
Abstract
Facial nerve blocks are widely used techniques for analgesia to the face and utilized by surgeons to facilitate facial procedures. The aim of this review is to explore the different nerve blocks of the face. Therefore, a comprehensive literature search of PubMed, Scopus, Elsevier, and Web of Science was conducted to identify relevant literature related to facial blocks. For each block reported, the literature was screened for relevant information on indications, techniques, and complications. The facial nerve blocks identified in the current literature for facial surgery procedures were supraorbital and supratrochlear blocks, maxillary nerve block, inferior alveolar nerve block, lingual nerve block, mental nerve block, nerve block of the nose, and auricular nerve block. Success rates in both achieving anesthesia and postoperative pain control has been reported to be between 70% and 90%. The most frequent adverse effects of these blocks were allergic reaction, bleeding or hematoma, infection, and nerve damage due to nerve compression. On the other hand, few studies have investigated the efficacy and patient-reported outcomes. Variable levels of analgesia and anesthesia have been reported between the discussed facial nerve blocks, with each yielding a different advantage. Further studies are necessitated to report on the block duration and patient outcomes reported by each facial nerve block discussed in this review.
Introduction
Nerve blocks are a highly useful technique for the application of analgesia to the face, with successful analgesia improving cosmesis, patient satisfaction, and reducing discomfort during wound repair and procedures. 1 During craniofacial procedures, facial nerve blocks are a common approach used by surgeons and comprise the administration of local anesthetics (LA) near the sensory nerves supplying a given surgical field. 2 The nerve block technique yields several benefits compared to other techniques, such as wide local infiltration and field blocks, including the small amount of LA required to anesthetize a large area, increased patient comfort due to fewer injections, and the smaller amount of solution. 3 Facial nerve blocks have been successfully administered to patients for more than 100 years 4 ; however, there are numerous different blocks utilized by surgeons that offer different advantages to patients.
This review will explore facial nerve blocks commonly used by surgeons, including supraorbital and supratrochlear, maxillary, inferior alveolar, lingual, and mental nerve blocks, nerve block of the nose, and auricular nerve block. The overall aim of this research is to facilitate the use of facial nerve blocks by providing a core resource on the different types of nerve blocks, indications (Supplemental Table 1), block duration, complications (Supplemental Table 2), and resulting patient satisfaction.
Methods and Materials
A comprehensive search of PubMed, Scopus, Elsevier, and Web of Science was conducted to identify research articles that investigated facial nerve blocks during craniofacial procedures. For each block reported, the literature was screened for relevant information on the indications, techniques, adverse events, complications, and patient-reported outcomes.
Trigeminal Nerve Anatomy
The trigeminal nerve provides sensory innervation to the face. The trigeminal ganglion is located in the trigeminal or Meckel’s cave of the petrous section of the temporal bone. It is divided into 3 branches: the ophthalmic (V1), maxillary (V2), and mandibular nerves (V3). Each division’s terminal branches allow for peripheral nerve blocks to deliver the necessary analgesia (Supplemental Figure 1). 1
Ophthalmic Division (V1)
