
Abstract
Purpose
Surgical site infection following total knee replacement is considered as one of the most severe postoperative complications. The presence of bacteria at the surgical site is the most important risk factor and therefore it is essential to prevent infection through appropriate preoperative skin preparation. The purpose of this study was to examine the presence and type of native bacteria on the incision site and to assess which skin preparation is most effective to sterilize those native bacteria.
Methods
Scrub-and-paint 2 step method was used for standard preoperative skin preparation. 150 patients who underwent total knee replacement were grouped into 3 groups- Group 1 (povidone-iodine scrub-and-paint), Group 2 (chlorhexidine gluconate paint after povidone-iodine scrub), and Group 3 (povidone-iodine paint after chlorhexidine gluconate scrub). 150 specimens of post-preparation swabs were obtained and cultured. To analyze the native bacteria at the total knee replacement incision site, 88 additional swaps were performed before skin preparation and cultured.
Results
The positive rate of bacterial culture after skin preparation was 5.3% (8/150). Positive rates of the groups were 12% (6/50) in group 1, 2% (1/50) in group, 2 and 2% (1/50) in group 3 and positive rates of bacterial culture after skin preparation in group 2 and group 3 were lower than in group 1 (p = 0.037). Among the 55 patients who had positive bacterial culture prior to skin preparation, 26.7% (4/15) in group 1, 5.6% (1/18) in group 2, and 4.5% (1/22) in group 3 were positive. Group 1 showed 7.64 times higher positive bacterial culture rate after skin preparation than group 3 (p = 0.084)
Conclusion
During skin preparation prior to total knee replacement surgery, chlorhexidine gluconate paint after povidone-iodine scrub or povidone-iodine paint after chlorhexidine gluconate scrub had a superior effect on sterilizing native bacteria compared to povidone-iodine scrub-and-paint method.
Introduction
Surgical site infection (SSI) is considered as one of the most severe postoperative complications, leading to the extension of hospital stay and increase in medical expenses, and even death.1,2 Especially, SSI following total knee replacement (TKR) is a greater problem, and the incidence is increasing gradually. 3 The Presence of bacteria at the surgical site is the most important risk factor and therefore it is essential to prevent direct inoculation of native bacteria through appropriate preoperative skin preparation.
Preoperative skin preparation requires appropriate antiseptic agent. Povidone-iodine (PVI) and chlorhexidine gluconate (CHG) are the most commonly used antiseptic agents.4-6 Although several studies have assessed the efficacy of these agents, there is paucity of RCT on arthroplasty.
The purpose of this study was to examine the presence and type of native bacteria on the TKR incision site and to assess which skin preparation is most effective to sterilize those native bacteria. We evaluated and compared the efficacy of aqueous PVI and alcohol-based CHG as the most commonly used antiseptic agents in orthopedic surgery of extremities. We hypothesized that alcohol-based CHG is more effective than aqueous PVI. Scrub-and-paint 2 step method was used for standard preoperative skin preparation.7-13
Methods
Patient population
This trial was approved by the institutional review board (approval number: CR-20-148) of our hospital and conducted in accordance with the declaration of Helsinki.
The study was a prospective randomized controlled trial of 150 osteoarthritis patients, treated primary TKR from 31 July 2020.
All subjects were informed and agreed voluntarily before the study. The exclusion criteria were: patients with open wound scar, repeated surgery at the same site, an ulcer or sore at the surgical site, acute or chronic systemic infection, and allergic to solution materials.
Patients were directed to take a shower the day before the surgery. Prior to preoperative skin preparation, the surgical site was shaved. A dry sponge and razor blade were used to remove all the foreign substances on the skin.
After routine antibiotic sensitivity screening, prophylactic intravenous antibiotics were injected 30 min before the skin incision. Patients having TKR were injected 2 g of cefazolin. Patients allergic to penicillin and/or cephalosporin were injected 1 g of vancomycin.
Skin preparation
This study used the most commonly used Ministry of Food and Drug Safety (MFDS) authorized antiseptic agents - PVP-I 10% in aqueous solution (Besetine Solution ®; Hyundai Pharm, Seoul, KOR) and CHG 2% and Ethanol 72% (Hexitanol ET 2% Solution ®; Firson, Cheonan, KOR).
