
Abstract
Introduction
Ergonomics is the scientific discipline that analyzes human interactions with systems and integrates principles to optimize well-being and system performance. 1 The operating room is a fast-paced, demanding environment where surgeons must sustain non-neutral body positions, utilize heavy equipment, maintain prolonged focus, and make decisions under pressure. 2 Poor ergonomics, including awkward postures, have been associated with musculoskeletal (MSK) injuries in surgeons that prompt absenteeism, clinical practice modification, shortened careers, and burnout. 3 In turn, this burnout may increase the risk of medical errors and worsen the quality of patient care.2,4,5
Plastic surgery is a diverse surgical specialty encompassing procedures operating across the entire body. 6 Operating on certain anatomic sites may require surgeons to maintain uncomfortable postures while performing repetitive, strenuous movements. 7 Prevalence measures the number of cases of a condition in a specified population at a specified time. 8 In 2018, the first major study investigating MSK symptoms in plastic surgeons reported that 78.3% have experienced a work-related injury. 9 However, no systematic review has been conducted that identifies the MSK disorders faced by each plastic surgery subspecialty (breast, hand, lower limb, craniofacial, pediatric, microsurgery, and aesthetic), revealing a gap in understanding variation in injury patterns across the field. 6
Given the breadth of plastic surgery subspecialties and the effects of poor ergonomics, defining subspecialty-specific challenges is imperative to develop informed preventative solutions. Thus, this systematic review aims (1) to define the prevalence and impact of work-related MSK disorders among plastic surgeons by subspecialty, (2) to identify injury risk factors, and (3) to propose ergonomic recommendations.
Materials and Methods
The requirement for institutional review board approval was waived as this work relied entirely on published primary research. The results will neither disseminate nor generate surgeon-identifiable information. This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 10 and the meta-analysis of observational studies in epidemiology guidelines. 11 This work abided by the tenets of the Declaration of Helsinki. The study was prospectively registered on PROSPERO (CRD420251026702).
Search and Study Selection
A systematic search was conducted on MEDLINE, Embase, CINAHL, Web of Science, and Scopus from inception until November 9, 2024, without language restrictions. Database search strategies were designed with input from an expert medical librarian (see Appendix, Supplemental Digital Content 1). Citations were reviewed to identify studies missed in the search.
Studies were included if they (1) reported primary ergonomic data on plastic surgeons; (2) were published in a peer-reviewed journal; (3) reported at least 1 prevalence estimate for a work-related MSK injury; (4) reported prevalence estimates for a common interval. Studies were excluded if they (1) were published as an abstract; (2) reported on non-MSK injuries; (3) reported on injuries in patients or nonplastic surgeons; (4) did not report injury/symptoms in plastic surgeons as a primary outcome.
Paired and independent reviewers (AM and BO) performed title and abstract screening, full-text screening, data extraction, and methodological quality assessment. Discrepancies were resolved via discussion.
Data Extraction and Methodological Quality Assessment
Data were extracted on study characteristics (location, design, sample size, and response rate), surgeon demographics (mean age, gender, training level, subspecialty, mean caseload, and mean years practicing), and injury-related characteristics (injury site, symptom, prevalence, days of work lost, necessary work adaptations, number of physicians requiring leave/early retirement, and risk factors). Methodological quality was assessed using the Joanna Briggs Institute (JBI) Checklist for Prevalence Studies. 12 Studies that satisfied <50%, 50% to 69%, and 70% or more of the JBI Checklist were considered to be low-, moderate-, and high-quality studies, respectively.13–17 Evidence certainty of study outcomes was evaluated using the GRADE tool. 18
The prevalence of work-related MSK disorders of the neck, lower back, upper back, shoulder, and forearm/wrist/hands was recorded. These sites were selected a priori because they are the most commonly investigated and affected areas across surgical subspecialties.19–22 When specifying the prevalence of forearm/wrist/hand symptoms, data that reported on injuries in broader locations such as “arms” were excluded because symptoms in this site could extend proximally beyond the forearm. If a study reported the prevalence of specific conditions, these estimates were extracted under their corresponding anatomic location. If a study explored multiple conditions affecting the same site, the highest prevalence among injuries affecting the same area was recorded.
Data Synthesis and Statistical Analysis
The primary measure was the overall literature-pooled prevalence (proportion; with a 95% confidence interval [95% CI]) of MSK injury among plastic surgeons, and additionally, the prevalence of MSK injury stratified by subspecialty.
