
Abstract
Introduction
The integrity and longevity of silicone breast implants are critical in plastic surgery, affecting patient outcomes and the success of breast augmentation and reconstruction. Given reported rupture rates ranging from 5.4% to 34.2% within 10 years of implantation, examining all factors that may impact silicone breast implant shells is vitally important. 1 Many of the irrigating solutions used for surgical site antisepsis contain solvents and/or surfactants that aid in cleansing but may hold the potential to weaken breast implant shells.
This topic was of much interest in the early 2000s after the US Food and Drug Administration (FDA) issued a contraindication for povidone-iodine contact with any breast implant following the results of an in vitro study by Becker, suggesting significant tissue expander fill tube weakening following povidone-iodine exposure. 2 Subsequently, several studies were performed demonstrating no change in breast implant tensile strength or shell delamination after povidone-iodine exposure.3,4 In 2017, the FDA approved a change in the Directions for Use (DFU) stating povidone-iodine irrigation is unlikely to affect breast implant shell integrity. 5 Nonetheless, there remains mixed practice patterns regarding the use of povidone-iodine compared to other irrigating solutions.
Establishing a gold-standard irrigant for breast pocket antisepsis prior to implant placement remains controversial. Multiple systematic reviews have been conducted exploring this topic, but no clear consensus has been determined. In 2020, Baker et al highlighted the ongoing debate, noting that triple antibiotic solution (TAS) with or without povidone-iodine (PI, Betadine®) was the most common irrigant used. Other irrigants used were chlorhexidine gluconate (CHG) and hypochlorous acid (HOCl). Each irrigant was shown to have specific benefits, but none demonstrated clear superiority. 6 A review in 2025 showed similar conclusions: all irrigants lowered infection risk with varying effectiveness on capsular contracture. However, the studies still differed on the best irrigant. 7 As such, surgeons should continue to consider a combination of antiseptics and antimicrobials for infection prevention.
While these reviews provide a detailed comparison regarding the effectiveness of the different irrigants at preventing infection and capsular contracture, they do not explore the effect these solutions may have on breast implant tensile strength. To our knowledge, no study has been performed exploring this topic since the Povidone-iodine debate in the 2000s. While the effect of PI exposure on breast implants has been documented, little is known about the impact of the other commonly used irrigants on implant integrity. This study's purpose is to determine the impact of various irrigants on the tensile strength of breast implant shells based on irrigation exposures used during operative procedures.
Methods
Silicone breast implant shells from Mentor and Allergan Natrelle were cut precisely into 80 samples, measuring 2.5 cm by 2.5 cm. The silicone breast implant shells from each manufacturer were evenly and randomly distributed among the experimental groups. The solutions used for irrigation were as follows: 0.9% Normal Saline, Clindamycin-cefazolin-gentamicin antibiotic solution, 0.05% Chlorhexidine Gluconate (Irrisept®), Poloxamer 188 (SAF-Clens® AF Dermal Wound Cleanser), and 10% povidone-iodine (Betadine®). Poloxamer 188 was used as the control as the solubility of silicone in this detergent has been described. 8 Given limited predicate data, a preliminary power analysis indicated the need for a sample size greater than 10 per group. Twenty samples of implant shells, including 10 from each manufacturer, were tested in each experimental group. Each silicone implant shell was soaked in its respective irrigant for 60 s to ensure thorough exposure to the solution. Each silicone implant shell was then handled using forceps and gently blotted to remove any residual solution (Figure 1). After irrigation, the implant shells were tested using a commercial tensiometer (500 N Digital Force Gauge) to measure their mechanical properties. Each silicone implant shell was secured in the tensiometer with the tension jaw clamps set at a minimal distance from one another (Figure 2; left is at rest, right is stretched). To assess the tension properties of the silicone implant shells, tension was measured in Newtons over a displacement of 1.0 cm (approximately 0.39 inches). This measurement provided a quantitative evaluation of the tensile strength of the implants after exposure to the different solutions. Multiple attempts were made to displace the samples 2 times their distance (5 cm) but were unsuccessful as the implant samples avulsed at this amount of distance. A displacement distance of 1.0 cm allowed the samples to stretch as far as possible without avulsion. This allowed us to determine the relative tensile strength of the implant shells accurately and consistently.