The ophthalmic division (V1) arises from the anterior part of the trigeminal ganglion and divides, as it passes through the cavernous sinus, into lacrimal, frontal, and nasociliary nerves. V1 provides sensory innervation to the face through the following terminal branches: (a) supraorbital and supratrochlear nerves (branches of the frontal nerve) supplying the upper eyelid and medial aspects of the forehead; (b) the infratrochlear nerve (a branch of the nasociliary) innervating the upper medial aspect of the eyelid inferior to the eyebrow; and (c) the external nasal branch of the anterior ethmoidal nerve, which provides sensory innervation to the medial part of the nares.1,5
Maxillary Nerve (V2)
The maxillary nerve (V2) originates from the posterolateral part of the trigeminal ganglion. Then, it travels through the cavernous sinus and exits the cranium at foramen rotundum. It gives off 3 branches at the pterygopalatine fossa: the palatine, nasal, and zygomatic nerves. The terminal branch then enters the orbit through the inferior orbital fissure as the infraorbital nerve. Then, it exits the orbit through the infraorbital foramen and gives off the external nasal, internal nasal, labial, and palpebral branches. The palpebral branch provides innervation to the lower eyelid and conjunctiva by the medial and lateral branches. Prior to exiting the orbit, the zygomatic nerve divides into the zygomaticotemporal and zygomaticofacial nerves. The zygomaticotemporal nerve then exits the orbit via the zygomaticotemporal foramen and supplies the skin of the lateral temple. The zygomaticofacial nerve exits the orbit via the zygomaticofacial canal and supplies the lateral cheek and lateral lower eyelid.5-7
Mandibular Nerve (V3)
The mandibular nerve (V3) exits the cranium inferiorly through foramen ovale, where it gives off the anterior and posterior divisions. The posterior division then divides into the inferior alveolar, lingual, and auriculotemporal nerves. The mental nerve is the terminal branch of the inferior alveolar nerve and provides sensation to the anterior mandible. The sublingual nerve is the terminal branch of the lingual nerve providing sensation to the buccal mucosa. The auriculotemporal nerve supplies sensation to the tragus and helix of the ear, the external portion of the tympanic membrane, the posterior temporomandibular joint, and the temple.1,5
Supraorbital and Supratrochlear Nerves Blocks
Anatomy and Sensory Distribution
The supraorbital and supratrochlear nerves are the terminal branches of the ophthalmic division of trigeminal nerve. V1 first gives off the lacrimal, frontal, and nasociliary branches, then the frontal nerve further splits into the supraorbital and the supratrochlear nerves. The supraorbital nerve exits the skull through the supraorbital foramen where it splits into the palpebral nerve to the upper eyelid, and travels toward the forehead giving off medial and lateral branches to the frontal scalp up to the lambdoidal suture. The supratrochlear nerve travels more medial through the supraorbital notch. These 2 branches provide the sensory supply to the frontal scalp and forehead, the medial part of the upper eyelid, and the root of the nose (Figure 1).5,8
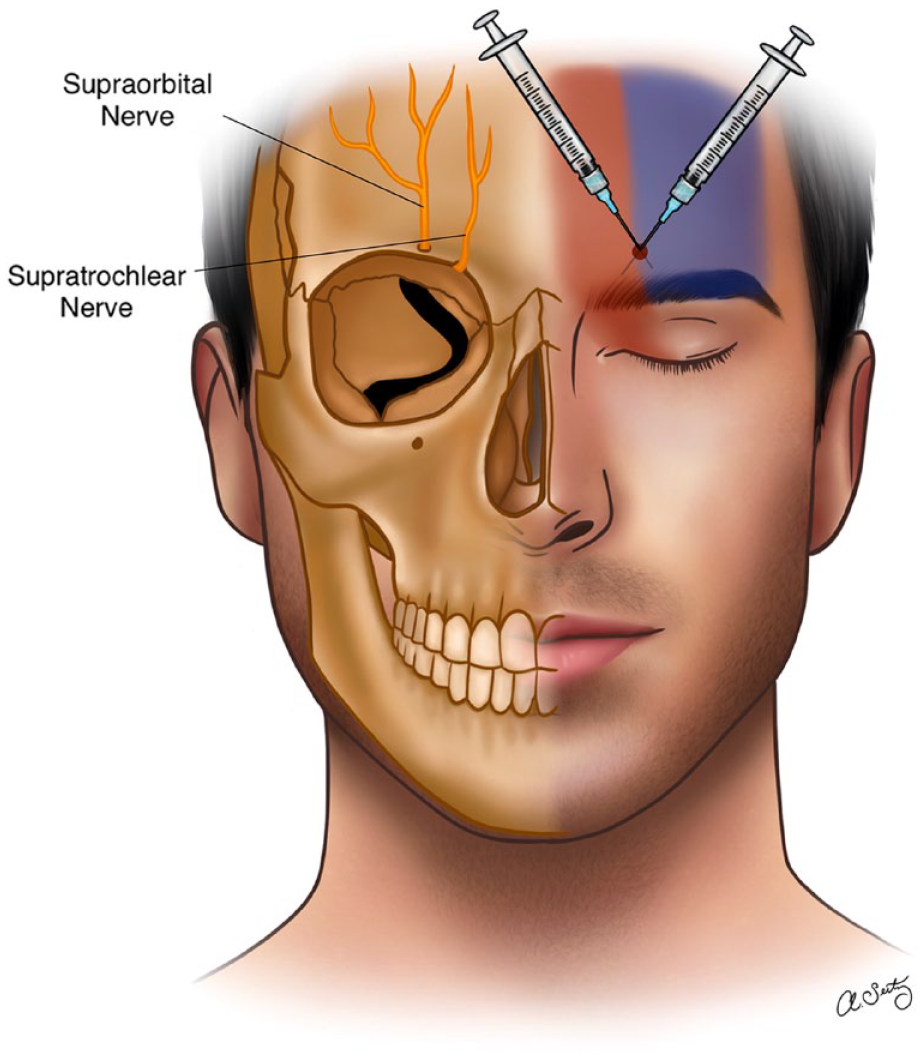
The right side of the face demonstrating supraorbital (exiting via the supraorbital foramen) and supratrochlear (exiting via the supraorbital notch). The left side of the face demonstrates supraorbital (blue) and supratrochlear (red) area of innervation.
Technique
The classical technique for performing a supraorbital nerve block involves locating the supraorbital foramen, which can be easily felt by running your finger along the orbital rim at 2 cm from the midline in adults (junction of the medial one-third and the lateral two-thirds of the orbital rim). For a supratrochlear nerve block, the landmark is at the top of the angle formed by the eyebrow and the nasal spine where the nerve is in contact with the bone. The supratrochlear nerve can be blocked immediately following supraorbital nerve block, without removing the needle, by directing the needle about 1 cm toward the midline and injecting an additional 0.5 mL of LA. After the injection, firm pressure should be applied for better anesthetic spread and prevention of ecchymosis.