The secondary measures were predictors for symptom development and impact on surgical performance. Female gender was hypothesized a priori to be a significant ergonomic risk factor due to smaller hand size, physiologic grip strength, and instrument designs more suited to male hands. 23 Therefore, gender was a candidate for meta-analysis. Similarly, injury impacts were hypothesized a priori to be significant, including worrying about future surgical ability, needing time off, and reducing case volume.
For continuous outcomes, we conducted a nonpairwise meta-analysis of prevalence proportions with 95% CI. The synthesis proceeded with a random effects meta-analysis utilizing a generalized linear mixed model, binomial distribution, pseudo-logit transformation for variance standardization, and maximum likelihood estimation. 24 For dichotomous outcomes, we conducted a pairwise meta-analysis to determine a literature-pooled odds ratio (OR) with 95% CI. A random effects meta-analysis of proportions was conducted using the Mantel–Haenszel method and maximum likelihood estimator to compare groups with versus without a given risk factor or impact.
Statistical heterogeneity was measured using the I2 value, which was interpreted according to Cochrane-endorsed thresholds: (i) might not be important (0%–40%); (ii) moderate (30%–60%); substantial (50%–90%); and considerable (75%–100%) heterogeneity. 25 Publication bias was evaluated qualitatively using funnel plots, and where applicable, quantitatively using Egger regression. Subgroup analysis omitted studies of low methodological quality. Analyses and figure syntheses were conducted in R (version 4.3.0; R Foundation for Statistical Computing, Vienna, Austria).
Results
The search yielded 270 unique studies (Figure 1). Citation screening identified 10 additional studies. Ultimately, 15 studies met the inclusion criteria. These studies were published between 2010 and 2024, and included microsurgery, craniofacial, aesthetic, hand, oculoplastic, and unspecified subspecialties (see Table, Supplemental Digital Content 2).
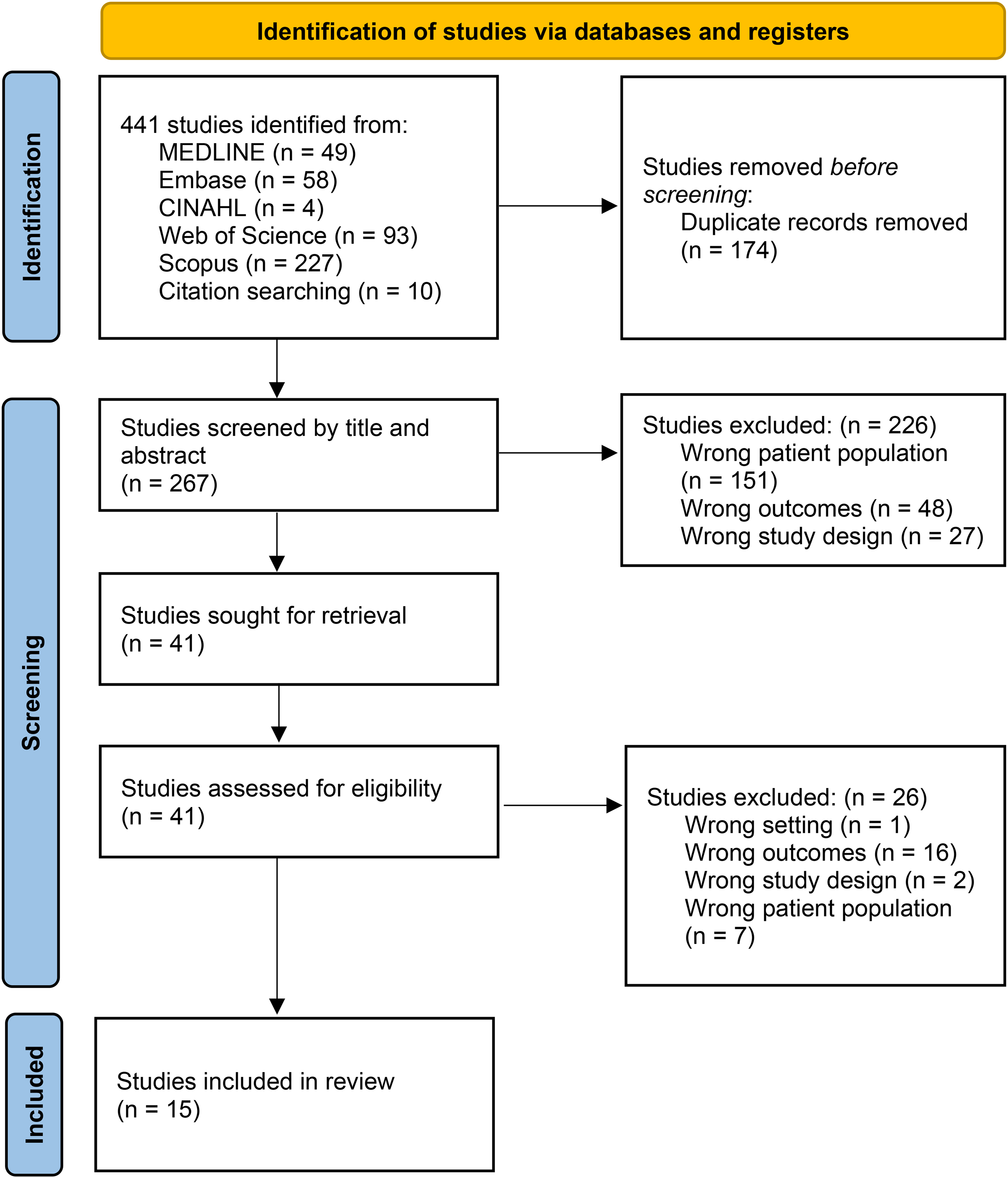
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram.
Methodological Quality
All included studies were observational in design with moderate methodological quality that predisposed them to very low GRADE certainty evidence (see Table, Supplemental Digital Content 3). Key factors reducing quality were low method validity (13 studies) and sample sizes (10 studies). Most data relied on self-reporting via surveys. Studies clearly described study subjects and settings (15 studies), selected appropriate sample frames (13 studies), and analyzed data with sufficient sample coverage (12 studies).