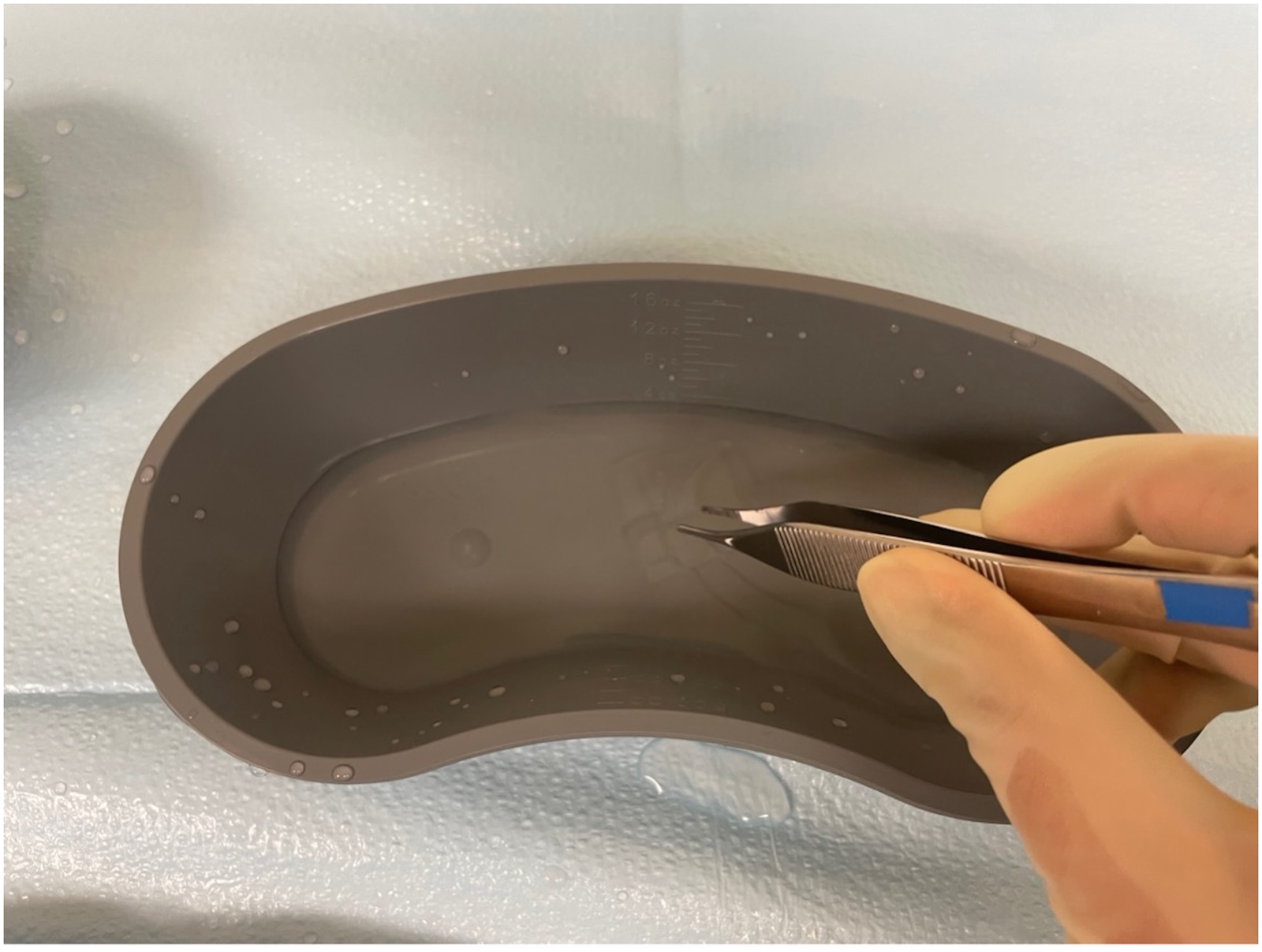
2.5 cm × 2.5 cm silicone implant shell handled using forceps.
