
Abstract
Introduction
Cubital tunnel syndrome (CuTS) is the second most common compressive neuropathy of the upper limb and it occurs when there is compression or traction of the ulnar nerve around the elbow. 1 CuTS can be idiopathic or post-traumatic due to anatomic abnormalities or ulnar nerve subluxation. 2 Management of CuTS can be nonsurgical, including nighttime elbow splinting, or surgical with ulnar nerve decompression, medial epicondylectomy, or transposition of the ulnar nerve.1,2
Surgical management of CuTS can be done under one of three different types of analgesia: general, regional, or local anesthesia (LA). General anesthesia has been classically used on patients who are not suitable for regional anesthesia (RA) and for patients who would otherwise be unable to psychologically tolerate being awake while in surgery. 3 On the other hand, the latter two forms of anesthesia can be advantageous for the patient, surgeon, and the system overall.
Firstly, both RA and LA block nerve conduction in a designated area without providing systemic analgesia.4,5 Both of these techniques utilize a mixture of epinephrine, lidocaine, and other anesthetic compounds.5,6 For RA, and more specifically for upper extremity surgeries such as hand surgery, blockades are usually given as an axillary, supraclavicular, or intravenous blockade. 7 Methods of LA include Wide-Awake Local Anesthesia with no Tourniquet (WALANT) and LA with a tourniquet, with or without sedation.
The use of LA and RA has been shown to be equally effective as the use of full body sedation with tourniquet for patients undergoing carpal tunnel surgery in metrics including patient satisfaction and comfort.8,9 In other upper limb surgeries, there have been no reported differences in complications between traditional anesthesia techniques and the WALANT technique. 6 For patients undergoing cubital tunnel release, LA can be used in a minor procedures room and does not carry some of the risks associated with general anesthesia. 10
Recently, more research has been devoted to investigating LA for cubital tunnel release. Currently, no comprehensive review exists that summarizes the safety and efficacy of local and RA for ulnar nerve decompression surgery. The primary objective of this scoping review is to summarize current literature on the safety and efficacy of local and RA for cubital tunnel release. This will be assessed based on postoperative complications, recovery time, pain control or other metrics of patient satisfaction for patients undergoing CuTS release with local or RA.
Methods
A scoping review was conducted following PRISMA-ScR protocol and reporting guidelines. 11 A review protocol was registered on Open Science Framework (OSF: https://osf.io/5c4vd).
Search Strategy
After a preliminary search of the literature, a search strategy was developed based on two key concepts: cubital tunnel surgery and local or RA (Table S1). Inclusion criteria were studies that (1) reported on surgery for CuTS, (2) used local or RA for intraoperative anesthesia, (3) were published in a peer-reviewed journal, (4) included human subjects, and (5) were available in English. Studies were not limited by geographical range or date of publication. Databases included in this review were MEDLINE, EMBASE, Web of Science and CINAHL. The search was conducted on December 21, 2024 and EndNote was used to manage references.
Study Screening
Two independent authors conducted title and abstract screening using Covidence. If a conflict arose, the authors discussed it with a third author. Full-text screening was conducted likewise.
Data Extraction and Synthesis
Data was extracted to Google Sheets (Google LLC, Mountain View, CA, USA). Specific data included demographics, surgical details, anesthetic details, and post-operative outcomes (complications from surgery or anesthesia, recovery time, post-operative pain, etc.). Data were synthesized descriptively and presented in table format.
Inter-Reviewer Agreement
Inter-reviewer agreement was assessed using the kappa (κ) statistic. A priori agreement was defined as: κ of 0.91–0.99 was almost perfect; κ of 0.71–0.90 was considerable; κ of 0.61–0.70 was high; κ of 0.41–0.60 was moderate; κ of 0.21–0.40 was fair; and κ of 0.20 or less was no agreement. 12
Quality Assessment
Quality assessment was based on the Methodological Index for Non-Randomized Studies (MINORS) criteria. 13 Using the MINORS score and a priori classification, non-comparative studies could score a maximum of 16, and comparative studies could score a maximum of 24. 14
Results
Study Characteristics
The inter-reviewer agreement was considerable (κ = 0.63) for title and abstract screening, and almost perfect (κ = 0.96) for full text screening. After screening, 21 studies were included in this review (Figure 1). Most of the studies were case series or cohort studies (Table 1). The mean MINORS score for comparative studies was 17.2/24 (range 14–21) with all studies being considered fair, good or high quality (Table 1). For non-comparative studies, the mean MINORS score was 10.2/16 (range = 7–12) with one study being considered low quality and the remaining being fair quality (Table 1).