Success Rate
Sato and Nishiwaki performed a retrospective study looking at the success of different nerve block in the scalp for patients undergoing awake craniotomy and found that supraorbital and supratrochlear nerve at a 97.6% success rate. 9
Maxillary Nerve Block
Anatomy and Sensory Distribution
The maxillary nerve is the second division of the trigeminal nerve. It arises from the anterior convexity of the trigeminal ganglion between the ophthalmic and mandibular divisions of the trigeminal nerve. Then it leaves the middle crania fossa through the foramen rotundum and courses forward through the roof of the pterygopalatine fossa. Finally, it enters the floor of the orbit via the inferior orbital fissure and exits through the infraorbital foramen as the infraorbital nerve (Supplemental Figure 1).1,10,11
Techniques
Three techniques are available to achieve a maxillary nerve block: the high tuberosity, greater palatine canal, and coronoid approaches. In the high tuberosity approach, the nerve is targeted as it travels via the pterygopalatine fossa. A needle is inserted with a 45° angle at the highest point of the mucobuccal fold distal to the second maxillary molar teeth, then advanced posteriorly, superiorly, and medially within the fossa. Negative aspiration for blood is confirmed to avoid injury of the maxillary artery, then LA is slowly injected. The greater palatine canal approach blocks the maxillary nerve as it travels via the pterygopalatine fossa which is located at 1 cm medial and adjacent to the second molar teeth. A 25-gauge long needle is inserted perpendicularly in front of or around the greater palatine foramen. If resistance is faced, the needle can be reinserted at a different angle, however if the canal cannot be approached, this approach is abandoned. In the coronoid approach, the access is external where the coronoid notch of the mandible is identified while the patient opens and closes the mouth and palpating in front of and below the tragus. A 22-gauge long needle is advanced perpendicular to the skin at the center of the coronoid notch below the zygomatic arch. At 4 to 5 cm depth, the lateral pterygoid plate can be identified. Then, the needle is redirected anteriorly and superiorly, and advanced to a 1 cm depth, block of the maxillary nerve can be achieved while if the needle is withdrawn by 2 mm, the block can also include the mandibular nerve. To avoid damaging the branches of the external carotid artery (eg, internal maxillary artery), the needle must be handled carefully.11-13
Success Rate
In a study performed in 2013, maxillary nerve block was compared to superior alveolar and infraorbital nerve blocks. The success rate for maxillary nerve block was reported to be 85% and showed to be effective in providing anesthesia for oral surgery. 14
Infraorbital Nerve Block
Anatomy and Sensory Distribution
The infraorbital nerve is the largest branch of the maxillary nerve. It arises as a terminal branch of the maxillary nerve at the floor of the orbit then travels through infraorbital canal to exit on the face via the infraorbital foramen. It provides cutaneous innervation to medial cheek, lateral nose and nostrils, lower eyelid, and upper lip. Besides, V2 supplies sensory innervation to the dura of the middle cranial fossa, the upper molars, premolars, incisors, canines, and related oral gingiva; mucous membranes of the maxillary sinuses and nasal cavity; and hard and soft palate (Figure 2).1,10,11
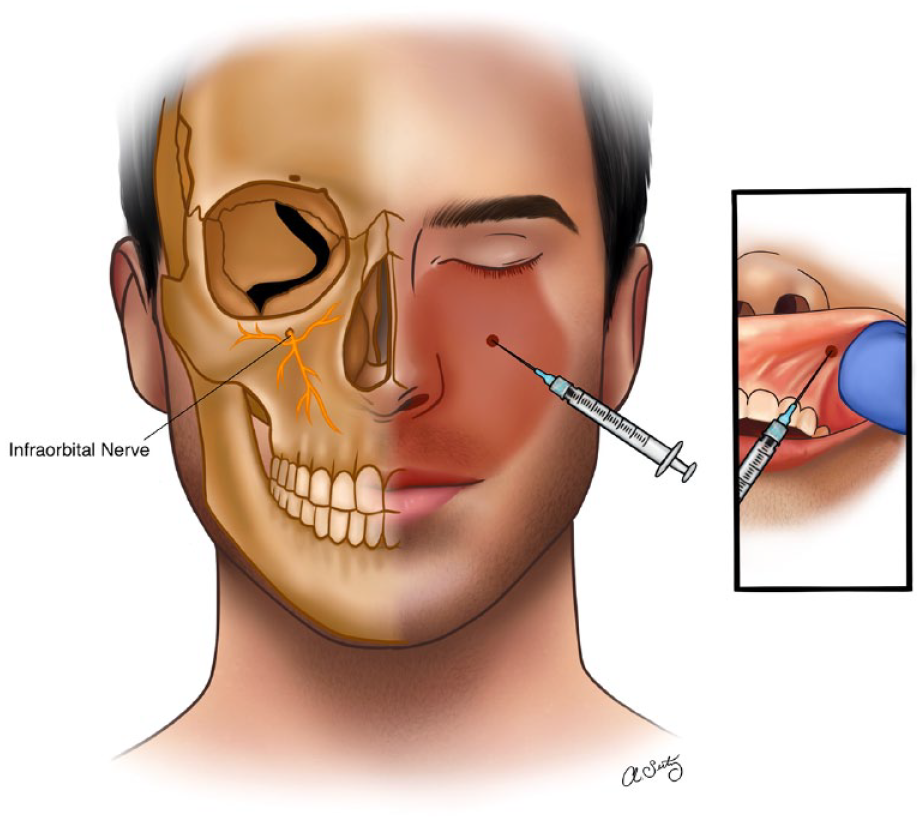
The right side of the face demonstrating infraorbital nerve as it exits the infraorbital foramen. The left side of the face demonstrates infraorbital nerve area of innervation.
Techniques
