
Abstract
Background:
The skin is the largest organ of the body, where many microorganisms reside. These microorganisms can produce detrimental effects if introduced into the body through surgical incisions. Therefore, the aseptic applications of the surgical site, with proper antiseptics, are necessary prior to an invasive medical procedure.
Objectives:
This study aims to identify the knowledge, attitudes, and practices on skin asepsis with the use of antiseptics and to identify the most preferred antiseptic by healthcare professionals in Sri Lanka, which allows understanding of whether the current procedure of skin antisepsis is up to the standard.
Methods:
A descriptive cross-sectional study was carried out among 210 healthcare professionals.
Results:
Most participants had poor knowledge (92.9%) and moderate attitudes with moderate practices (55.2%).
Conclusion:
This study highlights the need to improve further the existing skin antiseptic applications to address the gaps in knowledge, attitudes, and practices.
Introduction
Human skin is the largest organ in the body, with an average surface area of 30 square meters in adults 1 and is home to many microorganisms. These microorganisms on the skin have a tremendous potential to influence health. 1 They can cause infections if allowed into the body through cuts, scrapes, and surgical incisions. 2
Surgical site infections (SSIs) significantly burden healthcare systems, accounting for up to 20% of postoperative complications in colorectal surgery and 45% in head and neck cancer surgery. 3 They are also the second most common healthcare-associated infection in Europe, with a prevalence rate of 19.6%. 3 SSIs not only cause additional healthcare costs and consumption of antibiotics but can also lead to increased length of hospital stay, readmission rates, and the need for re-operation or intensive care. 4 SSI-related mortality and healthcare costs are estimated at €10 billion annually in the United States alone. 3
To address this issue, evidence-based strategies can prevent 65%–70% of SSIs. 5 A study at Colombo North Teaching Hospital in Sri Lanka found that 5.6% of blood cultures received were contaminated with microorganisms other than the target pathogen. 6 This is higher than the accepted contamination rates, indicating a need for aseptic techniques to correct the situation. In addition, an audit of blood collection techniques at the National Hospital of Sri Lanka in 2011 revealed that a large percentage of healthcare workers needed to adhere to standard guidelines when collecting blood for cultures, resulting in numerous false-positive results. 7 To minimize the risk of contamination and improve accuracy, it is crucial to establish standardized techniques and ensure that phlebotomists and blood culture teams receive adequate training with applicable guidelines. Effective hand hygiene practices and aseptic techniques are essential to maintaining the accuracy of blood culture results. 8
Therefore, the proper aseptic applications of the surgical site prior to an invasive medical procedure have been recommended to effectively reduce the occurrence of SSIs and related complications and costs. 9
As a standard before any invasive medical procedure, a cutaneous disinfectant is applied to reduce the microbial population in the skin section, commonly known as antiseptics. 10 Sri Lanka currently uses many different types of antiseptics in different concentrations according to availability and ease. 11 According to studies, the most widely used and clinically accepted antiseptic is chlorhexidine,12–14 although not very commonly used in Sri Lanka.14–16
Currently, there is a need for evidence-based survey studies in Sri Lanka on the commercial use of 70% alcohol, povidone-iodine, chlorhexidine, and other skin antiseptics, as well as the knowledge and attitude on the practical antiseptic usage in a healthcare setting. Therefore, the primary objective of this study was to identify the preferred antiseptic used in practice by medical professionals in Sri Lanka and explore the underlying factors that contributed to their selection. The study also sought to evaluate Sri Lankan healthcare personnel’s attitudes, practices, and knowledge surrounding the use of antiseptics.
Methods
Study design, setting, and population
A descriptive cross-sectional study was carried out to assess the knowledge, attitudes, and practices on applying antiseptics and skin disinfection prior to invasive medical procedures among healthcare professionals in Sri Lanka. The study setting consisted of conveniently selected healthcare professionals from the healthcare sector from all districts of Sri Lanka participating in skin antisepsis using antiseptics. The participants were recruited from KIU, the University of Kelaniya, and Colombo North Teaching Hospital (Ragama). The participants were contacted using their official work email groups with the approval of relevant authorities, and the study was conducted virtually using a Google Form. The study spanned a duration of 45 days, commencing on August 30, 2021. The study population included healthcare professionals (medical practitioners, surgeons, nurses, and medical laboratory technicians) in the healthcare professionals in Sri Lanka who had daily exposure to skin antiseptics.
