, a significantly higher frequency of lateral perforation (19.2%, 70/364) was observed than medial perforation (4.1%, 15/364). Moreover, the incidence of medial perforation was significantly decreased in the O-arm group compared to that of the C-arm group (2.9% vs. 5.8%, p < 0.05; Table 3).
Distribution of violated cortex by the misplaced screw.
Complications
Six cases in the C-arm group and nine cases in the O-arm group were associated with nerve symptoms. None of the patients without nerve injury got nerve symptoms after the surgery, while the patients associated with nerve symptoms showed no further damage of the nerve function after the operation according to the ASIA grade (Table 4).
ASIA grade of the two groups.

ASIA: American Spinal Injury Association.
Discussion
With the rapid technological advancements, spinal surgery becomes less invasive, higher accuracy, and better efficacy. Pedicle screw fixation can provide stabilized fixation to allow biological healing and correct segmental deformity of the spine, which requires precise placement of screws through narrow bony corridors surrounded by high-risk neural, vascular, and visceral structures. Thoracic screw perforates the cortical margins of the pedicle at a rate ranging from 16% to 54%, leading to the potential for hemorrhage, nerve root injury, or spinal cord injury. 18
Experienced surgeons can insert the thoracic pedicle screws with intraoperative fluoroscopy. However, freehand placement of pedicle screw may be safe in very experienced hands. The quality of fluoroscopic images is significantly reduced by the bony structures of the shoulder and mandible. 6 What’s more, the accuracy rate of screws perfectly located within the pedicle shows 87.7% in the conventional fluoroscopy-guided group. 19
In recent years, various image-guided navigation systems have been introduced and clinically attempted. 20 –23 Compared to traditional fluoroscopy, this new technique has several superiorities such as high quality of multidimensional images and larger field of surgical view. Scheufler et al. reported the accuracy of thoracic (97.8%) pedicle screw placement using CT-based navigation system. 24,25 Shin et al. reported that nearly 92% of the pedicle screws were contained completely within the pedicle using navigation coupled with the O-arm in 124 pedicle screws placed between T9 and S1. 19 Van de Kelft et al. presented a 97.5% accuracy rate including 1922 screws utilizing the O-arm navigation system in a multicenter trial. 26 Although there is increased accuracy rate of the pedicle screw placement, disadvantages of the intraoperative navigation system should not be ignored. Since image-guide spinal surgery carries a reported mean registration error up to 2–3 mm, any further changes to 3D anatomy subsequent to the registration scan may compromise pedicle screw accuracy rates. 9 The O-arm may take longer to set up, including the time spent in positioning the scanner, scanning, registration, and verification of registration. On the other hand, most of the screws were immediately inserted at the satisfactory screw positions without adjusting the screw directions in the O-arm-assisted system, resulting in reduced operative time. Possibly for this reason, Shin et al. found no statistically significant difference in operative time and estimated blood loss between navigated and nonnavigated cases. 27
To our knowledge, this is the first in the literature that compares the accuracy and safety of the intraoperative O-arm-assisted system without navigation procedure to conventional fluoroscopy. In our study, intraoperative three-axis view in the imaging screen of the O-arm machine offers better observation for the screw positions, which allows safe and accurate screw placement on the first attempt. The average time required for inserting a screw and the action times of adjusting the guide probe and pedicle screw in the O-arm group are less than respective ones in the C-arm group (p < 0.05). The hospitalization time in the O-arm group is shorter, which might be due to faster postoperative rehabilitation. The less fluid volume of wound drainage and less postoperative back pain, which might result from less action times of adjusting the guide probe and pedicle screw, could lead to faster postoperative rehabilitation in the O-arm group. There are the higher accuracy rate of satisfactory pedicle screw placement (grades 0 and 1) and the less incidence of medial perforation in the O-arm group compared to the C-arm group (p < 0.05). No further damage of the nerve function postoperatively is found according to the ASIA grade. The less repositioning of screws prevents further risk each time a screw is replaced.
Conclusion
The O-arm-assisted insertion of pedicle screws without navigation, which we described earlier, provides higher accuracy of pedicle screw placement and better clinical efficacy compared to conventional fluoroscopy (C-arm) technique.
Footnotes
Author contribution
HL and YW have contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.