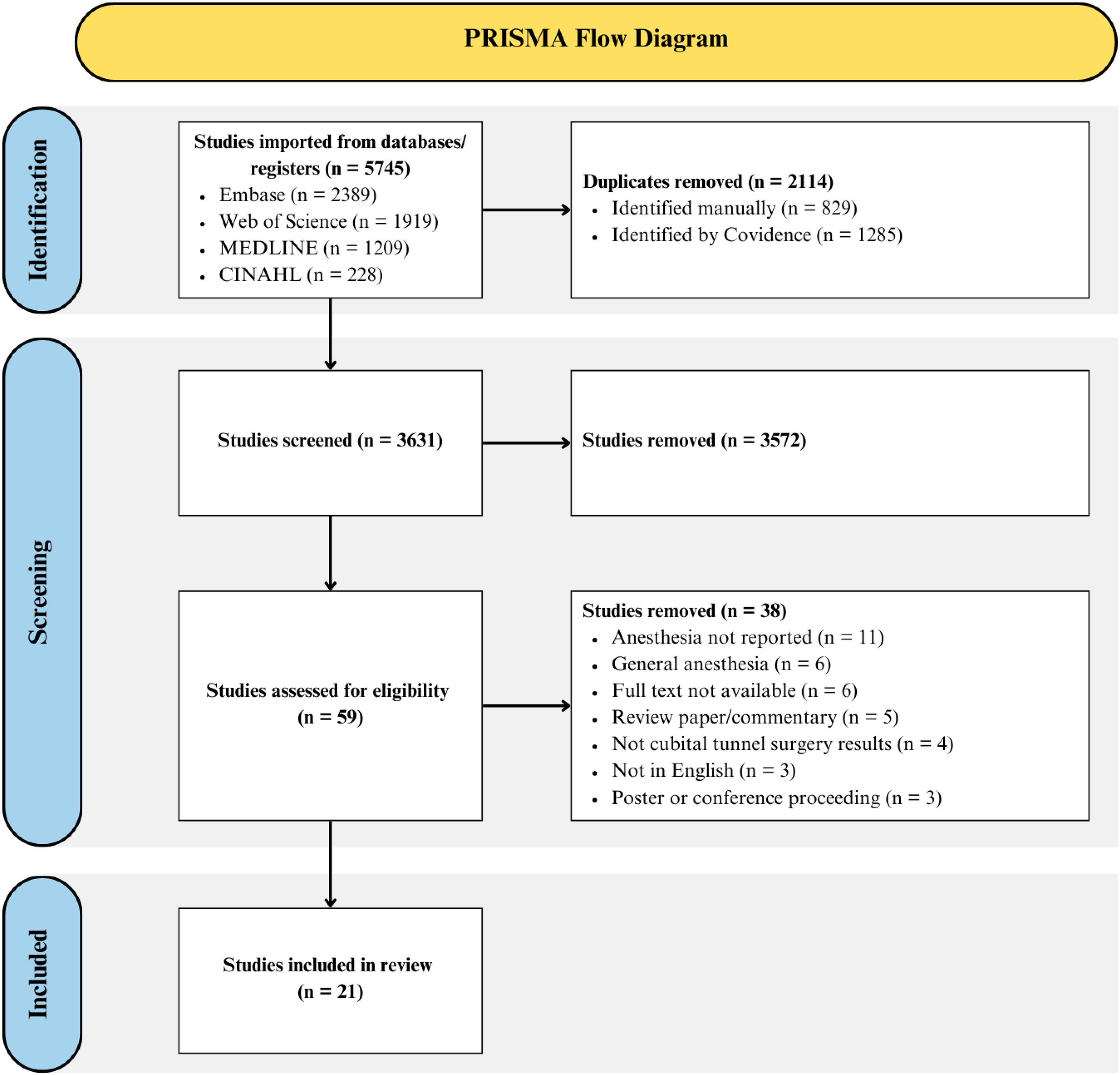
PRISMA Flow Diagram.
Demographic Data.