The main anatomical landmarks include infraorbital ridge and infraorbital foramen. Two approaches can be followed: extraoral or intraoral. In the extraoral approach, the infraorbital foramen is palpated, the needle is introduced through the skin cranially just below the palpation point until bone contact is made and then withdrawn slightly. In the intraoral approach, the center of the infraorbital ridge is palpated and marked with the middle finger. The upper lip is raised with a spatula or with the thumb and index finger. The needle is introduced through the mucosa above the second premolar tooth toward the infraorbital foramen, until bone contact is made, and then withdrawn slightly. In both techniques, slow injection of the LA should only be carried out after careful aspiration, followed by a thorough compression to prevent hematoma formation and to obtain better distribution of the LA. No injection should be applied to the infraorbital canal to avoid nerve injury. Also, care must be taken to ensure that the needle does not go too far and injure the globe, particularly in children where the maxilla is quite short.11-13
Success Rate
Atila assessed the effectiveness of infraorbital block in open septorhinoplasty surgery and found that patients who received infraorbital block had significantly lower postoperative pain compared to the control group. 15
Inferior Alveolar Nerve Block (IANB)
Anatomy and Sensory Distribution
The inferior alveolar nerve is a branch of the posterior division of the mandibular nerve—the largest division of the trigeminal nerve. It provides sensory innervation to the lower lip, chin, teeth, gums, and the anterior two-thirds of the tongue. It originates at the brainstem and travels via the foramen ovale along the inferior border of the mandible and enters the mandibular foramen, where it divides into the mental and incisive nerves. The mental nerve supplies the skin of the chin and lower lip, whereas the incisive nerve supplies the teeth and gums (Figure 3).10,16-18
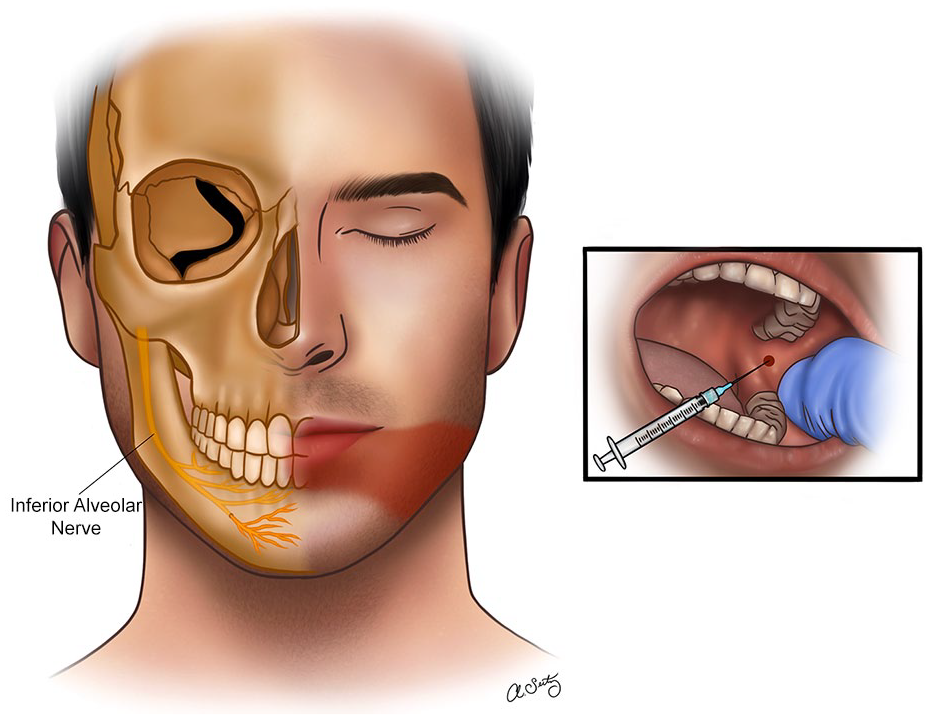
The right side of the face demonstrating anatomical location of the inferior alveolar nerve. The left side of the face demonstrates inferior alveolar nerve area of innervation.
Techniques
The conventional technique involves the insertion of the dental needle where the inferior alveolar nerve enters the mandibular foramen. The anatomical landmarks that should be recognized by the operator include the coronoid process and notch, the anterior and posterior border of the mandible, the sigmoid notch, and the condyle. Orthopantomogram radiographs can help locate the mandibular foramen and the bony landmarks used in the IANB. The coronoid notch and the pterygomandibular raphe are the 2 most significant clinical landmarks utilized in the IANB. Between these 2 landmarks is the optimal location for needle insertion. The insertion site is on a hypothetical line that is traced from the coronoid notch to the deepest portion of the pterygomandibular raphe. 13 Several alternative approaches have been described for the IANB, which aimed to achieve a higher success rate, reduce the risk of intravascular injections and nerve damage.16,19-22
In the Gow-Gates technique, instead of injecting near the pterygomandibular raphe, the needle is directed in a more posterior and superior trajectory (latero-anterior surface of the condyle). 23 In contrast, in the Vazirani-Akinosi technique, the injection is made in a more anterior and lateral direction. The needle is inserted from the opposite side of the mouth (contralateral) and aimed toward the mandibular foramen. This method can be valuable when patients have limited mouth opening, as it does not necessitate wide access to the injection site. 24
Success Rate
It is important to acknowledge that IANB may not consistently deliver full anesthesia and can exhibit a failure rate in certain instances. Research and clinical observations have indicated that the effectiveness of IANB can vary, ranging from around 70% to 85% in achieving deep anesthesia in the lower jaw’s teeth. Several factors can contribute to IANB’s ineffectiveness, including the presence of accessory nerve pathways, patient anxiety or stress, anatomical variations, and conditions related to inflammation in the nerve or target tissues. 25