The questionnaire, especially the knowledge-based section developed for this research, was based on established guidelines and recommendations from previous literature and research studies. These guidelines function as a point of reference for healthcare professionals, providing evidence-based best practices for hand hygiene and antiseptic use in various healthcare settings. Some of the main recommendations and guidelines that were included in the questionnaire are listed below:
Hand hygiene guidelines
The questionnaire included questions about hand hygiene procedures, which were informed by guidelines from reputable organizations such as the World Health Organization and the Centers for Disease Control and Prevention. These guidelines emphasize the importance of hand hygiene in preventing healthcare-associated infections and recommend using alcohol-based hand rubs with at least 70% alcohol or soap and water for handwashing in specific situations. 17
Antiseptic solutions
To assess participants’ knowledge of different antiseptic solutions, the questionnaire referred to research studies comparing the efficacy of various solutions. The incorporation of alcoholic chlorhexidine gluconate and povidone-iodine in the questionnaire was supported by evidence from previous studies done in the recent past.18,19
Aseptic techniques
Questions related to aseptic techniques, including skin preparation before procedures, were guided by recommendations from authoritative sources such as surgical and infection prevention guidelines from professional medical societies.
Variation in practices
The questionnaire explored the variation in practices among healthcare professionals based on their experience levels and specialities. These inquiries were underpinned by many previous studies17,20, which shed light on disparities in compliance and knowledge among healthcare workers.
Ethical considerations
Ethics were taken into account at every stage of the questionnaire preparation process and were in accordance with the rules governing research involving human subjects. The survey obtained informed consent from participants, and measures were implemented to safeguard their privacy and confidentiality.
This research ensured that the survey questions were grounded in established scientific knowledge by incorporating these evidence-based guidelines and recommendations into the knowledge-based questionnaire. The inclusion of authoritative sources and peer-reviewed studies lent credibility to the questionnaire and provided a solid basis for assessing the participants’ knowledge and practices related to hand hygiene and antiseptic use. Furthermore, this approach allowed the research findings to be contextualized within the broader framework of existing best practices and identified areas where further education and interventions could be targeted to improve patient care and safety.
Participants were enrolled through convenient sampling, and a Google form was sent to the sample population. The Google form was distributed among healthcare professionals in Sri Lanka via email and social media (Meta and WhatsApp).
Inclusion criteria were healthcare professionals (medical practitioners, surgeons, nurses, and medical laboratory technicians) in Sri Lanka with access to emails, social media, and the internet. The exclusion criteria were healthcare professionals (medical practitioners, surgeons, and medical laboratory technicians) who were unwilling to participate, did not have internet access, or had not adequately filled out the questionnaire form.
The descriptive cross-sectional study’s sample size is calculated using the following equation 21 :

n = sample size
p = expected proportion in the population is 60%/0.6 19 , 23
d = absolute error or precision is 0.05


n = 369
The electronic survey was then circulated to 400 healthcare professionals in Sri Lanka. In all, 210 responses were collected for this study using an electronic questionnaire via a Google link (52.5% response rate). In the discussion of this paper, this limitation will be explored. Prior to this, the study was pilot tested by sending the questionnaire link via WhatsApp to 10% of the final population (n = 21).
Ethical approval was obtained from the KIU Ethics Review Committee (KIU/ERC/21/79), and the Institutional Ethics Review Committee waived the written informed consent prior to study initiation. The decision to take part in the study was entirely voluntary. The participants were allowed the right to refuse to answer the questions. The participants had the right to withdraw from the study without any explanation, even if they had agreed earlier. The participants were not subjected to any charges for their involvement in the study nor were they remunerated for participating in this research.
The collected data were considered highly confidential and accessible only to the research team and the supervisors. The data collected by the questionnaire were stored in an Excel database and files, were kept strictly confidential, and accessible to the research team. A participant number tabulated the information collected from each participant to evaluate the results and did not use any personal details.