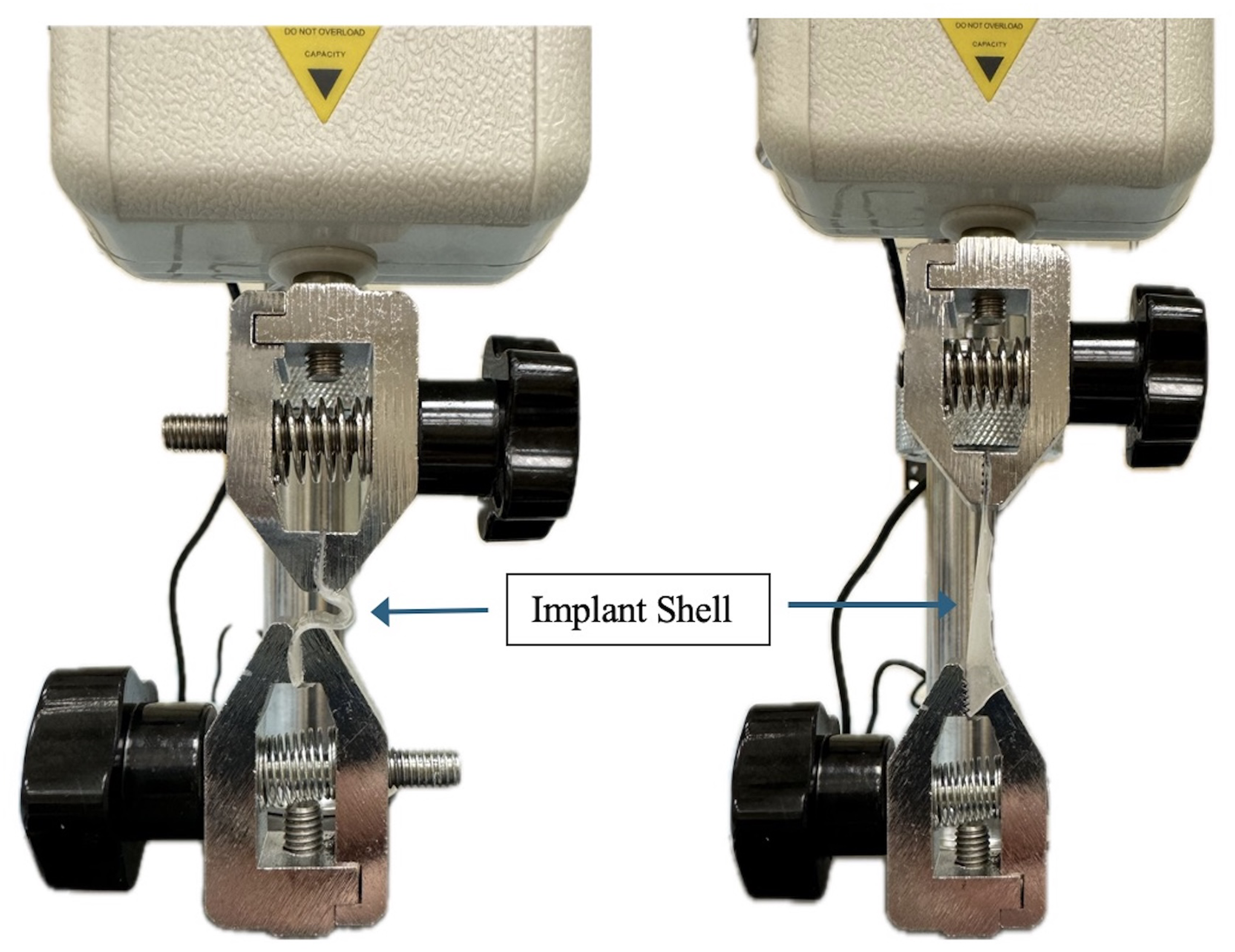
Silicone implant shell secured in the tensiometer. Left is at rest. Right is stretched.