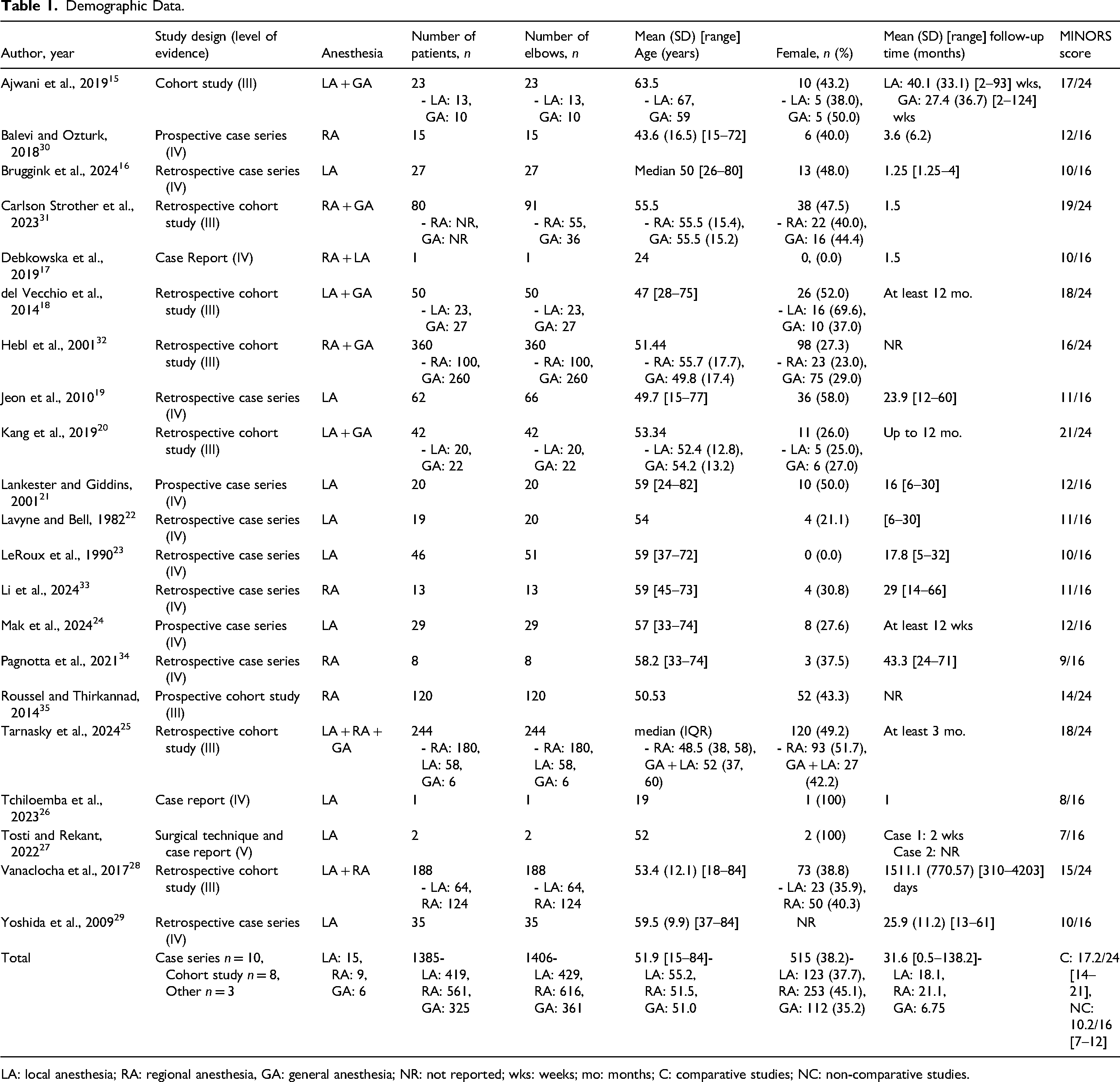
LA: local anesthesia; RA: regional anesthesia, GA: general anesthesia; NR: not reported; wks: weeks; mo: months; C: comparative studies; NC: non-comparative studies.
Demographics
A total of 1385 patients were included in this review with 1406 surgeries (Table 1). Fifteen studies used LA for 419 patients (429 surgeries).15–29 RA was used in nine studies for 561 patients (616 surgeries).17,25,28,30–35 Six studies compared local or RA to general anesthesia for a total of 325 patients (361 surgeries) receiving general anesthesia.15,18,20,25,31,32 The mean age of included participants was 51.9 years, and 38.2% of participants were female (Table 1). The mean follow-up time was 31.6 months (Table 1).