A gauze soaked with first antiseptic agent was used to scrub the site for 5 min and wiped out with a blotting towel. After the skin was fully dried, the second agent was applied for 5 min and swabbed after it was fully dried.
Randomization and masking
The patients were grouped into 3 groups- Group 1 (PVI scrub-and-paint), Group 2 (CHG paint after PVI scrub), and Group 3 (PVI paint after CHG scrub), by block randomization. In our study, block randomization was used to allocate 50 people to each group. To maintain balance between groups, the block size was set to be 30. The blocked randomization list was generated by an independent observer not involved in this study. The randomization allocation was concealed in an envelope until arrival in the operation room. To assure allocation concealment, numbers were kept in sealed envelopes, which were opened by an independent observer to ensure masked blocking. After the independent observer completed all preparations including skin preparation, the investigator entered the operating room and performed surgery. Although skin preparation agents had different colors, iodine-impregnated drape was used after obtain a bacterial culture specimen to prevent investigators from distinguishing between 3 groups. The investigator and subjects were completely blinded to their randomization until completion of this study.
Analysis of culture
Bacterial culture specimen was obtained from the patella center, which is the incision site, with dry, sterile, cotton-tipped swabs. Every TKR operation used a midline skin incision and the medial parapatellar approach.
First, a bacterial culture specimen of 150 patients was obtained by swab from the patella center skin after using the preparation agents. In order to analyze the native bacteria at the TKR incision site, 88 additional swaps were performed before skin preparation. The swab was sealed and carried in a sterile transport container to a microbiology laboratory and incubated for 5 days.
To observe the positive rate of bacteria and classify each group, we used the following media: Sheep blood agar plate, for Gram positive, Gram negative, yeast, candida, etc. and MacConkey agar, for Pseudomonas, Acinetobacter, Salmonella, etc.
We also considered patient factors which can affect the positive rate of bacteria such as gender, age, body mass index (BMI), smoking, diabetes mellitus (DM), and corticosteroid use.
Statistical Analysis
Sample-size requirements were based on the findings of a prospective study evaluating positive cultures from the foot and ankle following surgical skin preparation. 14 On the basis of the assumption that a 30% difference in positive culture rates would be clinically significant, the number of patients required to achieve 80% power at alpha = 0.05 was 45 patients per group. All the analyses were performed with IBM SPSS version 19.0 software (SPSS Inc., Chicago, IL) for Windows.
Descriptive statistics for all variables of interest were calculated. Continuous measures were summarized using means and standard deviations, whereas categorical measures were summarized using counts and percentages.
A Chi-square test was used on 3 groups to compare the positive rate of bacteria after skin preparation. Several patient factors and the presence of the bacteria were assessed by logistic regression analysis. A p value less than or equal to 0.05 was considered to be statistically significant.
Results
Analysis of bacterial culture before the skin preparation
Epidemiology of all patients.

Abbreviations: N = number, M = male, F = female.
Group 1: PVI scrub-and-paint
Group 2: CHG paint after PVI scrub.
Group 3: PVI paint after CHG scrub.

Native bacteria that has been collected and cultured before skin preparation were coagulase-negative Staphylococcus (38), Bacillus (11), and Micrococcus (6).
Positive rates were 53.6% (15/28) in group 1, 62.1% (18/29) in group 2, 71.0% (22/31) in group 3. Before skin preparation, there was no statistically significant difference in bacterial positive rate between the three groups (p = 0.386).
Analysis of bacterial culture after the skin preparation
The positive rate of bacterial culture after skin preparation was 5.3% (8/150). Positive rates of the groups were 12% (6/50) in goup1, 2% (1/50) in group, 2 and 2% (1/50) in group 3.
A chi-square test to identify the difference in positive isolates after skin preparation.

Group 1: PVI scrub-and-paint.
Group 2: CHG paint after PVI scrub.
Group 3: PVI paint after CHG scrub.
Analysis of positive bacterial culture rate after skin preparation in patients with bacteria before skin preparation.
Multiple variables logistic regression analysis of the difference in positive isolates after skin preparation.