Differences between all the irrigants were assessed using ANOVA followed by Tukey's Honestly Significant Difference (HSD) test for post hoc analysis. There were no violations of statistical analysis assumptions. The P-value of <.05 was considered statistically significant.
Results
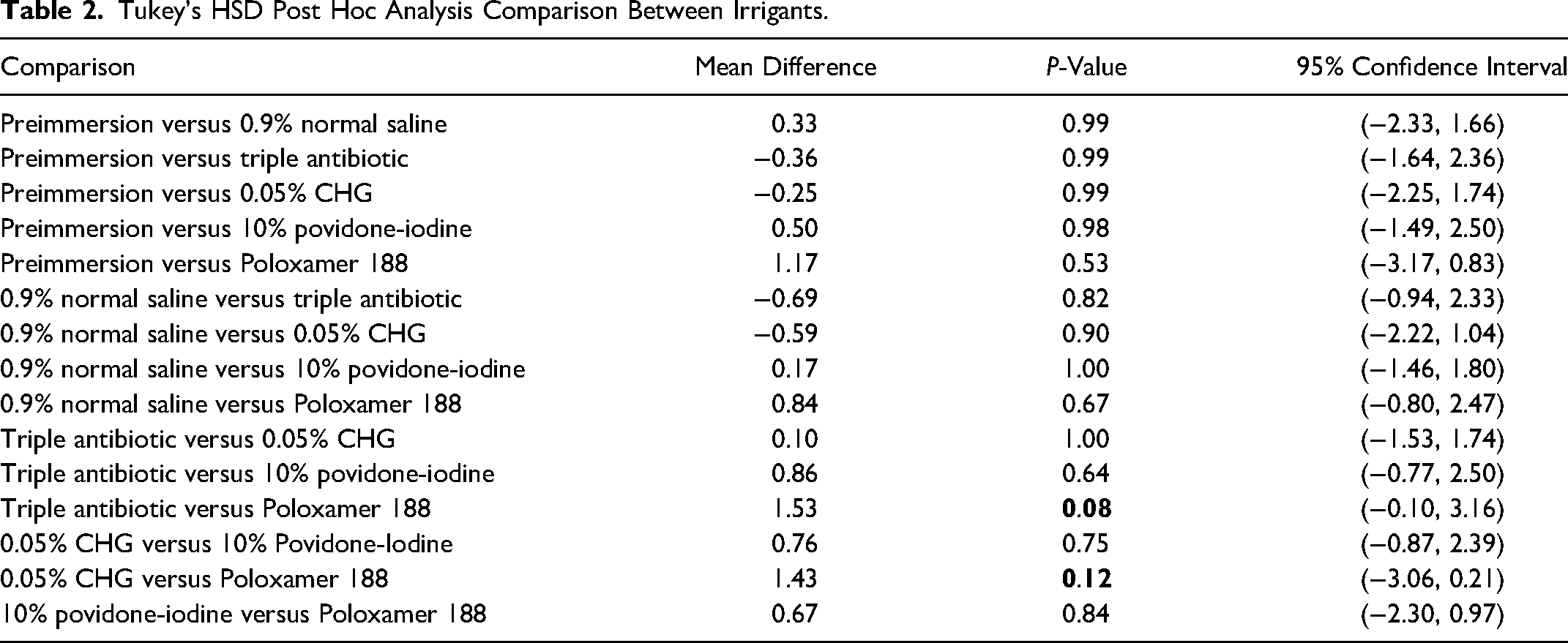
The average tensile strength (in Newtons) required to displace the implant shells by 1 cm after exposure to each solution is detailed in Table 1 and Figure 3. The average preimmersion tensile strength was 8.58 N. The implant tensile strength after exposure to the control Poloxamer 188 was 7.41 N. The implant tensile strengths after exposure to the other irrigants were higher: 8.25 N for 0.9% normal saline, 8.94 N for TAS, 8.84 N for CHG, and 8.08 N for PI. Differences between all the irrigants were assessed using ANOVA, demonstrating P = .085. Post hoc analysis was performed using Tukey's HSD test and detailed in Table 2. Comparison between TAS and Poloxamer demonstrated P = .08. pH of each irrigant is displayed in Table 3.