LA Only
Twelve studies assessed outcomes using LA alone for a total of 307 procedures. Among those studies, 10 used decompression surgery, while two performed a mixture of decompression and transposition (Table 2). Commonly used anesthetics were Lidocaine in eight (57%) studies, Bupivacaine in three (21%), Lignocaine in two (14%), and Marcaine in one (7%). In addition, epinephrine was used to supplement the anesthesia in nine (75%) of the 12 studies. Out of the 307 procedures completed with only LA, none were converted to general anesthesia and one case (0.3%) required intravenous sedation due to gross anxiety. Complications were reported in nine (2.9%) cases ranging from bleeding in three patients, two wound infections, two hematomas without further surgical intervention, one wound dehiscence, and one wound breakdown (Table 3). Compared to patients who received general anesthesia, those who received LA had less pain up to 48 h after surgery (p < .05) and less pain 2–12 h after surgery (p < .01). 20
Cubital Tunnel Surgery Under Local Anesthesia Only.
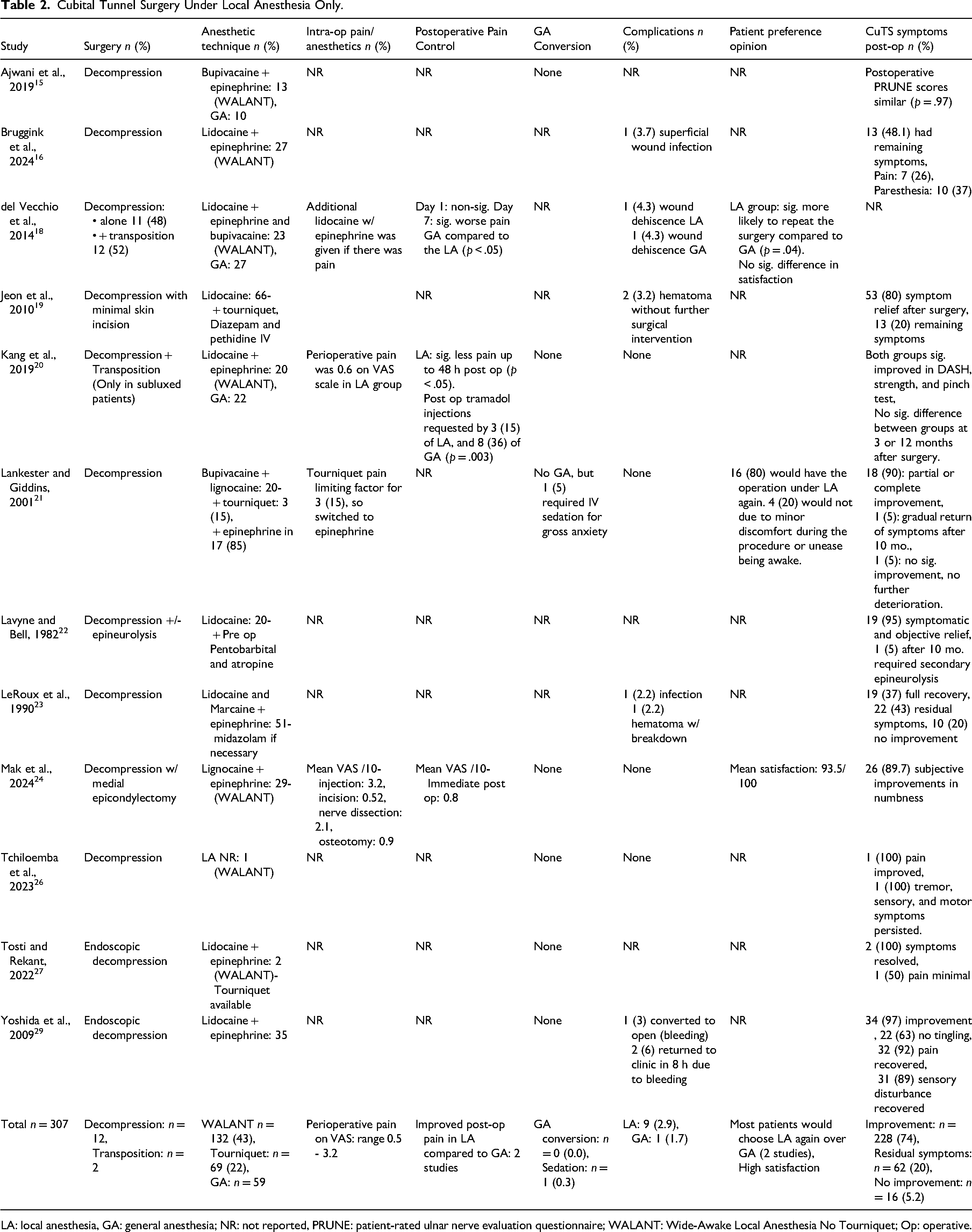
LA: local anesthesia, GA: general anesthesia; NR: not reported, PRUNE: patient-rated ulnar nerve evaluation questionnaire; WALANT: Wide-Awake Local Anesthesia No Tourniquet; Op: operative.