Meta-Analysis of MSK Injury Prevalence
Overall Injury Prevalence
Across 15 studies, there were 3313 surveyed surgeons, of whom 2274 reported MSK injury (1 affected per 1.5 surgeons). The pooled prevalence of MSK injury among plastic surgeons was 72.0% (95% CI [63.4, 79.3], I2 = 95%) (Figure 2). There was no significant heterogeneity between subgroups stratified by methodological quality, and statistical heterogeneity did not appreciably improve with subgroup analysis. There was no significant publication bias (p = 0.40) (Figure 3).
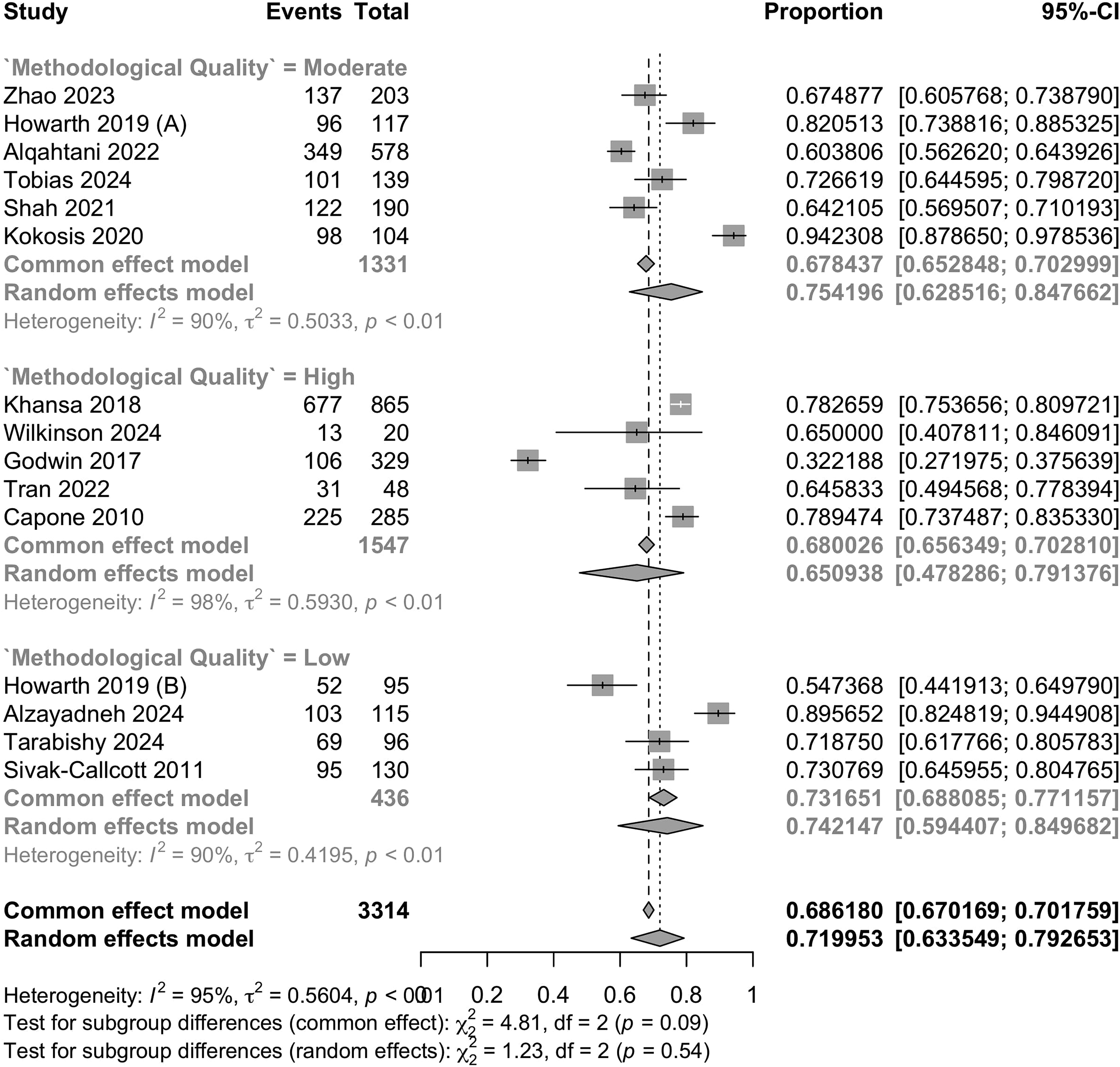
Forest plot for the synthesis of the prevalence of musculoskeletal injury among plastic surgeons.
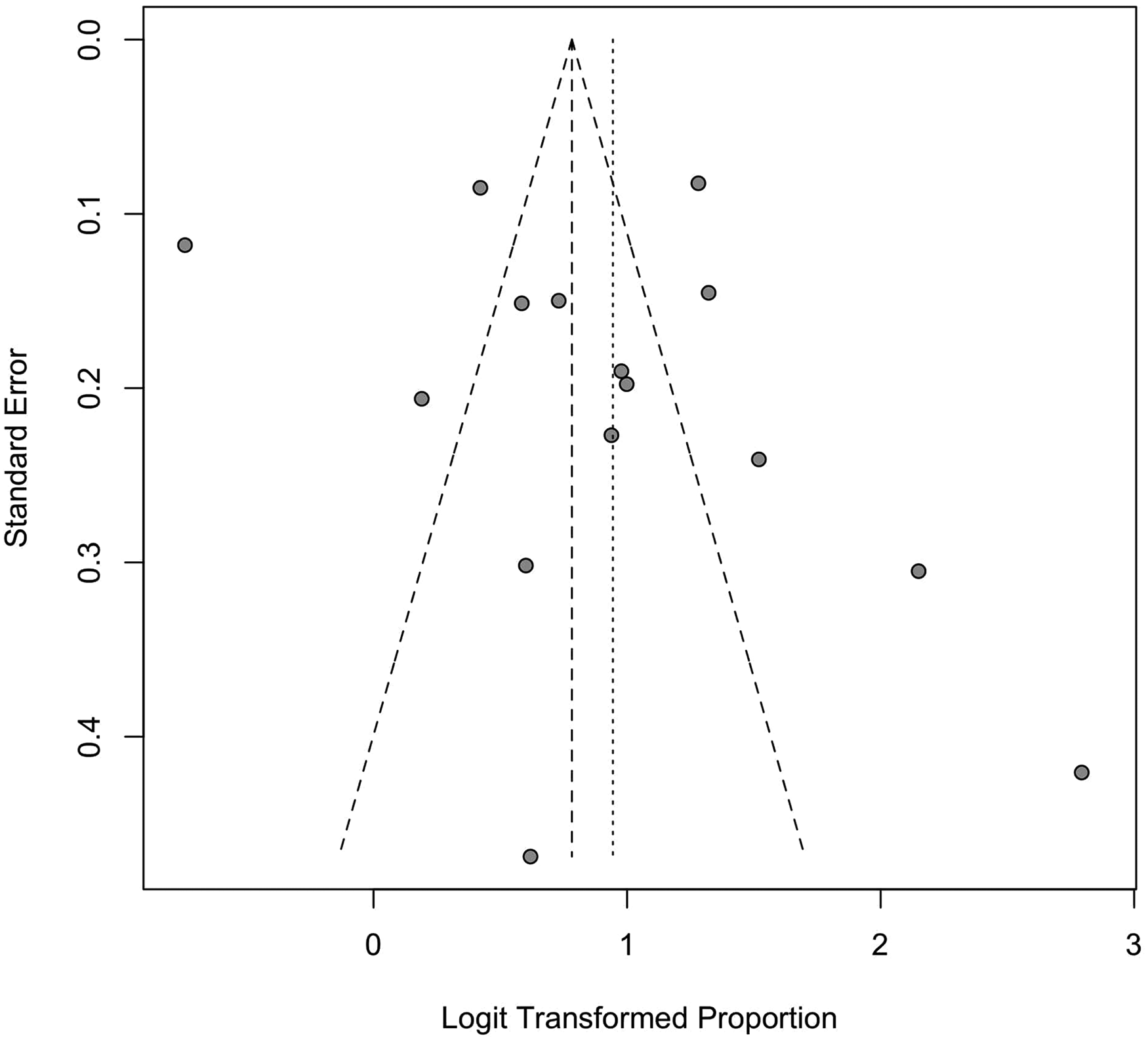
A funnel plot of overall injury prevalence.
Injury Prevalence by Plastic Surgery Subspecialty
Subspecialties reported by at least 2 studies (and therefore were eligible for meta-analysis) included microsurgery (n = 3 studies; 513 surgeons), craniofacial surgery (n = 3 studies; 408 surgeons), aesthetic surgery (n = 2 studies; 562 surgeons), and hand surgery (n = 5 studies; 965 surgeons) (Table 1). Injury prevalence was highest among aesthetic surgeons (84.3%; 95% CI [76.0, 90.1], I2 = 81) and lowest among craniofacial surgeons (69.4%; 95% CI [52.8, 82.1], I2 = 91%) (see Figure, Supplemental