Lingual Nerve Block
Anatomy and Sensory Distribution
The lingual nerve emerges from the infratemporal fossa and crosses the tensor veli palatini. It also passes by pterygoid muscles (lateral, medial & anterior), and routes toward the mandibular ramus. Then lingual nerve enters the mouth, then it passes underneath the superior constrictor muscle in the close vicinity to the pterygomandibular attachment. This space is significant due to the presence of mandibular molars. Then lingual nerve moves anteriorly further and continues the track by turning medially to reach the tongue. It covers the floor of the mouth, and its branches supply the lingual gingiva.5,26-28
Techniques
For lingual nerve block, the point of insertion is distal to mandibular second molar and almost 6 mm away from the gingival margin. The site of injection is about 1 cm medial to the second mandibular molar. 29
Mental Nerve Block
Anatomy and Sensory Distribution
The mental nerve is a branch of the mandibular division of the trigeminal nerve and is responsible for innervating the skin and mucosa of the lower lip, chin, and skin over the lower jaw. It is a purely sensory nerve and does not have any motor function. The mental nerve arises from the mandibular nerve and exits via the mental foramen about 2 cm below the second mandibular premolar (Figure 4).1,30
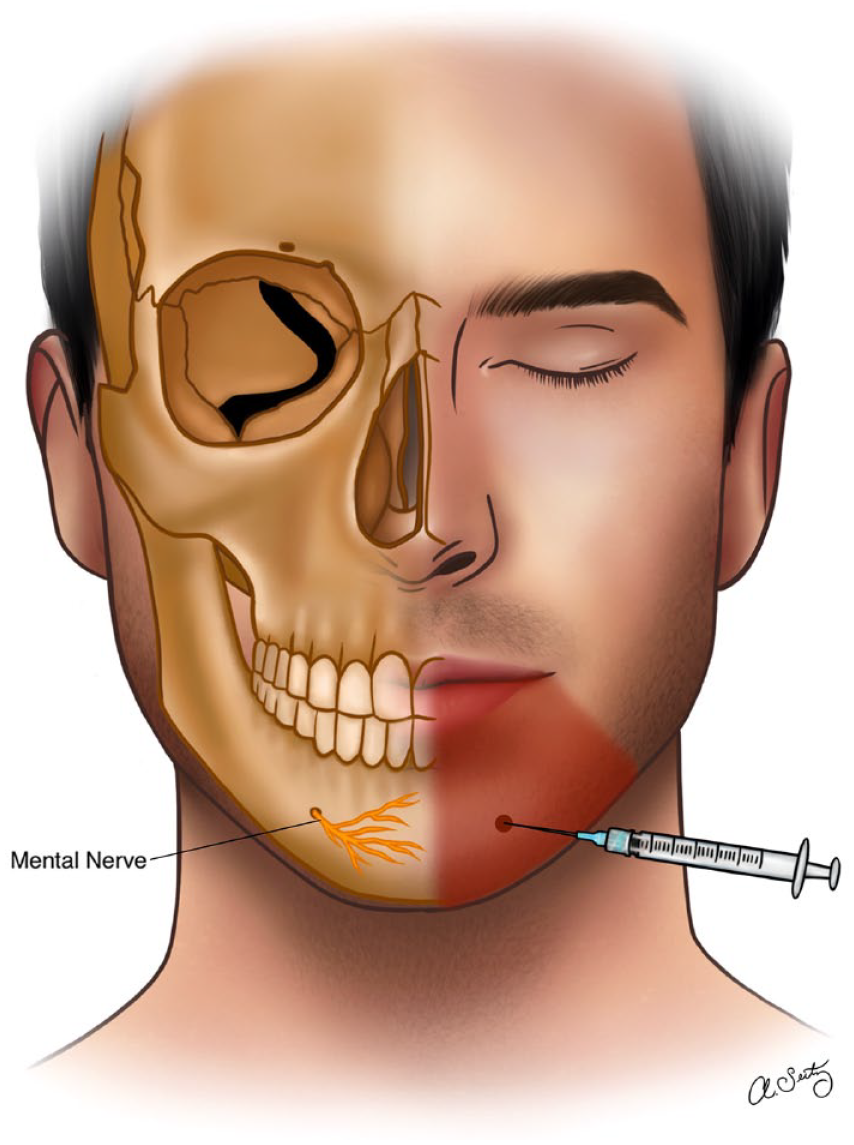
The right side of the face demonstrating mental nerve as it exits the mental foramen. The left side of the face demonstrates mental nerve area of innervation.
Techniques
The infiltration technique involves injecting the LA directly into the tissue surrounding the mental foramen, about 2 cm below the second mandibular premolar. This technique is simple and easy to perform and does not require any special equipment. However, it may be less reliable than other techniques and may not provide complete anesthesia.31-34
Field Blocks
Due to innervation by several branches of the trigeminal nerve, the nose requires more careful consideration for getting adequate anesthesia. Similarly, the ear received innervation from the vagus and spinal nerves. The following section describes techniques in performing field block for the nose and the ear.
Nose Blocks
Anatomy and Sensory Distribution
The nose is innervated by the ophthalmic, maxillary, and mandibular divisions of the trigeminal nerve. V1 provides sensory innervation to the upper part of the nasal septum and lateral nasal wall. V2 provides sensory innervation to the nasal vestibule and the lower part of the nasal septum. V3 provides sensory innervation to the ala nasi and the nasal vestibule. The posteroinferior half of nasal septum mucosa is innervated by the nasopalatine nerve, a branch of the maxillary nerve, which enters the nasal cavity through the sphenopalatine foramen and innervates nasal septum filaments. The superoanterior half of nasal septum mucosa is innervated by anterior ethmoidal nerves, branches of the nasociliary nerve from the ophthalmic nerve. Superiorly, the nasal septum mucosa is innervated by the olfactory nerve, with nerve endings traversing the cribriform plate through multiple tiny foramina. Besides, the nose is innervated by the sympathetic and parasympathetic branches of the autonomic nervous system. The sympathetic branches, which originate from the thoracic spinal cord, provide innervation to the vasculature of the nose and play a role in the regulation of blood flow and nasal secretions. The parasympathetic branches, which originate from the cranial nerves, provide innervation to the glands and smooth muscle of the nose and play a role in the regulation of nasal secretions and mucociliary clearance (Figure 5).5,6,18,35
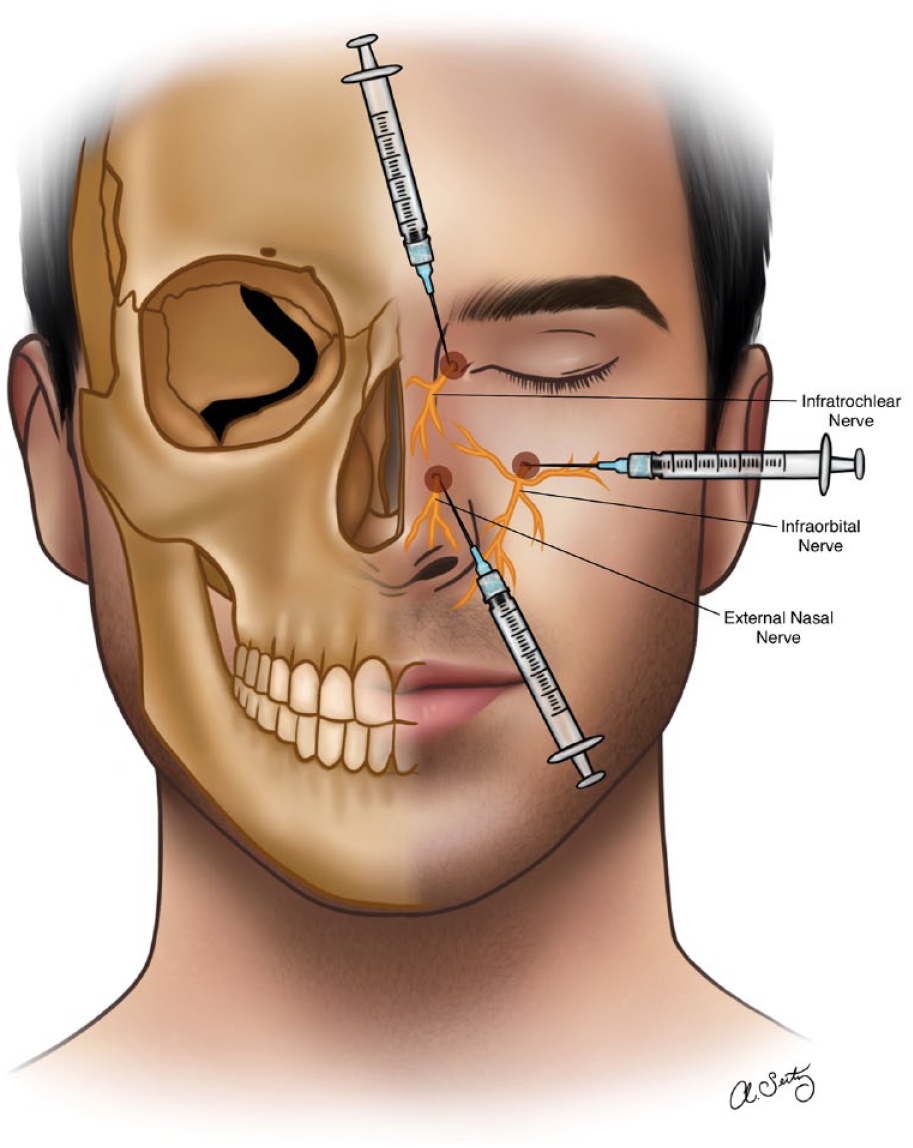
Innervation of the nose via the branches of the ophthalmic (V1), maxillary (V2), and mandibular nerves (V3).