Cubital Tunnel Surgery Under Regional Anesthesia Only.
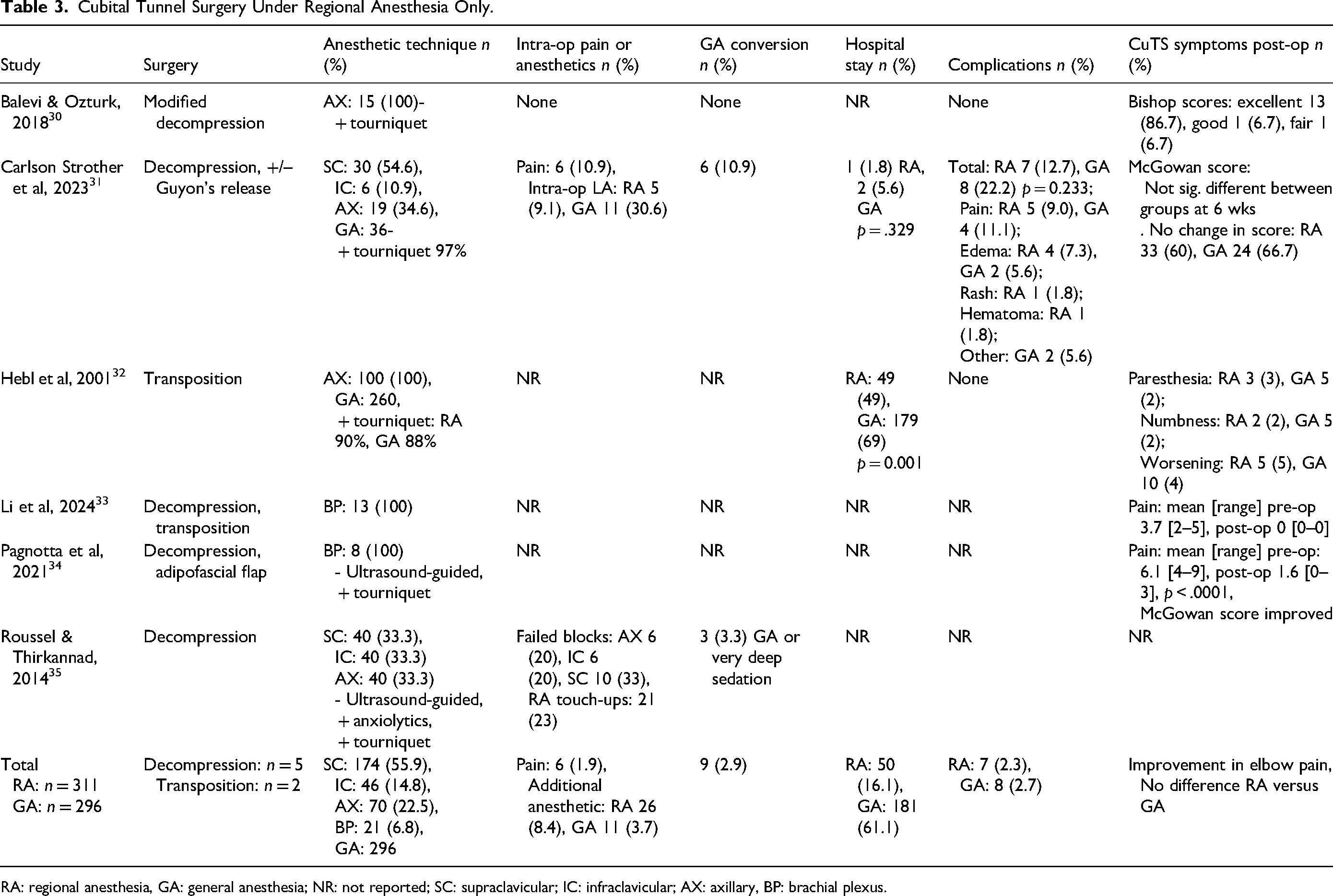
RA: regional anesthesia, GA: general anesthesia; NR: not reported; SC: supraclavicular; IC: infraclavicular; AX: axillary, BP: brachial plexus.