Digital Content 4). In the random effects analysis, subgroups with high methodological quality were significantly associated with higher prevalence estimates for craniofacial surgeons and lower prevalence estimates for aesthetic surgeons. For hand surgeons, moderate quality subgroups exhibited the lowest prevalence, whereas high quality subgroups depicted higher prevalence estimates. Subgroup analysis among high-quality studies resulted in reduced statistical heterogeneity. The smaller number of eligible studies precluded the statistical evaluation of publication bias for subspecialty- and impact-specific analyses (see Figure, Supplemental Digital Content 5).
A Table That Summarizes MSK Injury Prevalence by Subspecialty, Injury Site, and Impact on Function.
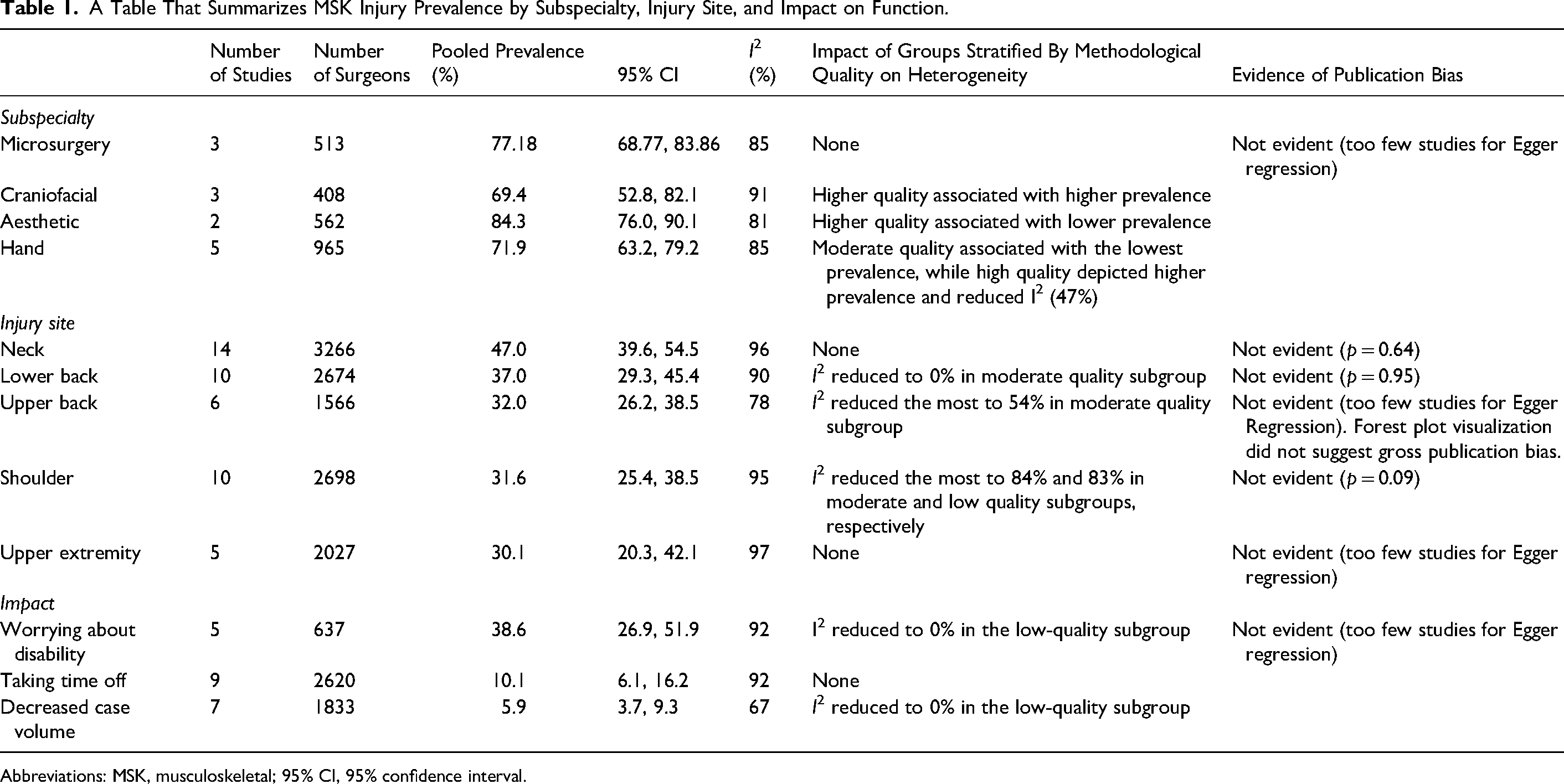
Abbreviations: MSK, musculoskeletal; 95% CI, 95% confidence interval.
Prevalence by MSK Injury Site
The neck was the most reported injury site with a pooled prevalence of 47.0% (95% CI [39.6, 54.5], I2 = 96%), followed by the lower back (37.0%; 95% CI [29.3, 45.4], I2 = 90%), upper back (32.0% (95% CI [26.2, 38.5], I2 = 78%), shoulder (31.6% (95% CI [25.4, 38.5], I2 = 95%) and forearm/wrist/hands (30.1%; 95% CI [20.3, 42.1], I2 = 97%) (see Figure, Supplemental Digital Content 6). The random effects analysis showed no significant heterogeneity between subgroups stratified by methodological quality. Heterogeneity was consistently high, although notably reduced in certain subgroups during quality-stratified analysis, including lower back and upper back injuries. Egger regression did not demonstrate publication bias for neck (p = 0.64), lower back (p = 0.95), or shoulder (p = 0.09) injuries (see Figure, Supplemental Digital Content 7). The smaller number of eligible studies precluded the statistical evaluation of publication bias for upper back and forearm/wrist/hand injuries.
Impact Prevalence
Worrying about future disability was the most reported injury impact with a pooled prevalence of 38.6% (95% CI [26.9, 51.9], I2 = 92%), followed by taking time off (10.1%; 95% CI [6.1, 16.2], I2 = 92%), and decreasing case volume (5.9%; 95% CI [3.7, 9.3], I2 = 67%) (see Figure, Supplemental Digital Content 8). The random effects analysis showed no significant heterogeneity between quality-stratified subgroups. Paradoxically, statistical heterogeneity decreased to 0% within the low-quality subgroup for worrying about future disability and decreasing case volume. Some degree of publication bias was suggested among most studies used to assess the impacts of worrying about future disability and taking time off (see Figure, Supplemental Digital Content 9).