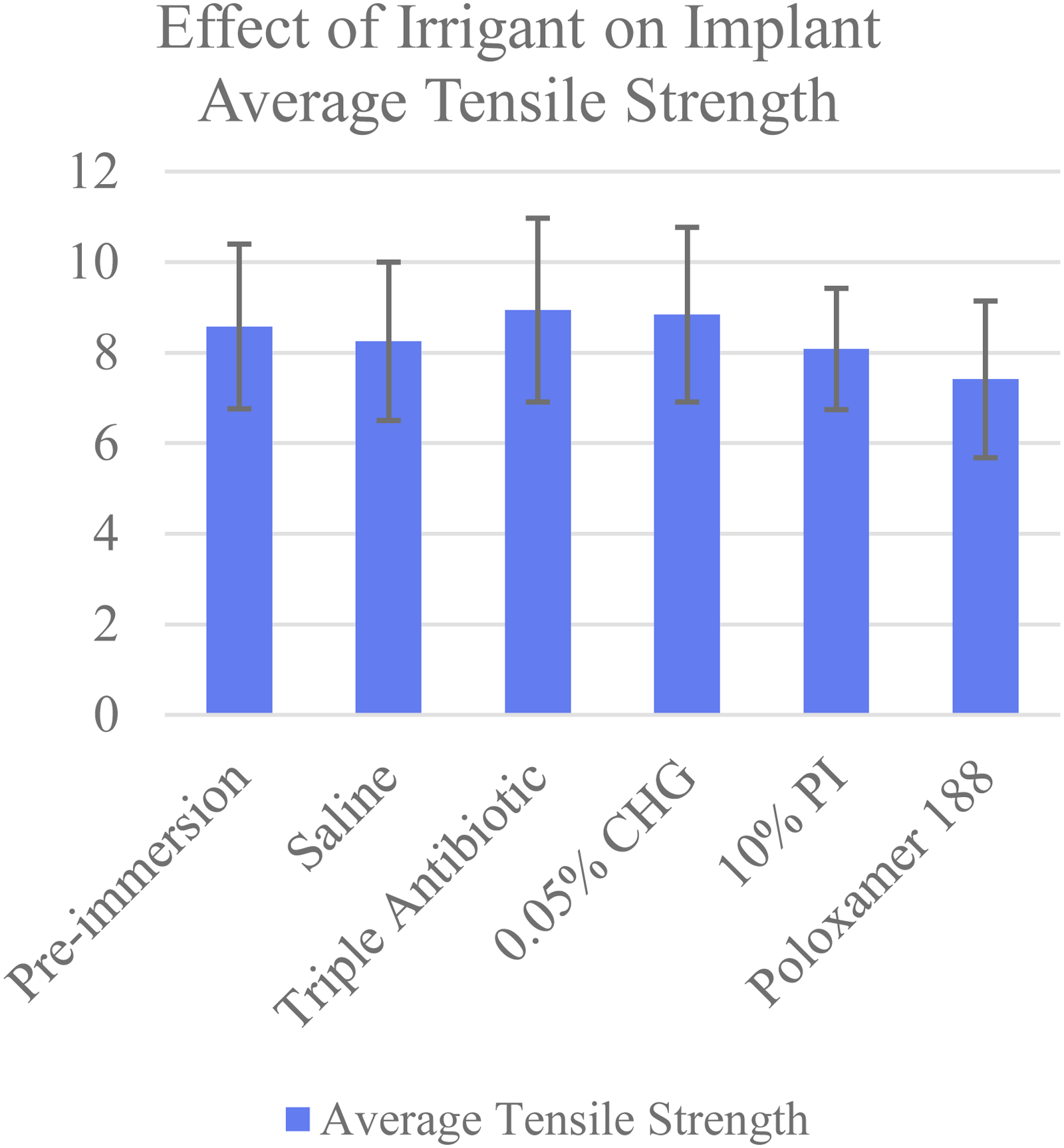
Effect of irrigant on implant average tensile strength.