After surgery with LA, cubital tunnel symptoms improved in 228 (74%) patients (Table 2). No improvement was reported in 16 (5.2%) patients. In 62 (20%) patients, there were residual symptoms such as pain, paresthesias, or numbness (Table 2). There were no significant differences in postoperative cubital tunnel symptoms in patients who received LA compared to general anesthesia.15,20 Patients were more likely to have improvements if their preoperative symptoms were mild, had an onset < 1 year prior to surgery, and did not involve muscle atrophy. 23 Patient preference was reported in favour of LA in two studies, and another reported high patient satisfaction.18,21,24 Notably, 20% of patients in one study would not repeat the procedure with LA due to minor discomfort or unease related to being awake in the operating room. 21
RA Only
In six studies that assessed RA for cubital tunnel surgery, supraclavicular blocks were the most common, being performed in 55.9% of patients (Table 3). Out of 311 patients who received RA, there were 6 (1.9%) reports of intra-operative pain. Additional anesthetics, including intraoperative LA and RA touch ups, were required in 26 (8.4%) of patients (Table 4). In comparison, 11 (3.7%) control patients receiving general anesthesia were given additional intraoperative local anesthesia. Overall, nine (2.9%) of patients who received RA were converted to general anesthesia or required very deep sedation, largely due to pain.
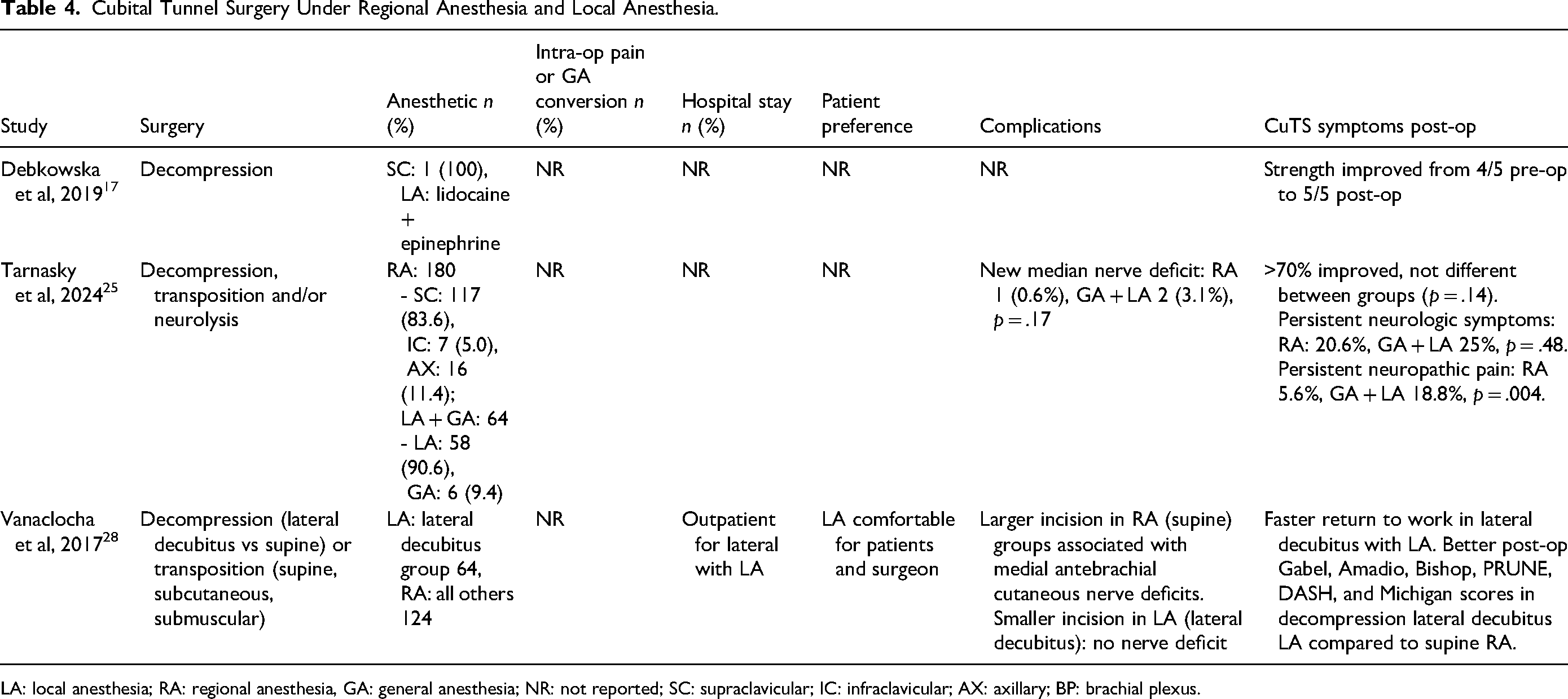
Cubital Tunnel Surgery Under Regional Anesthesia and Local Anesthesia.
