
Abstract
Cubital tunnel syndrome is the second most common compressive neuropathy of the upper limb. Endoscopic cubital tunnel decompression has gained popularity in recent years as this enables surgeons to achieve decompression of the ulnar nerve along its course using a small incision. This article describes the technical peals in performing endoscopic cubital tunnel decompression. In conditions which anterior transposition of the ulnar nerve is needed, subcutaneous transposition can be performed under endoscopic guidance. In addition, current literature is reviewed, and outcomes are presented. While short term results are encouraging, further prospective randomized study with longer follow-up is recommended.
Keywords
Introduction
Cubital tunnel syndrome is the second most common compressive neuropathy of the upper limbs, following carpal tunnel syndrome. It has an incidence of 25 cases per 100,000 person per year. 1 It is a compressive neuropathy of the ulnar nerve around the medial aspect of the elbow, with the potential sites of compression being (from proximal to distal): Arcade of Struthers (8–10 cm proximal to medial epicondyle), medial intermuscular septum (especially if the nerve is needed for transposition), osteophytes of medial epicondyle, cubital tunnel retinaculum (also known as Osbourne’s ligament), anomalous anconeus epitrochlearis muscle, and the deep fascia of the flexor carpi ulnaris muscle (which may extend to 6–8 cm distal to medial epicondyle) 2 (Figure 1).
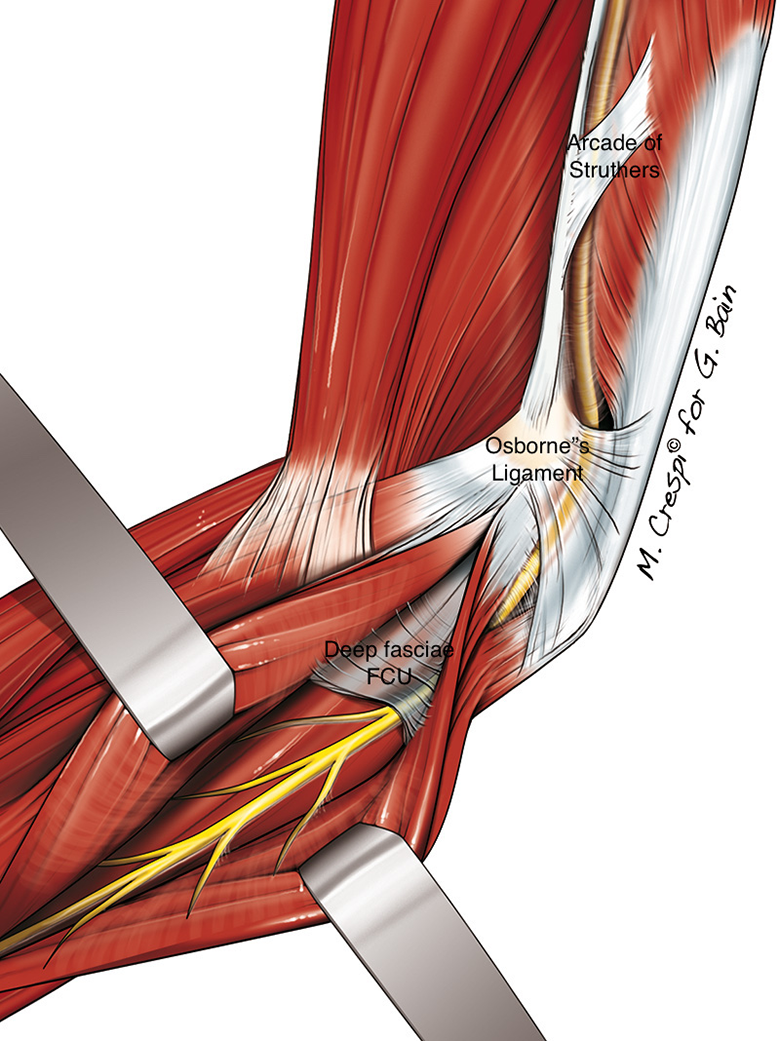
Potential sites of ulnar nerve compression in cubital tunnel syndrome (copyright Professor Greg Bain and Mr Max Crespi).
Surgical intervention for cubital tunnel syndrome is indicated if the patients maintain to have persistent symptoms after a period of conservative treatment or if they present with severe motor or sensory deficit. Open decompression and anterior transposition of the ulnar nerve used to be the gold standard for the treatment of cubital tunnel syndrome. 3 Yet, four prospective randomized studies 4 –7 comparing decompression and anterior transposition with open decompression in situ, showed that both techniques had similar recovery and functional outcomes. In addition, with the decompression in situ group 4,6 revealing significant lower complication rate, the trend has shifted from open decompression and anterior transposition to open decompression in situ. 8 –10
In recent years, endoscopic cubital tunnel release has gained popularity. 11 It allows surgeons to decompress the ulnar nerve along its route of all potential sites of compression under endoscopic guidance, with a smaller incision than that used in open decompression in situ (i.e. 2 cm as opposed to 4 cm). 12
Currently there are different instruments which are dedicated for cubital tunnel release in the market. It can be classified into 2 types: the use of specialized dissecting equipment: Storz instruments (Karl Storz, Tuttlingen, Germany) 13,14 (Figure 2), and Agee device (3M, Orthopedic Products, St Pauls, MN, USA) 15,16 and the use of cannula (Integra LifeSciences, Plainsboro, NJ, USA) 17,18 (Ace Glass company, Louisville, KY, USA) 19 (Figure 3). In this article, we are going to describe the technique of using Storz instruments in the endoscopic cubital tunnel release in situ as well as anterior transposition.