Effect of Irrigant on Implant Average Tensile Strength.
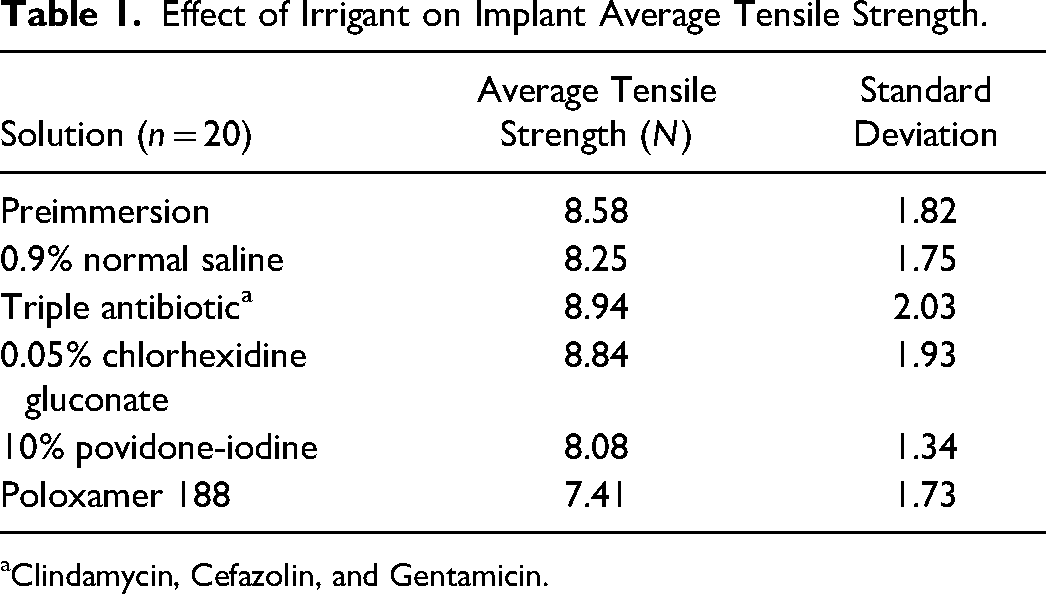
Clindamycin, Cefazolin, and Gentamicin.
Tukey's HSD Post Hoc Analysis Comparison Between Irrigants.
Irrigant Impact on Tensile Strength and Solution pH.
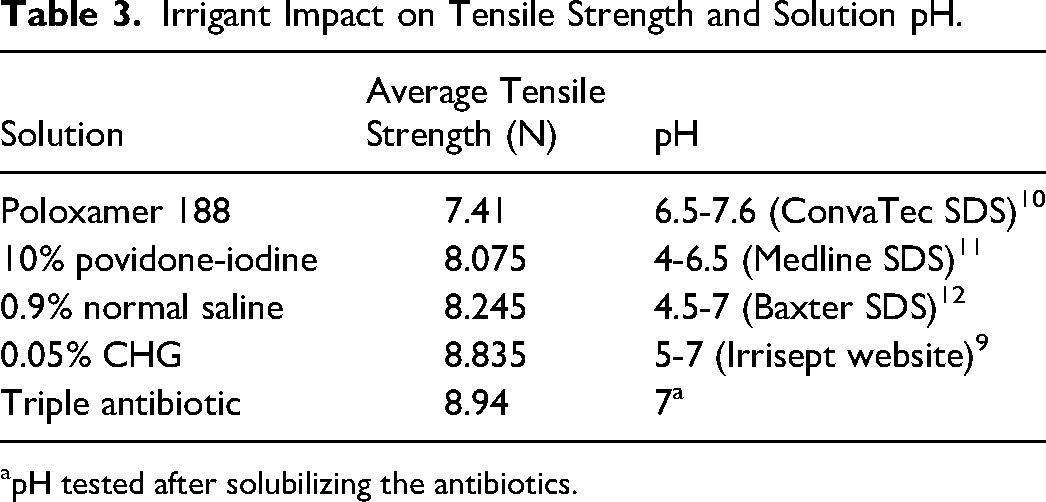
pH tested after solubilizing the antibiotics.