Abbreviation: OR = odds ratio, CI = confidence interval, G1 = Group 1, G2 = Group 2, G3 = Group 3.
Group 1: PVI scrub-and-paint
Group 2: CHG paint after PVI scrub; Group 3: PVI paint after CHG scrub
aAdjusted by gender, DM.
Multivariate logistic regression analysis of positive bacterial culture rate
No factor had a significant effect on positive bacterial culture rate in the multivariate analysis performed with age, sex, BMI, smoking, DM, and corticosteroid use as a covariate.
For logistic regression analysis performed by selecting sex and DM for Forward conditional method, group 1 showed a 5.35 times higher positive bacterial culture rate than group 3 (p = 0.042). Group 2 was 2.29 times higher than group 3, but there was no statistical significance (p = 0.326) (Table 3).
Analysis of multiple variables effects for positive isolates after skin preparation.
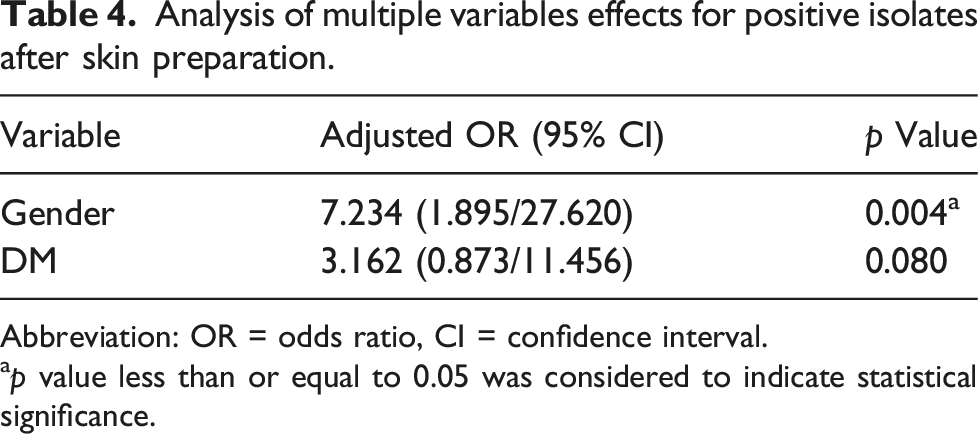
Abbreviation: OR = odds ratio, CI = confidence interval.
ap value less than or equal to 0.05 was considered to indicate statistical significance.
Discussion
Infection after TKR is one of the most serious complications, 15 which leads to increased treatment costs and mortality. Therefore, it is important to prevent infections. Since 2/3 of SSI is localized at the incision site 16 surgical site skin preparation with antiseptic solution before surgical incision is an important infection prevention measure. However, it is not clear which antiseptic skin preparation is the most effective in preventing infection, and therefore further research is required.
Currently, PVI and chlorhexidine gluconate (CHG) are the most commonly used preoperative skin antiseptics,4-6,17 and povidone-iodine is the most commonly used surgical skin preparation agent in orthopedic surgery.
PVI works as an antibiotic that has an affinity to bacterial cell membranes, rapidly penetrates into micro-organisms, and induces cell death by inhibiting microbial protein synthesis required for survival. 18
CHG changes osmotic equilibrium by binding to bacterial cell wall surface which is negatively charged. It changes the permeability of the cell wall thereby inducing leakage of the cytoplasmic component which makes bacterial apoptosis. 19 Alcohol-based CHG is more commonly used in skin preparation since it dries quickly and has a better disinfection effect. 8
Although studies have shown that the paint-only one-step method is equally effective against bacteria compared to the traditional two-step and pre-operative skin preparation methods,20,21 it is still controversial, and currently, most hospitals use the traditional two-step scrub-and-paint method.7,8
While several studies have shown that Alcohol-based PVI is less effective does not lower SSI risk compared to aqueous PVI22,23 other studies have shown that alcohol-based CHG is superior to aqueous PVI in skin disinfection at the surgical site,7-10 but many studies have shown that there is no significant difference.11-13
Bibbo et al. 7 have found that chlorhexidine-alcohol is superior to povidone-iodine in reducing bacterial carriage in foot and ankle surgeries. In the povidone-iodine preparation group of this study, 53 (79%) of 67 patients had positive cultures after skin preparation. In the chlorhexidine-alcohol preparation group, only 23 (38%) of 60 patients had positive culture after skin preparation. Overall, the povidone-iodine preparation group had more positive culture than the chlorhexidine-alcohol preparation group.