Endoscopic view of distal release using endoscope and specialized dissection equipment. Inlet: instrument used (copyright Professor Greg Bain).

Illustration of endoscope and cannula in place (copyright Dr Tyson Cobb).
Endoscopic cubital tunnel decompression in situ
Indications
Symptomatic idiopathic cubital tunnel syndrome who are unresponsive to conservative care, preferably confirmed by nerve conduction study.
Contraindications
The presence of mass or space occupying lesion around the elbow, leading to ulnar nerve compression.
Patient with concomitant condition necessitating open surgery, e.g. humeral malunion or non-union.
Patient with severe elbow contracture.
Patient with previous trauma or surgery to the ulnar nerve.
Patient in which ulnar nerve decompression and anterior transposition is more indicated (refer to below: Indication for endoscopic ulnar nerve decompression and anterior transposition).
Patients with hypermobile ulnar nerve (refer to below: Hypermobility of ulnar nerve).
Hypermobility of ulnar nerve
Hypermobility of ulnar nerve remains to be a constant factor for debate on whether anterior transposition is needed. Conventionally, in the presence of ulnar nerve subluxation, concomitant ulnar nerve transposition at the time of surgical decompression is recommended. 9,10,20 –24 Interestingly Bartels et al. 4 who randomized 152 patients suffering from cubital tunnel syndrome into either simple decompression and anterior subcutaneous transposition, irrespective of the mobility of their ulnar nerve, demonstrated that there was no significant difference in clinical outcomes between two groups at 1 year follow-up. There was no significant increase in persistent symptoms and recurrence. These findings were substantiated by the findings of Cobb et al who found that post-operative resolution rates of pain (p = 0.69), numbness and tingling (p = 0.53) and satisfactory (p = 0.37) were not affected by the presence of preoperative ulnar nerve subluxation. 25
Nevertheless, recurrence of ulnar nerve cubital tunnel syndrome in the presence of ulnar nerve subluxation remains to be a concern for some authors. Krogue et al. 26 demonstrated that subluxation of the ulnar nerve was one of key factors for patients to undergo a revision surgery after simple ulnar nerve decompression. Meanwhile Cobb et al studied recurrence following endoscopic cubital tunnel release in 104 cases and found a recurrence in one case only (0.96%; 95% confidence interval 0.02–5.24). Recurrence rate following endoscopic release were not found to be higher than that of literature controls following open cubital tunnel release. 17
Among our authors, TKC only performs anterior transposition for instability if the instability is clinically symptomatic, while GB and MWM Fok perform anterior transposition if gross instability is found either preoperatively or intra-operatively.
Surgical techniques
An 1.5–2 cm incision is first made at the retro-condylar grove, between the medial condyle and olecranon. After dissecting through the subcutaneous tissue, the ulnar nerve is usually identifiable distal to the cubital retinaculum. It is important to avoid injuring the medial antebrachial cutaneous nerve in the subcutaneous plane as this may result in numbness around the surgical incision and the medial aspect of forearm. The cubital retinaculum is cut open under direct vision to decompress the ulnar nerve. A dissecting forceps is then used to develop a subcutaneous tunnel between subcutaneous tissue and fascia along the route of ulnar nerve (proximal extent: 10–12 cm proximal to the medial epicondyle; distal extent: 8–10 cm distal to the medial epicondyle). The surgeon should not encounter much resistant during this procedure and force should not be needed in the tunnel preparation.
During the decompression, the ulnar nerve should be kept under direct vision at all times. The ulnar nerve can be released from the Arcade of Struthers proximally (8–10 cm proximal to the medial epicondyle) and to the distal extent of the deep fascia of the branching of ulnar nerve to the flexor carpi ulnaris muscle (about 6–8 cm distal to the medial epicondyle). When the decompression is completed, the stability of the ulnar nerve is checked by taking the elbow in full range of movement. If the nerve is found to be subluxatable or dislocatable during elbow flexion, anterior transposition is recommended by GB and MWM. 21 –24 Prior to wound closure, hemostasis is obtained with long bipolar forceps. This is especially important in the presence of tourniquet use 13,19,27 –29 (Tables 1 and 2).
Case series of endoscopic cubital tunnel decompression.