Discussion
The primary goal of this study was to evaluate the effects of various intraoperative irrigants on the tensile strength of silicone breast implant shells. We initiated the study by utilizing Poloxamer 188 as a control due to its known solubilizing effect and use in removing silicone following implant rupture. 8 Compared to the preimmersion tensile strength of 8.58 N, breast implant shells following Poloxamer 188 exposure resulted in a tensile strength of 7.41 N (mean difference 1.17 N). Implant tensile strengths after exposure to the other irrigants were all higher than that of Poloxamer with the highest being TAS (mean difference 1.53 N) and the lowest being PI (mean difference 0.67 N). One newton is defined as the amount of force needed to accelerate a 1-kilogram mass by 1 meter per second squared. For context, a small apple or a 100-gram stick of butter exerts a force of approximately 1 newton. Implants exposed to PI had a lower tensile strength than that of normal saline. However, there was no statistically significant difference in tensile strength between the 5 irrigation solutions. There was also no significant difference in implant tensile strength before and after solution immersion. Post hoc analysis did demonstrate a trend towards a statistically significant difference between TAS and the control Poloxamer (P = .08) and between CHG and Poloxamer (P = .12). Statistical differences likely would have been achieved if our sample size or exposure time was increased.
10% povidone-iodine, 0.05% chlorhexidine gluconate, triple antibiotic solutions, and 0.9% normal saline are all commonly used for irrigation of breast pockets during implant-based breast surgeries. Implant shells exposed to 10% povidone-iodine, known for its strong antiseptic properties, had a lower tensile strength compared to the other irrigants, which we hypothesized could in part be due to its pH of 4. However, there does not appear to be a correlation between the pH of the solutions and their impact on tensile strengths, as seen in Table 3. Additionally, prior studies have been performed showing no adverse effect of PI on breast implants.3,4 A meta-analysis by Engels et al in 2025 explored the effect of different irrigations on infection and capsular contracture. They concluded that PI was the most effective at reducing infection frequency, while TAS (cefazolin, gentamicin, bacitracin) was the most effective at reducing capsular contracture frequency. 13 Anthony et al performed a systematic review in 2025 exploring specifically for the optimal PI concentration for infection and capsular contracture prevention. Unfortunately, their results did not yield sufficient evidence to determine ideal concentration or application techniques. 14
The use of 0.05% CHG resulted in an implant tensile strength close to that of TAS. This indicates that chlorhexidine gluconate could be a promising alternative for intraoperative irrigation with antimicrobial effect without affecting implant integrity. CHG is a positively charged compound that interacts with the negatively charged surfaces of microbial cells, especially gram-positive bacteria. This results in cell membrane disruption, leakage of intracellular contents, and cell death. 15 0.05% Chlorhexidine gluconate (Irrisept®) is a common formulation that is non-cytotoxic and non-irritating, aiding in the removal of debris, bacteria, and microorganisms from wounds. 9 Several studies have demonstrated the superior efficacy of chlorhexidine gluconate solution when compared to povidone-iodine for surgical site antisepsis as well as in the field of orthopedics.16,17 Irrigating the breast pocket with 0.05% CHG has been found to reduce the number of microorganisms present in the surgical site, particularly decreasing Staphylococcus epidermidis biofilm formation compared to other commonly used solutions.18,19
Triple antibiotic solution consisting of clindamycin, cefazolin, and gentamicin maintained the highest tensile strength among the tested irrigants. This suggests that this antibiotic solution preserved the integrity of the silicone implant shells. However, there is much variability in the formulations of TAS and infection prevention outcomes. A prospective study by Hemmingsen et al found that TAS irrigation consisting of cefazolin, vancomycin, and gentamicin had adequate protection against Staphylococcus aureus but may be insufficient against Pseudomonas aeruginosa. 20 On the other hand, a prospective, randomized control trial by Walker et al demonstrated that TAS irrigation, consisting of cefazolin, gentamicin, and bacitracin, did not reduce bacterial abundance or impact microbial diversity when compared to saline breast pocket irrigation. In fact, TAS irrigation in breasts without cancer significantly increased bacterial abundance and changed the microbial composition, drawing to question the risks of antibiotic resistance. 21