Data analysis
Data were collected using a pre-tested questionnaire in the manner of “Google Forms,” designed by the researchers using scientific literature.2,19,22–24 The survey was divided into five sections, as shown below, with a total of 31 items. These sections included 10 questions about practices, 5 questions about sociodemographics, 1 question on the most popular skin antiseptic, 7 questions about knowledge, 7 questions about attitudes, and 5 questions about practices. These items were employed for data collection purposes.
The level of knowledge was assessed using eight questions, including multiple-choice questions and “yes” or “no” questions. Attitudes were measured using seven statements, where the respondents were given the option to select on a 1- to 5-point scale between strongly agree and strongly disagree. Practices were assessed using eight multiple-choice questions.
Data were entered into an Excel sheet, coded, and then exported into IBM SPSS 25 for inferential and descriptive statistics analysis.
A scoring system was used where 1 point was given for each correct response to knowledge, positive attitudes, and good practices and 0 for incorrect knowledge, negative attitudes, and poor practices. Participants’ overall knowledge and attitude were categorized using Bloom’s cutoff point 21 as high if the score was between 80% and 100%, moderate if the score was between 60% and 79%, and poor if the score was less than 60%. The cutoff values were used to determine good, moderate, and poor levels using previously published studies with some modifications to suit our purpose. Descriptive statistics such as percentages, graphs, and inferential statistics such as the chi-square test were used to analyze the data.
Results
Among the total population (n = 210), there were 119 (56.7%) female participants. The mean age of the sample was 40 ± 13 years. The highest age of participants was recorded as 65 years, and the lowest age recorded was 21 years. The majority of participants (21.4%) (n = 45) were medical laboratory technicians (MLTs), followed by 16.2% (n = 34) public health inspectors (PHI), and 15.7% (n = 33) of the participants were midwives (Figure 1). The mean experience level of the participants of the study was 13 ± 12 years. The highest level of experience was found to be 42 years (Figure 2). Participants were recruited for the study from three different institutions. However, given the widespread distribution of healthcare workers across various districts in Sri Lanka, the study saw representation from participants in all districts of the country. Notably, a significant proportion of was recognized hailed from the Colombo district, accounting for 32.4% (n = 68) of the total participants. The majority of participants (83.9%) (n = 176) were from government institutions, including government hospitals, government laboratories, government universities, Ministry of Health Offices, nurse training schools, and family health midwife offices. 16.2% (n = 34) of the participants were from private hospitals and corporate medical institutes, which included private hospitals and private laboratories. Currently, there are around 600 government medical institutes and 100 private medical institutes in Sri Lanka. 25

The distribution of participants according to their occupations.

Distribution of the number of years of experience among participants.
When the most preferred skin antiseptic among the population was assessed, a majority of participants (75.7%) (n = 159) preferred 70% alcohol as a skin antiseptic, followed by 29.5% choosing (n = 62) povidone-iodine and 8.6% of the participants (n = 18) preferred hydrogen peroxide (Figure 3). The choice was among 70% alcohol, povidone-iodine, alcoholic chlorhexidine, aqueous chlorhexidine, hydrogen peroxide, chloroxynelol, and others.

Most preferred skin antiseptic among participants.