LA: local anesthesia; RA: regional anesthesia, GA: general anesthesia; NR: not reported; SC: supraclavicular; IC: infraclavicular; AX: axillary; BP: brachial plexus.
One study reported no difference in the number of patients requiring an overnight hospital stay for post-operative pain control between regional and general anesthesia. 31 However, another study reported a significantly lower rate of overnight hospital stay in patients who received RA compared to general anesthesia (Table 3). 32 Minimal complications were reported post-operatively for patients receiving cubital tunnel surgery under RA (Table 3). Complications were reported at a similar rate (2.3–2.7%) between patients receiving regional and general anesthesia, including pain, edema, rash and hematoma (Table 3). Improvements in CuTS symptoms, including elbow pain, were similar between patients receiving regional and general anesthesia (Table 3).
Local and RA
In a case report of a hemophiliac patient undergoing ulnar nerve decompression at the elbow, the patient received a supraclavicular nerve block plus local infiltration of lidocaine and epinephrine. 17 There were no complications related to the anesthesia or surgery, and the patient's cubital tunnel symptoms improved post-operatively (Table 4).
Another study compared patients who received a peripheral nerve block versus patients who received either local or general anesthesia for decompression, transposition and/or neurolysis of the ulnar nerve at the elbow. 25 There was less persistent neuropathic pain in patients who received RA compared to patients who received either general or local anesthesia (Table 4). Otherwise, the rate of improvement was similar between RA and general or LA. 25
A third study compared ulnar nerve decompression and transposition in the lateral decubitus and supine positions. 28 Patients who had ulnar nerve decompression in the lateral decubitus position received LA, whereas all other patients received RA (Table 4). Patients in the lateral decubitus with LA group had smaller incisions, fewer postoperative nerve deficits and a faster return to work compared to patients who had surgery in a supine position with RA. 28 Patients and surgeons reported being comfortable using LA during the surgery.
Discussion
Overall, the current scoping review shows that regional and local anesthetic techniques are safe and feasible for cubital tunnel release. Complications for cubital tunnel release were reported in 2.9% of patients receiving LA, 2.3% of patients receiving RA and 2.5% of control participants with general anesthesia. These rates of complications are comparable to previous research reporting a complication rate of 3% across eight different surgical techniques for cubital tunnel decompression. 36 The main complications reported were pain, edema, hematoma, wound dehiscence and infection.
Several benefits of LA have been suggested by previous research. 10 In the current review, 43% of procedures with LA were conducted with WALANT. This surgical technique allows for patient-surgeon interaction during surgery, which can provide real-time feedback as to the effectiveness of the procedure. 37 In addition, local anesthetic techniques such as WALANT do not necessarily require preoperative fasting or the cessation of home medications, which allows patients with contraindications for general anesthesia to receive surgery. 38 On an economical side, LA is less resource intensive than general anesthesia as it can be done in an office-based or minor procedures setting rather than in an operating room.10,38 As well, patients recuperate faster after surgery, which reduces the need for postoperative recovery rooms. 38 This allows surgeons to use their outpatient offices for surgeries, helping reduce not only the load on the healthcare system but also the cost associated with the surgery. 8 Previous studies have shown that WALANT is equally as effective as other traditional anesthesia techniques for carpal tunnel release and other upper limb surgeries.6,39
In the current study, most patients were satisfied with LA and would choose it again over general anesthesia. As well, patients who had LA had lower postoperative pain compared to those who had general anesthesia. Patients who would not have the procedure again complained of minor discomfort during the procedure or unease at being awake in the operating room. Patients most commonly have discomfort during LA because of either incomplete tumescence of the operative field due to insufficient volume of LA, or not waiting a sufficient length of time for the LA to take effect prior to commencing. 40 Anxiety during the procedure could be mediated by administering additional anxiolytics as needed or modifying the operating room environment, such as by having relaxing music. As well, patient selection for local and RA should consider the patient's baseline anxiety, to ensure that patients are suitable candidates.