On the other hand, Rodrigues et al. 11 have found similar incidence of SSI in operations classified as clean or potentially contaminated for which skin preparation was done with povidone-iodine and chlorhexidine-alcohol. Seven of 102 patients in the povidone-iodine group and 11 of 103 patients in the chlorhexidine-alcohol group undergoing clean and potentially contaminated operation turned out to have SSI. Thus, there was no superiority of one antiseptic solution over the other.
Therefore, the author divided the patients who underwent TKR by one surgeon into three groups (PVI scrub and paint, CHG paint after PVI scrub, and PVI paint after CHG scrub groups) to access which agent was the most effective in sterilizing native bacteria on TKR incision site. Patients in each group were sterilized by verified preoperative skin preparation antiseptic agents, aqueous PVI, and Alcohol-based CHG. The use of PVI and CHG interchangeably was more effective than PVI alone in reducing bacteria after skin preparation.
There was bacterial culture prior to skin preparation, 62.5% (55/88) were cultured. The cultured bacteria were coagulase-negative Staphylococcus (38), Bacillus (11), and Micrococcus (6) in the order. There was also bacterial culture after skin preparation, 5.3% (8/150) were cultured, which were all bacillus species.
Bacillus species are a type of bacteria that exists in any environment. In the past, it was considered pollutants or non-pathogenic organisms. 24 However, cases were reported that Bacillus species cause infection in orthopedic surgery, 25 and cases of infection after knee surgery have also been reported. So this bacteria cannot be taken lightly. 26
In the bacterial culture performed after skin preparation, there was a statistically significant difference in the positive rate between group 1 (6/50) and groups 2 (1/50), and 3 (1/50).
We thought it was important to compare the positive bacteria culture rate after skin preparation in patients with bacteria before skin preparation to see the antiseptic effect of skin preparation. Our results showed that group 1 had 7.64 times higher positive bacterial culture rate after skin preparation than group 3 (p = 0.084), and group 2 was 1.24 times higher than group 3. However, the difference was not statistically significant (p = 0.884) (Table3)
Gender is an important factor in determining the microorganisms colonizing human skin. 27 Several studies have shown that there is a sex difference in the flora of organisms living in the skin due to the difference in sebum excretion, a sexual hormone, and skin surface pH.28,29 In fact, there are more bacteria present in males’ skin than in females’ skin. 27 Also, several studies have shown that diabetes is a risk factor for surgical site infection. 30
Since no factor had a significant effect on positive bacterial culture rate in the multivariate analysis performed with age, sex, BMI, smoking, DM, and corticosteroid use as a covariate, logistic regression analysis was performed by selecting sex and DM for forward conditional method.
Our study showed that men had 7.23 times more positive bacterial culture rate after skin preparation than women. Diabetic patients had a 3.16 times higher positive rate than non-diabetic patients. But the difference was not statistically significant (p = 0.080)
The present study has several limitations. First, culture specimens obtained before applying skin preparation agent were from only 88 patients, which could affect the actual bacterial positive culture rate. Second, in our study, there was no control over the false positive or false negative. Third, we used qualitative culture data to access the effect of skin preparation. In the future, studies including quantitative cultures should be conducted. Forth, there are many factors involved in the occurrence of clinical infection but were not considered in this study. However, a positive bacteria culture at the surgical incision site will certainly have a negative impact on infection, unlike a negative culture.
Despite these limitations, the strong point of this study is, to the best of our knowledge, the first study to reveal the native bacteria present in the knee region and show an effective skin preparation method.
Conclusion
During skin preparation prior to TKR surgery, CHG paint after PVI scrub or PVI paint after CHG scrub had a superior effect on sterilizing native bacteria compared to PVI scrub-and-paint method. Also, more attention is needed for male patients since men had a higher bacterial positive culture rate than women after skin preparation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Catholic University of Daegu (The grant of Research Institute of Medical Science).