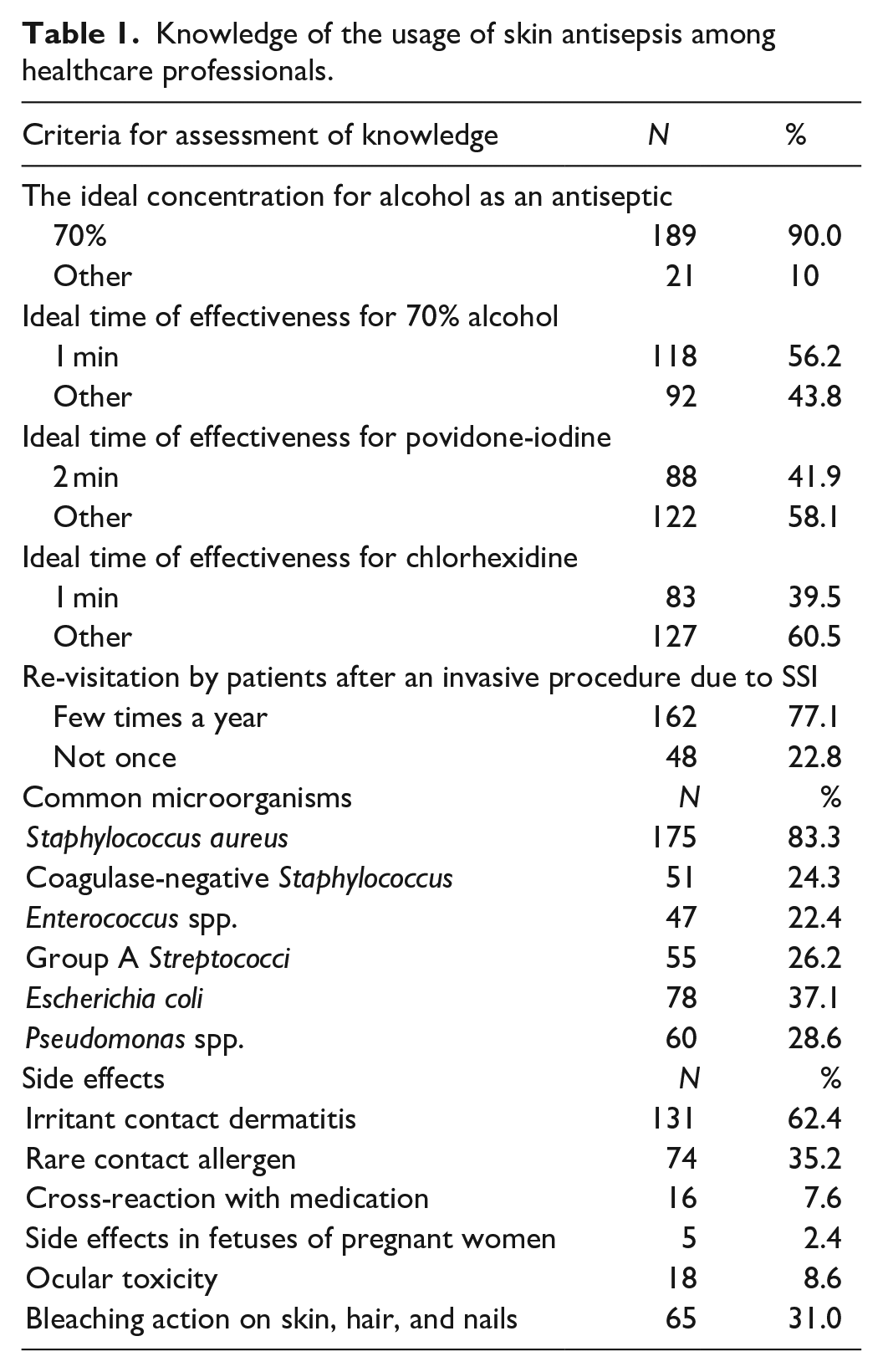
The knowledge of participants was assessed using seven multiple-choice questions. Each correctly chosen answer had a value of 1, and each incorrect answer and “Not sure” answer had a value of 0. The total marks obtainable from providing correct answers for each multiple-choice question was 17, and the lowest was 0. A majority (92.9%) of the participants had poor knowledge, 6.2% with moderate knowledge, and only 1% with good knowledge (Figure 4). In terms of experience, good knowledge was only seen among 3% of the participants with experience of less than 1 year and 3.8% of participants with experience of 1–5 years. Criteria for assessing participants’ knowledge and the results are listed in Table 1.