Meta-Analysis of Gender as an Ergonomic Risk Factor
Five studies compared the gender-based injury distribution among plastic surgeons, encompassing 1474 males (1 affected per 1.5 surgeons) and 404 females (1 affected per 1.3 surgeons). The odds of injury did not significantly differ between females and males in the random effects analysis (OR: 1.3, 95% CI [0.9, 1.7], I2 = 33%). Yet, in the fixed effects model, females had significantly higher odds of injury (OR: 1.3, 95% CI [1.0, 1.7], I2 = 33%) (Figure 4). These findings may reflect the small sample size included in this analysis. There was no significant difference in effect size between quality-stratified subgroups. Paradoxically, statistical heterogeneity increased among high-quality studies. No significant publication bias was noted (p = 0.09) (Figure 5).
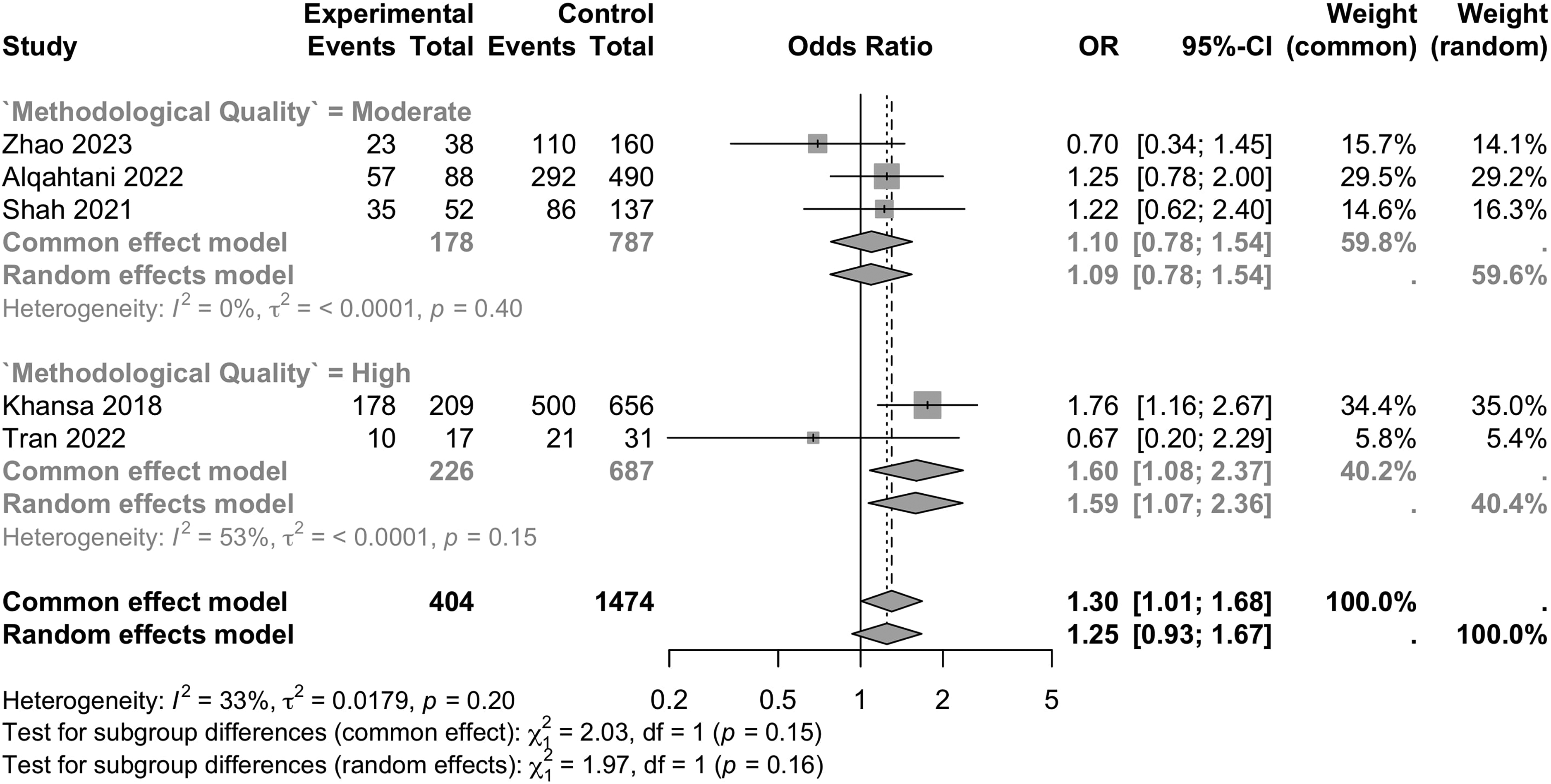
Forest plot on the association of surgeon gender with concomitant musculoskeletal injury among plastic surgeons.