* Wilson and Krout rating system, modified by Heithoff 1990. 54
Complex regional pain syndrome – CRPS.
Medial antebrachial cutaneous nerve – MABC.
Comparative studies of endoscopic cubital tunnel decompression with other techniques.

MABC: medial antebrachial cutaneous nerve.
VAS – Visual analogue scale score.
Pitfalls
There is a learning curve in mastering endoscopic techniques. It is recommended for surgeons to familiarize with all the instruments and tissue manipulation in a cadaveric lab.
A small incision may cause difficulty in visualization, which in turn result in iatrogenic injuries to either ulnar nerve proper or cutaneous nerves. It is recommended to use a larger incision especially in the first few cases and in overweight patients, until the surgeon is comfortable with the procedure
Injury to either the ulnar nerve proper or one of its branches may be resulted during decompression of the fasciae. It is important to keep the ulnar nerve in view at all times. Dissecting scissors is used to separate the nerve from the deep fasciae (i.e. ‘nick and spread’ technique) prior to the incision of the fasciae. If the endoscopic field is clouded (e.g. by blood) and cannot be cleared, convert to an open procedure should be considered.
Aggressive dissection and forceful insertion of the endoscopic instruments may lead to soft tissue damages and bleeding. If resistance is encountered during the insertion of the endoscope, all the instruments should be retrieved, and the subcutaneous tunnel should be checked
One of the recognized complications of endoscopic cubital tunnel release is hematoma formation 13,19,27 –29 (Tables 1 and 2). Tourniquet with no Esmarch is recommended for the procedure, as small vessels can be identified and be cauterized proactively. Long bipolar cautery is used (Figure 4). If needed, low suction can be used to clear out the smoke generated. If the endoscopic view is obscured by blood, one may need to extend the incision or convert it to an open procedure.