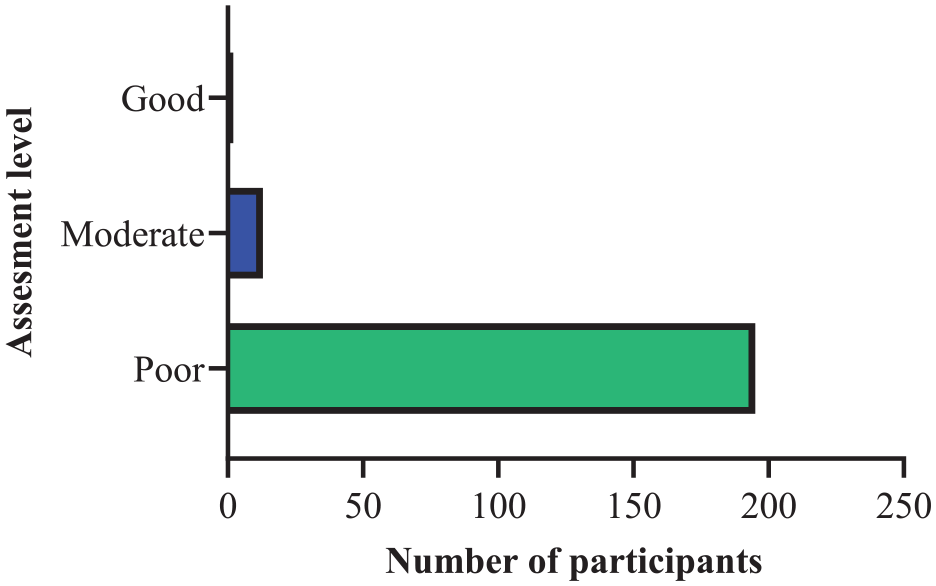
Assessment of participants’ overall knowledge.
Knowledge of the usage of skin antisepsis among healthcare professionals.
A chi-square test of independence was performed to assess the relationship between knowledge and age, knowledge and occupation of participants, and knowledge and experience of participants (Table 2). There was a significant relationship between each two variables, χ2 (21.12, N = 210) = 8, p = 0.007; χ2 (35.34, N = 210) = 14, p < 0.001; and χ2 (31.46, N = 210) = 18, p < 0.025, respectively. This showed that the age, occupation, and experience of participants are associated with the overall knowledge level of participants individually.
Chi-square tests of independence.

The attitudes toward skin antiseptics were assessed using seven statements for the overall population in Table 3. Responses to questions related to attitude were graded on a 5-point Likert scale, an agreement scale ranging from “1” for strongly agree to “5” for strongly disagree.23,24 55.2% of the participants were with moderate attitudes, 34.8% of the population were good, and 10% had poor attitudes (Figure 5).
The attitudes on the usage of skin antisepsis among healthcare professionals.

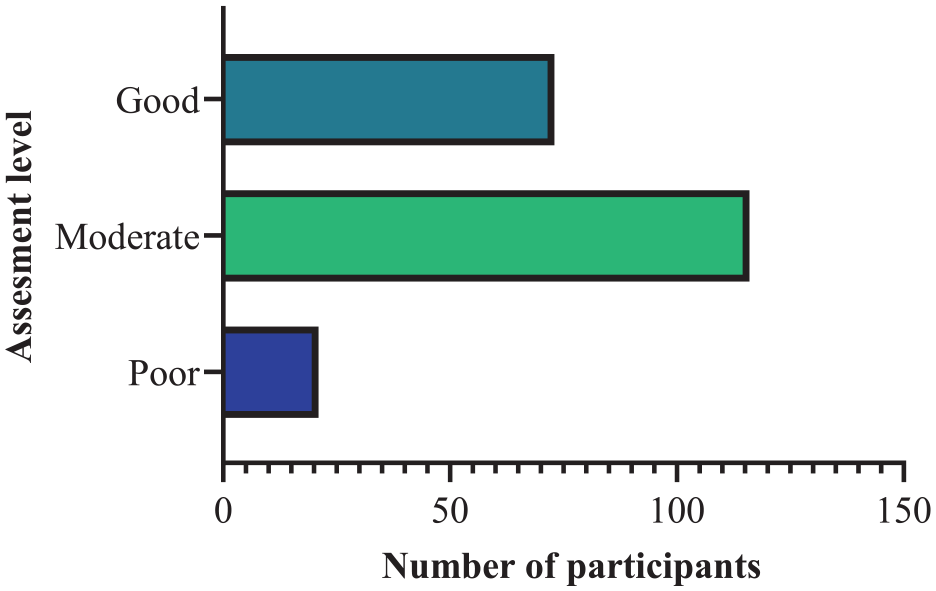
Assessment of participants’ overall attitudes.
A chi-square test of independence was performed to assess the relationship between the attitudes and experiences of participants (Table 4). There was a significant relationship between the two variables, χ2 (49.37, N = 210) = 18, p < 0.001. Participants’ experience and overall attitude levels are associated with each other (Figure 6).
Chi-square tests of independence.

Correlation between attitudes and level of experience among participants.