0.9% normal saline had a median effect on implant tensile strength in our study. Although 0.9% normal saline is isotonic and often used as a control irrigant in many studies, it is interesting that the implant shells’ postimmersion tensile strength was lower than that of TAS and CHG (albeit not significant), and there was no difference between saline and Poloxamer. Many studies have compared the effectiveness of saline to other irrigants regarding infection and capsular contracture, which are discussed in a systematic review by Awad et al. There was no difference in capsular contracture risk between antibiotic irrigation and saline. However, there was a significantly lower rate of contracture with PI compared with saline. 22 Pfeiffer et al found a significantly lower infection rate after cephalothin irrigation compared with saline irrigation. 23
Poloxamer 188 exposure resulted in the lowest implant tensile strength. This finding is particularly important as Poloxamer 188 is commonly used in cases of implant rupture for the removal of silicone. 8 Our data suggests that while Poloxamer 188 effectively removes silicone from the breast pocket, it should be thoroughly rinsed out with a less harmful solution before implant placement to prevent compromising the implant's durability. Surgeons using solutions of Poloxamer 188 are cautioned to ensure thorough irrigation with additional solutions prior to implant placement.
We acknowledge that the in vitro results of this study do not translate to in vivo clinical experience. Tensile strength does not account for long-term biocompatibility, delamination, or interactions with surrounding tissues, all of which may impact the implant's integrity. Other limitations of this project include the short exposure time of 60 s, using flat sections rather than whole implants, and testing at non-physiologic temperatures. The 60 s exposure time was selected based on Irrisept's manufacturing guidelines and applied to all other irrigants. We recognize that the actual dwell time for breast implant irrigants, such as povidone-iodine and triple antibiotic solutions, is provider dependent and will vary compared to what was performed in our study. We also did not measure the implant shell rate of displacement, nor did we perform fatigue or aging tests. Our experimental conditions did not replicate the real-world stresses of breast implants, thereby limiting the generalizability of our results.
While there is much data regarding the effectiveness of irrigants on infection and capsular contracture as outlined above, further research is necessary to examine the long-term impacts of solution exposure on implant durability and to develop best practice guidelines for intraoperative use. Our findings underscore the importance of carefully choosing irrigation solutions that minimize the risk of weakening silicone breast implant shells during surgery while providing adequate antimicrobial coverage. This study provides a foundation for improving intraoperative care and optimizing patient outcomes in breast augmentation and reconstruction surgery.
Conclusion
This study demonstrates the effects of irrigation solutions on silicone breast implant tensile strength. Although no solutions showed a significant difference, there was a possible trend towards a difference between the triple antibiotic solution and chlorhexidine gluconate compared to Poloxamer 188. While it is accepted that antibiotic solutions designed for breast pocket irrigation are safe, solutions like 0.05% chlorhexidine gluconate (Irrisept) may offer a promising alternative in providing antimicrobial coverage during intraoperative use. When Poloxamer is used to remove silicone in the breast pocket, it should be thoroughly rinsed out with a less harmful solution before implant placement. These findings may guide surgeons in optimizing intraoperative practices to protect implant shell durability. Further research is warranted to examine long-term impacts of solution exposure on implant integrity and establish best-use guidelines for these agents.
Footnotes
Author Contributions
Leah Thomas: conceptualization, investigation, visualization, and writing (original draft). James Tran: formal analysis and writing (review/editing). Kylie McMath: conceptualization, investigation, and writing (original draft). Subhas Gupta: conceptualization, methodology, project administration, resources, supervision, and writing (review/editing).
Statement of Originality
This work represents original research that has not been published elsewhere and is not under consideration by another journal.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
This study did not involve human or animal participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.