The use of bipolar cautery to achieve haemostasis (copyright Professor Greg Bain).
Endoscopic cubital tunnel decompression + anterior transposition
Indications
In conditions which anterior transposition is needed, e.g. the presence of hostile bed, ulnar nerve hypermobility (refer to the above on discussion), cubital valgus and previous incomplete ulnar nerve decompression, the procedure can still be done under endoscopic guidance by creating an additional volar portal. 21,35,45
Contraindications
Similar to endoscopic cubital tunnel release in situ
In addition, as this is a subcutaneous anterior transposition, in conditions like severe elbow contracture, previous trauma or surgery causing abundant scar around the elbow and in thin patients who predispose to ulnar nerve irritation, necessitating submuscular transposition, this technique is contraindicated.
Surgical techniques
In the initial stage of procedure, the ulnar nerve is decompressed in the usual manner, as described in the above section. Furthermore, the previously identified medial intermuscular septum (MIMS) during proximal dissection must be excised. MIMS has been known to be a potential site of impingement along the new course of the ulnar nerve if it is left intact.
An anterior subcutaneous space anterior to the medial epicondyle which the ulnar nerve will be placed after the transposition is developed by dissecting forceps or spatula. Then an additional subcutaneous volar portal, about 1 cm in length, is created just distal to the medial epicondyle (Figure 5). A nylon tape in introduced into this portal in order to aid the mobilization of ulnar nerve. The tape looped over the ulnar nerve, and its accompanied vessels. By having an assistant to pull on the tape gently, the nerve can be mobilized from the loose aerolar tissue under endoscopic guidance.

Additional portal for anterior transposition for ulnar nerve mobilization (copyright Professor Greg Bain).
Once the ulnar nerve is positioned into its ‘new’ course, anterior to the medial epicondyle, the entire course of the ulnar nerve is inspected again to ensure that there was no new site of compression or kinking of the nerve. A proximally based fascial sling from the flexor pronator muscle complex can be raised. By retracting the ulnar nerve anteriorly, i.e. between the fascial sling and the muscle bed, and suturing the sling onto the adjacent subcutaneous tissue, the nerve is being secured in its new course. Alternatively the subcutaneous tissue can be sutured to the rasped medial epicondyle in order to prevent the ulnar nerve from subluxing posteriorly during elbow movement. The stability of the nerve is checked again by taking the elbow to its full range of motion. Hemostasis is needed prior to the closure of the incisions to prevent the development of hematoma.
Pitfalls
Due to the close proximity of the ulnar nerve to the MIMS, nerve injury may be resulted during MIMS excision. An additional proximal incision can be made to retract the ulnar nerve from the MIMS prior to the excision (Figure 5).
Surgeons may devascularized the ulnar nerve by skeletonized the nerve from its accompanied vessels during the mobilization. This may affect the nerve recovery. It is recommended to mobilize the nerve together with its vessels.
Traction injury to the ulnar nerve may be resulted if the assistant retracts the nerve, by pulling on the nylon tape with excessive force. It is important to remind assistant to lift up, instead of pulling on, the nylon tape, which wraps around the nerve and accompanied vessels, with minimal force. The accompanied vessels would be engorged proximally if excessive force is applied. Cadaveric practice may be beneficial for new assistants.
New site of compression may be noted after transposition. It is important to inspect the new route for potential compression site and its stability.
Review of the current literature
Cubital tunnel decompression is a common procedure of which more than 50,000 were performed per year in United States. 8 It comprises of different techniques including open and endoscopic decompression, with and without transposition, and medial epicondylectomy. Endoscopic cubital tunnel decompression was first described by Tsai et al in 1995. 19 By using a 30° endoscope, ulnar nerve can be identified and released along its route, while preserving the vascularity of the ulnar nerve. Out of 112 patients, Tsai reported 87% excellent and good outcomes 46 (Table 3), with short return to work time, low recurrence and complication rate. Subsequent case series also showed similar results 13,16,27,30,31 (Table 1).
Bishop rating system. 46