Table 5 lists the criteria and results which assessed the practices of using skin antiseptics of participants.
The practices on skin antisepsis among healthcare professionals.

Discussion
This electronic survey provides critical data on Sri Lankan healthcare professionals’ knowledge, attitudes, and practices using antiseptics during skin asepsis before an invasive medical procedure. In Sri Lanka, this study is expected to help prevent and reduce blood culture contaminations and SSIs.
The analyzed sociodemographic data of participants show that most responses were from MLTs (21.4%) in the age group of 21–30 years (38.1%). This study also consisted of 56.7% male participation. Most of the participants in the study were working in the Colombo district (32.4%) and healthcare professionals in government hospitals (46.7%). Using the results of this study, we identified that the main participants who provided accurate and valid facts were young participants who had updated their knowledge recently since the majority of responses (38.1%) were by the 21–30 age group, which was the youngest age group.
According to the results, the most preferred skin antiseptic among the majority (75.7%) of the participants was 70% alcohol, followed by 29.5% and 8.6% of participants selecting povidone-iodine and hydrogen peroxide as the second and third most preferred antiseptic, respectively. Many physicians and dermatologists do not recommend hydrogen peroxide as an antiseptic as it has been found to slow the healing process and can worsen scarring by killing healthy cells surrounding a wound. 26 Compared to 70% alcohol and povidone-iodine, only a small percentage of the population chose alcoholic chlorhexidine (6.2%), emphasizing the low preference for alcoholic chlorhexidine among healthcare professionals in Sri Lanka. However, it is commonly used in well-developed countries such as the United States27–29 Europe, 30 and Canada. 31
The assessment of the overall knowledge of the population on the use of skin asepsis indicated that a majority (92.9%) of healthcare staff need more knowledge (poor) on the use of antiseptics. When knowledge was assessed by age, experience, and occupation of participants, the age group of 21–30 years (2.5%), the experience range of 1–5 years (3.8%), and the occupation of MLT (4.4%) possessed good knowledge. The overall assessment of knowledge depicted that awareness creation on the role and the importance of skin asepsis before an invasive medical procedure is needed by a majority of healthcare professionals in Sri Lanka as indicated by the participants of this study. It is essential to focus more on an optimized standard protocol and to improve the knowledge gaps regarding skin asepsis to enhance the knowledge of healthcare professionals in Sri Lanka. In terms of experience, good knowledge was only seen among 3% of the participants with experience of less than 1 year and 3.8% of participants with experience of 1–5 years. With the increase in years of experience, there was a decrease in the level of knowledge. This calls for updating all staff members’ knowledge, especially participants with higher years of experience.
Staphylococcus aureus was the most common microorganism present on the skin surface (Table 1), according to most participants (83.3%). Several recent studies have introduced coagulase-negative Staphylococcus (80.6%), followed by Corynebacterium (7.4%), Micrococcus (6.5%), 32 Propniobacterium species, Clostridium species, and α-Streptococci 33 as the most common contaminants of blood culture. Several recent studies have introduced coagulase-negative Staphylococcus (80.6%), followed by Corynebacterium (7.4%), Micrococcus (6.5%), 34 Propniobacterium species, Clostridium species, and α-Streptococci32,33 as the most common contaminants of blood cultures. Therefore, this study is in agreement with prior literature and identifies Staphylococcus aureus as the most common isolated pathogen 30 based on the statistical data analyzed.
Most participants (62.4%) stated irritant contact dermatitis as the most typical side effect caused by skin antiseptics. At the same time, it was also found to be the common cutaneous side effect induced by antiseptics in a previous study. 35 According to this study by Lachenmeier, the main reason for the irritations might be due to the misuse of antiseptics. The application of concentrations too high or inadequate, occlusion, and improper usage of antiseptics among healthcare professionals evoke some side effects on the skin.
From the results of our study, 55.2% of the participants had moderate attitudes. While there was an evident lack of knowledge among the participants, most had good and moderate attitudes toward using antiseptics during skin asepsis. The highest values of good attitudes regarding skin antiseptics were seen among the age group of 61–70 years (71.4%) and also the participants with 36–41 years (100%) and 42–47 years (100%) years of experience. This shows that with the increase in age and years of experience among the participants, there was a significant increase in attitudes.