Techniques
There are several different approaches to nerve blocks of the nose, including topical, intradermal, subcutaneous, and intranasal injections. The choice of approach depends on the specific nerve or nerves being targeted and the purpose of the block. One common technique for a nerve block of the nose is the topical approach, which involves the application of a LA cream or gel to the skin overlying the nerve or nerves being targeted. Despite its proven anesthetic and vasoconstrictive effects, cocaine may also be a viable alternative, however, it is limited because of its increasing costs, abuse potential, side effects, and availability restrictions. 36
The second technique for a nerve block of the nose is the intradermal approach, which involves the injection of a LA into the skin overlying the nerve or nerves being targeted. This approach is generally used for superficial nerves, such as the infraorbital nerve, and is less commonly used for deeper nerves, such as the sphenopalatine ganglion. 37
A third technique is regional anesthesia which can be performed on each side by blocking the infraorbital nerve and nasal branches of the nasociliary nerve. To block the nasociliary nerve or its branches, a 3 cm, 25-gauge needle is inserted 1 cm above the inner canthus and directed posterolaterally, keeping contact with bone. At a depth of 1.5 cm the needle should be at the anterior ethmoidal foramen, and 2 mL of LA is then injected. The needle is then advanced slowly 1 cm further to reach the posterior ethmoidal foramen where 1.5 mL of solution is injected to block the posterior ethmoidal nerve that supplies the posterior sinuses. The 2 injections can also be likely to block another branch of the nasociliary nerve, the infratrochlear nerve which supplies the root of the nose. An oral approach to block the infraorbital nerve involves palpating the infraorbital foramen, inserting a needle in the mucobuccal fold along the axis of the bicuspid tooth, and injecting an anesthetic solution without entering the canal.1,38
A fourth technique for a nerve block of the nose is the intranasal approach, which involves the injection of a LA directly into the nasal cavity. This approach is generally used for nerves within the nasal cavity, such as the nasociliary nerve, and is less commonly used for nerves outside the nasal cavity, such as the infraorbital nerve.1,38,39
Auricular Blocks
Anatomy and Sensory Distribution
The ear is innervated by several nerves, including the auricular branch of the vagus nerve and the great and lesser auricular nerves, arising from the C2/C3 spinal nerves. The auricular branch of the vagus nerve provides sensory innervation to the posterior and superior aspects of the ear, including the concha and the crus of the helix. The great auricular nerve provides sensory innervation to the anterior and inferior aspects of the ear, including the lobule and the tragus, whereas the lesser auricular provides innervation to the upper and medial third of the auricle (Figure 6).5,6,18
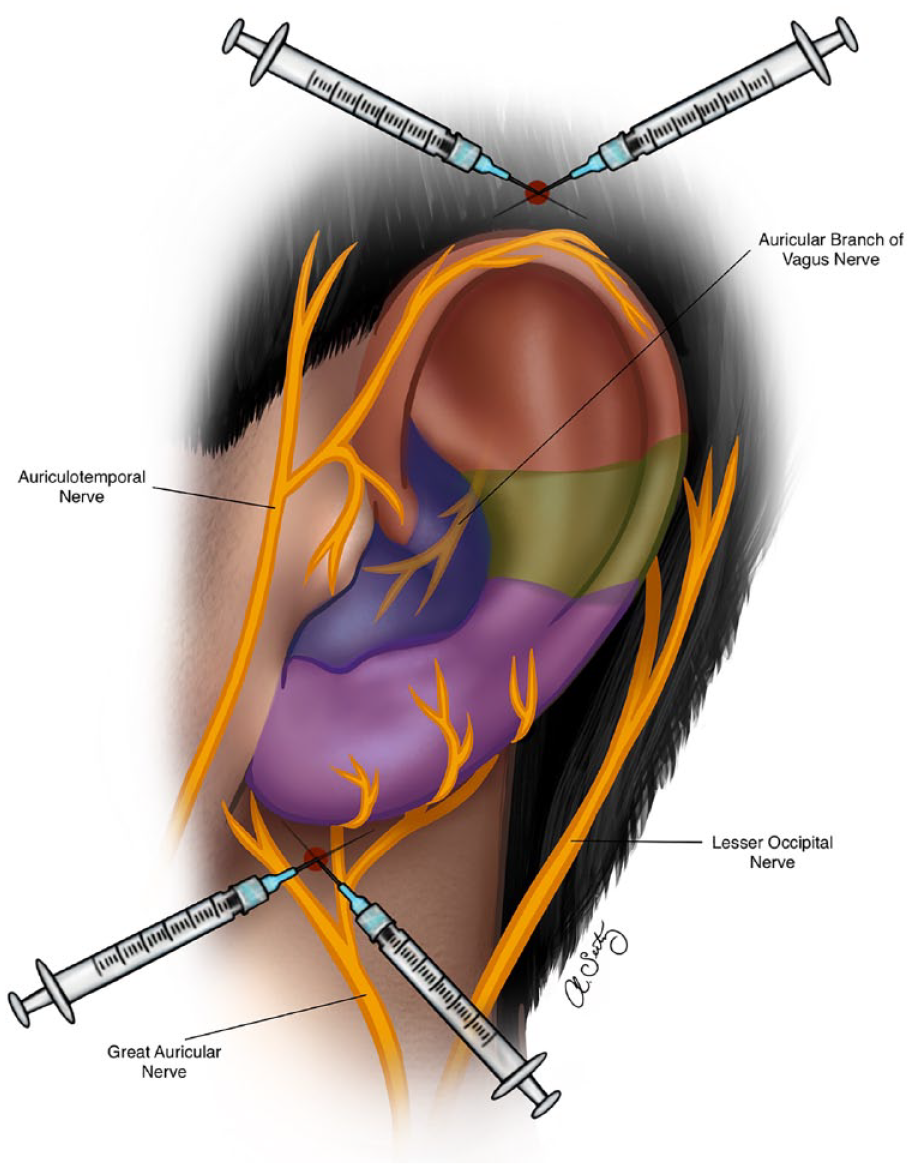
Innervation of the nose via the branches of the vagus and greater auricular nerves.