When compared to general anesthesia, RA has been shown to reduce postoperative nausea, vomiting and chronic pain. 41 Some evidence suggests that RA also reduces postoperative infection rates. 42 RA can lead to decreased blood loss during surgery, and helps reduce the metabolic stress response to surgery. 43 More specifically, RA reduce the likelihood of mortality due to deep vein thrombosis, pulmonary embolisms, transfusion requirements, pneumonia, or respiratory depression. 44 The findings of the current review build on previous research by showing that RA also decreases the likelihood of patients requiring an overnight hospital stay.
On the other hand, both of these methods have associated disadvantages. One of the most severe potential complications with the use of local or regional anesthetics is Local Anesthetic Systemic Toxicity (LAST). 45 LAST is a potentially lethal complication that involves a collection of progressively worsening neurological or cardiovascular symptoms due to anesthetic medication entering circulation. 46 The risk of LAST in tumescent LA is negligible if long-lasting bupivacaine or ropivacaine are avoided and the maximum recommended dosage limit of 7 mg/kg of lidocaine with epinephrine is followed. 47 The risk of LAST in regional nerve blocks can be reduced by almost four-fold with the use of an ultrasound. 48
Another possible complication of WALANT is vasovagal syncopal episodes during local injection. 49 In the current review, no such events were reported. In patients who had LA with a tourniquet, pain related to the tourniquet was a limiting factor. This can be avoided by using epinephrine to control surgical bleeding rather than a tourniquet. In patients who received RA, 2.9% were converted to general anesthesia or required deep sedation. Patients should be thoughtfully selected for local and RA to ensure they are suitable candidates, which can reduce the risk of requiring general anesthesia conversion.
Among the key strengths of this scoping review is the broad inclusion criteria that allowed for the inclusion of various types of literature and study designs, such as case series, cohort studies, and case reports. Another strength of this scoping review is that it assesses the methodological rigor and risk of bias within the included studies. This scoping review can provide guidance to surgeons and anesthetists planning for cubital tunnel surgery. By offering local or RA to appropriate patients, this can lead to changes in practice that improve patient postoperative pain and decrease hospital admissions.
A limitation of this scoping review is the limited amount of studies available to analyze. Most studies were case series or cohort studies and no randomized controlled trials were available. In addition, the results of included studies were predominantly descriptive, precluding the ability to synthesize data statistically. Future research should involve high-quality randomized controlled trials comparing cubital tunnel release under local, regional and general anesthesia to confirm the findings of this study.
Conclusion
In conclusion, cubital tunnel release under local and RA is safe and feasible. These anesthetic techniques have similar complication and success rates as general anesthesia. They offer the benefits of intraoperative feedback, improved postoperative pain control, and lower rates of overnight hospital stay. Future research should consider randomized controlled trials to further evaluate these findings.
Supplemental Material
sj-docx-1-psg-10.1177_22925503251404418 - Supplemental material for Cubital Tunnel Release Under Local and Regional Anesthesia: A Scoping Review
Supplemental material, sj-docx-1-psg-10.1177_22925503251404418 for Cubital Tunnel Release Under Local and Regional Anesthesia: A Scoping Review by Madeline E. Hubbard, Amr AlMasri and Nasimul S. Huq in Plastic Surgery
Supplemental Material
sj-docx-2-psg-10.1177_22925503251404418 - Supplemental material for Cubital Tunnel Release Under Local and Regional Anesthesia: A Scoping Review
Supplemental material, sj-docx-2-psg-10.1177_22925503251404418 for Cubital Tunnel Release Under Local and Regional Anesthesia: A Scoping Review by Madeline E. Hubbard, Amr AlMasri and Nasimul S. Huq in Plastic Surgery
Footnotes
Authors Contributions
All authors were involved in conceptualizing and designing the scoping review. MH and AA conducted screening and analysis for the scoping review with interpretation from NH. MH and AA drafted the manuscript and all authors revised it critically. The final manuscript was approved for publication by all authors.
Data Availability
Data can be made available upon request to the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
This study was a scoping review consisting of previously peer-reviewed, published articles; therefore, no ethics approval was required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.