Compared to 70% alcohol, povidone-iodine, only a small percentage of the population chose alcoholic chlorhexidine, which emphasized the knowledge about the commercial usage of alcoholic chlorhexidine is very poor among healthcare professionals in Sri Lanka. The assessment of practices highlighted that while the techniques of using 70% alcohol was commendable among the participants, the practices of using chlorhexidine were deficient. 82.7% of participants agreed that the currently used skin antiseptic procedure in Sri Lanka is adequate and up to the standard. The audit on the technique of collection of blood for culture at NHSL in 2011 has determined that a high percentage of healthcare workers need to learn or adhere to standard guidelines. 9
The most significant limitation of this study was that the response rate was relatively slow due to the COVID-19 pandemic straining the medical workforce. This limitation also did not allow us to meet our target population of 369 before the end of the study. There is a preexisting limitation of marginalization of groups since online surveys call for digital literacy and access to digital technologies. This increases the exclusion of certain groups with access to technology but needs to be more skilled in information technology. The responses might have been more genuine if done as a verbal questionnaire rather than an online survey, with the participants having more understanding and allowing them to be more mindful of their answers. Oral questionnaires also allow more clarity in participants to understand the purpose of the research since they can clarify issues while the data are being collected. While the response rate of 52.5% may be low, according to a systematic review of 207 survey-based articles, one-third was based on online recruitment, and the average response rate was 34.2% (SD = 22.6). 36 Therefore, the generalizability of this study is not affected due to a lower-than-expected sample size. As a future recommendation, it is proposed to perform multivariate analysis, such as multivariate analysis of variance (MANOVA) or multivariate regression, using IBM SPSS 25 to enhance the statistical power of this study.
Conclusion
The study found that participants had low overall knowledge but moderate attitudes and practices regarding skin antiseptic procedures. Younger participants with updated knowledge showed better responses than more experienced individuals. This highlights the need to improve the existing procedure and address knowledge gaps through workshops or seminars. Such efforts can reduce SSI rates and associated economic burdens. Based on current literature, the study emphasizes the importance of a standardized skin antisepsis procedure. Chlorhexidine, a widely used and cost-efficient antiseptic, effectively reduces contamination and minimizes skin toxicity. The findings provide a basis for future laboratory-based studies to develop an updated procedure applicable to different invasive procedures. A comprehensive and cost-effective skin cleaning protocol is necessary, considering antimicrobial susceptibility and proper antiseptic usage. This standardized procedure can be adapted for specific invasive procedures based on participant recommendations.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231199654 – Supplemental material for Knowledge, attitudes, and practices on the usage of antiseptics prior to invasive medical procedures: Evidence from Sri Lankan Healthcare Professionals
Supplemental material, sj-docx-1-smo-10.1177_20503121231199654 for Knowledge, attitudes, and practices on the usage of antiseptics prior to invasive medical procedures: Evidence from Sri Lankan Healthcare Professionals by Yasheelee Thameesha Kalingamudali, Praba Jalini, Akila Jayamaha and Dehiwela Liyanage Jayaratne in SAGE Open Medicine
Footnotes
Acknowledgements
The researchers extend their heartfelt appreciation to the participants of this study and extend their gratitude to all individuals and institutions for their indispensable assistance during the course of the research and the writing phase.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors have no conflicts of interest to report. The authors confirm that the research presented in this article met the ethical guidelines of Kaatsu International University (KIU), Sri Lanka.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted as a survey study, making it a cost-effective research endeavor that required minimal funding and resources. We are pleased to highlight that no external funding was received for this study. The study design allowed us to efficiently collect data through electronically administered surveys, eliminating the need for physical materials and logistical support.
Moreover, conducting the survey study within a relatively small geographical area helped to minimize travel expenses and logistical complexities. By utilizing online survey platforms, we ensured easy access for participants, reducing the need for manual data entry, and streamlining the data collection process. This approach allowed us to focus our efforts on data analysis and interpretation, maximizing the efficiency and impact of the study.
Ethical approval
Ethical approval was obtained from the KIU Ethics Review Committee (KIU/ERC/21/79).
Informed consent
The written informed consent prior to study initiation was waived by the Institutional Ethics Review Committee.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.