Techniques
The classical techniques for regional field nerve block can be used to block the sensory innervation of the external ear, except the posterior wall of the external auditory meatus (ie, Ramsay Hunt area). Regional nerve block can be performed by injecting a LA solution above the posterior portion of the zygoma, anterior to the ear and behind the superficial temporal artery using a 27-gauge needle. The greater auricular nerve and the lesser occipital nerve can be blocked distally over the mastoid process posterior to the ear, by inserting the needle behind the lower lobe of the ear and advancing it following the curve of the posterior sulcus. Additionally, a ring nerve block technique can provide efficient analgesia of the external ear. This nerve block is done by everting the tragus, inserting a 30-gauge needle, and injecting 0.2 mL of LA solution after aspiration. The steps of the traditional ring block is described elsewhere by Kravchik et al.3,17,40
Types of Local Anesthetics
LAs are divided into 2 major categories: Amino Amides and Amino Esters. Common drugs within the amino amides include lidocaine, bupivacaine, and mepivacaine. Procaine, cocaine and tetracaine on the other hand belong to the amino esters. Both categories work by blocking the voltage-gated sodium channels to prevent sodium influx into the cells leading to signal transmission blockage. Amino amides are found to be stable in solution, whereas amino esters are unstable leading to higher risk of allergic and hypersensitivity reactions. Amino amides are metabolized in the liver compared to amino esters that are metabolized by plasma cholinesterase. Given the lower risk of allergic and hypersensitivity reactions, amino amides are commonly used for LA, with lidocaine and bupivacaine being the most common options. 41
Complications
Needle-Induced Tissue and Vascular Injuries
Nerve block causes tenderness and bruising, but rarely significant. Needle-induced vascular injury, including hematomas and microvascular injuries, can lead to nerve injury, vascular insufficiency, fistula, or pseudoaneurysm formation. 42
Nerve Injury and Neurotoxicity
Nerve injury following peripheral nerve blocks is rare nerve injury, with an estimated the incidence of long-term injury occurring 2.4 to 4 per 10 000 blocks, while the transient sequalae occur 8.2% to 15%. 43 Several mechanisms were described, including needle-induced transection, pressure-induced ischemic injury (particularly with intraneural injection), compression by hematoma (intraneural or extraneural), LA-induced toxicity, vascular compromise due to direct vascular injury, prolonged vasoconstriction, and needle-induced endoneural herniation. At the cellular level, the neurotoxicity of LAs is caused by the effect on the intrinsic caspase-pathway, PI3k-pathway, and MAPK-pathways.42,44,45 For example, immediate and delayed facial nerve palsy are common after inferior alveolar anesthesia, with immediate types involving needle trauma, air blast, hematoma formation, or infiltration. Delayed facial nerve palsy may result from viral infection reactivation, axonal ischemia, excessive stretching, or inadvertent intra-arterial injection.46-48
Ocular complications following IANB have been reported, with an estimated incidence of 0.03% to 0.13%. The most frequently reported complications are diplopia, ptosis, and mydriasis. Common causes include back pressure, perivascular trauma, or local diffusion of LA.49-51 Furthermore, a recent case-report described, for the first time, transient glossopharyngeal nerve palsy (nasal speech, numbness around external auditory meatus, and Uvula deviation) following mandibular nerve block by LA administration in the right pterygomandibular space. 52
Systemic Toxicity
Local anesthetic systemic toxicity (LAST) is the most severe complication of LA use primarily affecting the central nervous system (CNS) or the cardiovascular system (CVS). However, the CNS toxicity occurs at lower plasma concentrations than CVS toxicity. The incidence of LAST is reported in recent literature as low as 2 to 2.8 per 10 000 peripheral nerve blocks, whereas 36% had minor symptoms, 14% reported moderate symptoms, 3.5% reported severe symptoms, and 0.4% died. Pharmacological risk factors for LAST include the specific LA agent and the total dose administered. The cardiovascular-collapse-to-CNS ratio is an important pharmacologic factor, as agents with lower ratios are associated with earlier cardiotoxicity. Patient-related factors include extremes of age, and mitochondrial dysfunction. Medication administration factors include the site of administration. For example, intravascular injection or administration in a highly vascular sites increases the risk due to more rapid plasma uptake and systemic absorption. Ultrasound guidance has been associated with a reduced risk of LAST.53,54
Early recognition and intervention with supportive measures and intravenous lipid emulsion 20% (particularly for patients with seizures or severe cardiotoxicity), are the mainstays of treatment. The mechanism of action for treatment of LAST is unclear, but literature showed that it may improve sodium channel function, mitochondrial metabolism, and fatty acid processing.55,56
Methemoglobinemia
LAs have the potential to cause oxidative damage to hemoglobin, resulting in the formation of methemoglobin. Benzocaine and prilocaine are the agents most associated with the development of methemoglobinemia. Methemoglobinemia should initially be treated symptomatically, while in severe cases, methylene blue and hyperbaric oxygen may be used.57,58
Allergic Reactions