Comparative studies and meta-analysis between endoscopic cubital tunnel decompression and open decompression
Numerous studies comparing endoscopic cubital tunnel decompression with open decompression were available in the literature (Table 2). Both the operative time 44 and the tourniquet time 42 were noted to be significantly longer (of an average of 5–10 min) for the endoscopic decompression as compared with the open decompression, likely due to the additional need of endoscopic equipment preparation and in some cases limited experience. The latter is suggested by the findings of Cobb et al who reported on 172 cases of endoscopic cubital tunnel release with a mean tourniquet time of 10 min (range 3–23). 25 While there was no significant difference in Bishop score 46 and patients’ subjective satisfaction between the two groups, 24,39 –44 the duration of post-operative pain and scar satisfaction were significantly in favour for endoscopic cubital tunnel decompression. There was no significant difference in the time to return to work for endoscopic and open decompression. 24,39 Yet there was a significant difference in the time to return to work when endoscopic decompression was compared with anterior subcutaneous transposition, i.e. 7 days vs. 71 days. 44 The overall complication rate for endoscopic cubital tunnel decompression was low compared with open cubital tunnel decompression. 24,44,40 Nevertheless, post-operative haematoma remained to be a significant complication in endoscopic cubital tunnel decompression and care should be taken to achieve good haemostasis intra-operatively. 24,25,40,43
Only one long-term multicentre study was available with an average follow-up of 92 months (range: 9–144 months), comparing endoscopic decompression with other techniques namely open decompression, anterior subcutaneous transposition and submuscular transposition. 41 The majority of these patient suffered from mild to moderate ulnar nerve palsy i.e. McGowan I and IIA. 47,48 There was no significant difference in subjective improvement between different techniques. Submuscular transposition appeared to have more recurrence (i.e. 5 out of 82 patients) compared with other techniques (i.e. 1 out of 44 patients in open decompression), but the number was too small to reach a statistically significant difference.
Numerous systematic reviews and meta-analysis comparing endoscopic cubital tunnel decompression and open decompression have been published in recent years (Table 4). Similar clinical outcomes could be achieved with the two techniques. Yet there were more overall complications associated with open decompression. 28,50 Scar tenderness and injuries to the medial antebrachial cutaneous nerve were associated with the open decompression while haematoma was associated with endoscopic decompression. 28,29
systematic review and meta-analysis of endoscopic cubital tunnel decompression with other techniques.

MABC: medial antebrachial cutaneous nerve.
VAS – Visual analogue scale score.
Results described as more, are significantly more.
Satisfaction is post-operative satisfaction.
Only statistically significant results are presented.
Endoscopic decompression and anterior transposition
There are only a few case series illustrating the outcome (up to 24 months) after endoscopic cubital tunnel decompression and anterior transposition (Table 5). Only Martin et al. 35 described the subjects of their study as patients with preoperative elbow discomfort or recurrence, requiring anterior transposition. The short term outcomes of endoscopic cubital tunnel decompression and anterior transposition was promising, with at least 75% achieving either good or excellent outcome. 35,52,53 Though the complication rate was low, hematoma and injury to the medial antebrachial cutaneous nerve remained to be the main complications. 35
Case series of endoscopic cubital tunnel decompression and anterior transposition.

MABC, Medial antebrachial cutaneous nerve injury.
Conclusion
Endoscopic decompression appears to be a promising technique in the management of cubital tunnel syndrome. It can achieve, comparable or superior clinical outcome as with open decompression and is associated with low complication rate and recurrence rate. Yet, there is a lack of well-designed study, preferably an adequately powered, double blinded, randomized controlled trial to compare endoscopic decompression with open decompression.
With the need of using endoscopic equipment, endoscopic decompression is associated a higher operative cost than open decompression. 11 Currently there is no study examining the cost effectiveness in open and endoscopic cubital tunnel decompression. If endoscopic decompression is associated with early return to work and low complication rate, an increase in the initial surgical cost may be justified.
Endoscopic decompression and anterior transposition is a relatively new concept. It is useful in cases which the native bed of the ulnar nerve is hostile, or the ulnar nerve is subluxatable. Yet, further study is needed to compare its outcome with different conventional anterior transposition.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.