Two allergic reactions to LAs have been described. First, immediate reactions (immunoglobulin E-mediated Type 1 hypersensitivity) which manifested as urticaria or systemic anaphylaxis (eg, dyspnea, cough, wheezing, hypotension, and tachycardia). The prevalence of true immunoglobulin E-mediated allergy to LAs is estimated to be lower than 1%. Second, delayed hypersensitivity reaction which includes allergic contact dermatitis. It is uncommon but well-established and peaks within 72 hours, with an estimated incidence up to 3.4%. The treatment of immediate reactions relies on immediate intravenous vasoconstrictors (epinephrine), while antihistamines are the mainstay of delayed type reactions.57,59-61
Local Anesthetic Toxicity
Most LAs show similar symptoms, but their neurotoxicity to cardiotoxicity ratio may differ, with bupivacaine being the most cardiotoxic. Bupivacaine has a slower onset of action (5-8 minutes) and longer duration than lidocaine (2-4 hours). Intravenous injection or rapid vascular uptake of bupivacaine is the most common reason for its toxicity. However, patients with l-carnitine deficiency may experience cardiac toxicity at low doses of bupivacaine. Methemoglobinemia is typically associated with benzocaine or prilocaine; however, case reports exist implicating bupivacaine in rare instances. Treatment for bupivacaine toxicity include supportive measures like cardiopulmonary resuscitation and GABA agonists, however, lipid emulsion became widely accepted as a first-line treatment for patients with LAST.57,62,63
Discussion
Facial nerve blocks represent a crucial element in managing pain and anesthesia for a wide range of medical and dental procedures involving the face and the scalp. These blocks mostly target the facial nerve, which governs the muscles responsible for facial expressions, and they serve both diagnostic and therapeutic purposes. Various methods exist for performing nerve blocks in the face, including the supraorbital, supratrochlear, infraorbital, inferior alveolar, lingual, and mental nerve blocks, each targeting specific branches of the facial nerve. Typically, these blocks involve the administration of LA close to the location of the nerve. Achieving precise needle placement is essential to ensure successful anesthesia while minimizing the potential for complications. Although nerve blocks are generally considered safe when administered by experienced practitioners, there is a possibility of inadvertent injection into a blood vessel or damage to nearby structures. Potential common complications encompass temporary facial muscle weakness, the formation of hematomas, and infection at the injection site.
The duration of anesthesia induced by nerve blocks varies depending on the technique employed and the type of LA utilized. In many instances, the effects are temporary and dissipate within a few hours, rendering them suitable for brief procedures. Proficiently executed facial nerve blocks can markedly enhance patient comfort during facial procedures, and alleviating pain and anxiety.
In facial surgery, both local and regional anesthesia can be used for craniofacial and esthetic procedures such as rhinoplasty, forehead lifts, eyelid surgery, chin augmentation, facelifts, and neck lifts. Additional facial procedures that can be done under LA include brow lift, cheek augmentation, lip augmentation, jawline contouring, and ear reshaping. The type of anesthesia used will depend on the complexity of the procedure and the patient’s individual needs and preferences. Surgeons should be well educated about the use of the regional blocks and their indications, techniques, and complications.
Conclusions
In summary, facial nerve blocks constitute invaluable tools across a spectrum of medical and dental specialties. When administered with precision, they can deliver effective pain relief and elevate patient comfort during facial procedures. However, their safe and precise execution necessitates an in-depth comprehension of facial anatomy and meticulous technique to mitigate potential complications.
Supplemental Material
sj-docx-1-fac-10.1177_27325016231217153 – Supplemental material for Nerve Blocks Utilized in The Face: A Comprehensive Review
Supplemental material, sj-docx-1-fac-10.1177_27325016231217153 for Nerve Blocks Utilized in The Face: A Comprehensive Review by Joshua Kohan, Armin Edalatpour, Allison J. Seitz, Daniel Y. Cho and Brian H. Gander in FACE
Supplemental Material
sj-docx-2-fac-10.1177_27325016231217153 – Supplemental material for Nerve Blocks Utilized in The Face: A Comprehensive Review
Supplemental material, sj-docx-2-fac-10.1177_27325016231217153 for Nerve Blocks Utilized in The Face: A Comprehensive Review by Joshua Kohan, Armin Edalatpour, Allison J. Seitz, Daniel Y. Cho and Brian H. Gander in FACE
Supplemental Material
sj-jpg-3-fac-10.1177_27325016231217153 – Supplemental material for Nerve Blocks Utilized in The Face: A Comprehensive Review
Supplemental material, sj-jpg-3-fac-10.1177_27325016231217153 for Nerve Blocks Utilized in The Face: A Comprehensive Review by Joshua Kohan, Armin Edalatpour, Allison J. Seitz, Daniel Y. Cho and Brian H. Gander in FACE
Footnotes
Acknowledgements
None
Author Contributions
Joshua Kohan, BA—study design, data acquisition, preparation of tables, writing the manuscript, critical review and approval of the manuscript, accountability for the contents of the manuscript. Armin Edalatpour, MD—study design, critical review and approval of the manuscript, accountability for the contents of the manuscript. Allison J. Seitz, BS—preparation of figures, critical review and approval of the manuscript, accountability for the contents of the manuscript. Daniel Y. Cho, MD—critical review and approval of the manuscript, accountability for the contents of the manuscript. Brian H. Gander, MD—study design, critical review and approval of the manuscript, accountability for the contents of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Ethical Approval
Institutional Review Board approval was not required.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.