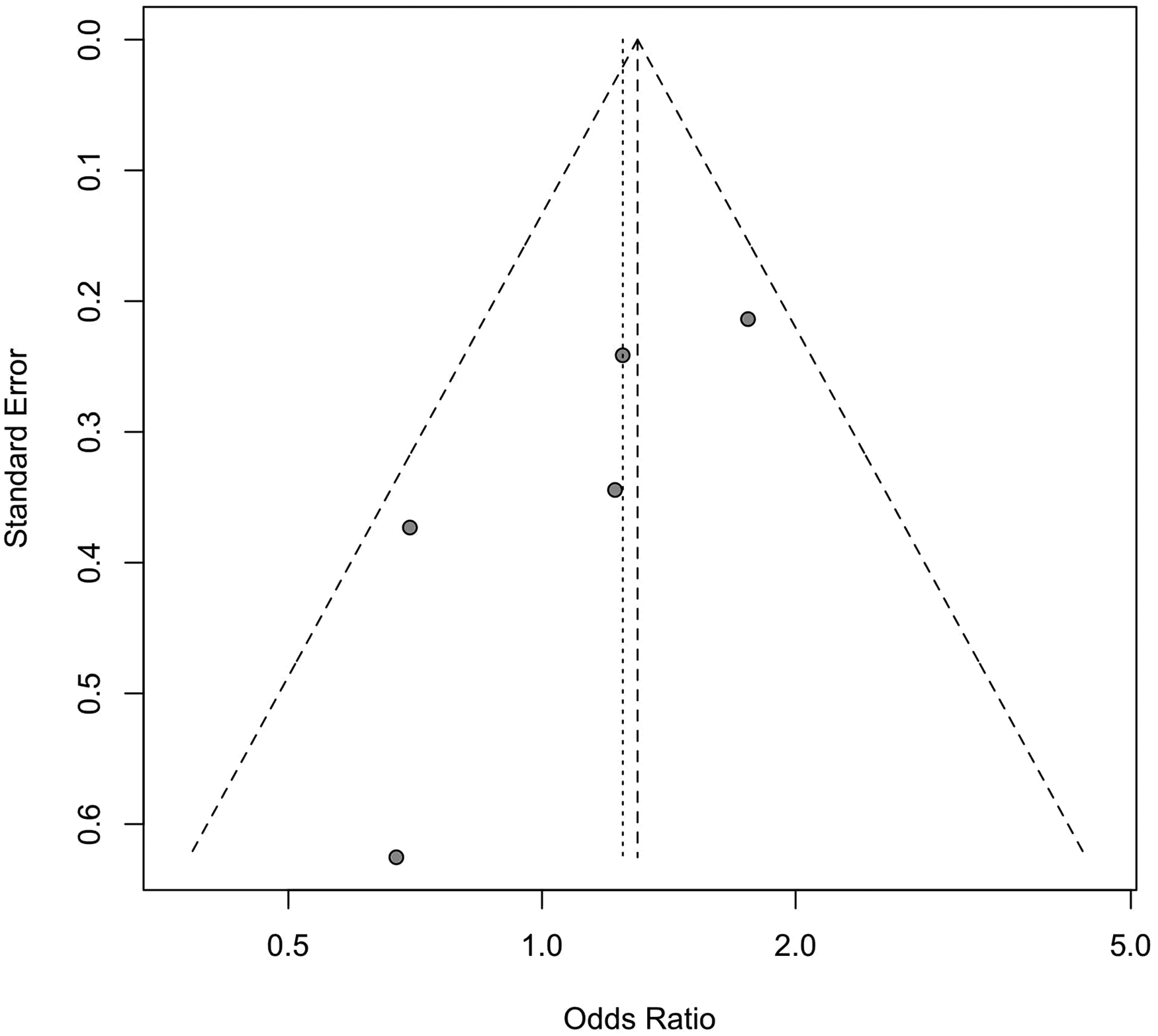
A funnel plot for musculoskeletal injury by surgeon gender.
Qualitative Analysis of Injuries
All included studies found that the most reported MSK symptom was pain/strain. Following pain/strain, stiffness and fatigue were common.9,26–28 Figure 6 displays injury prevalence by subspecialty and site.
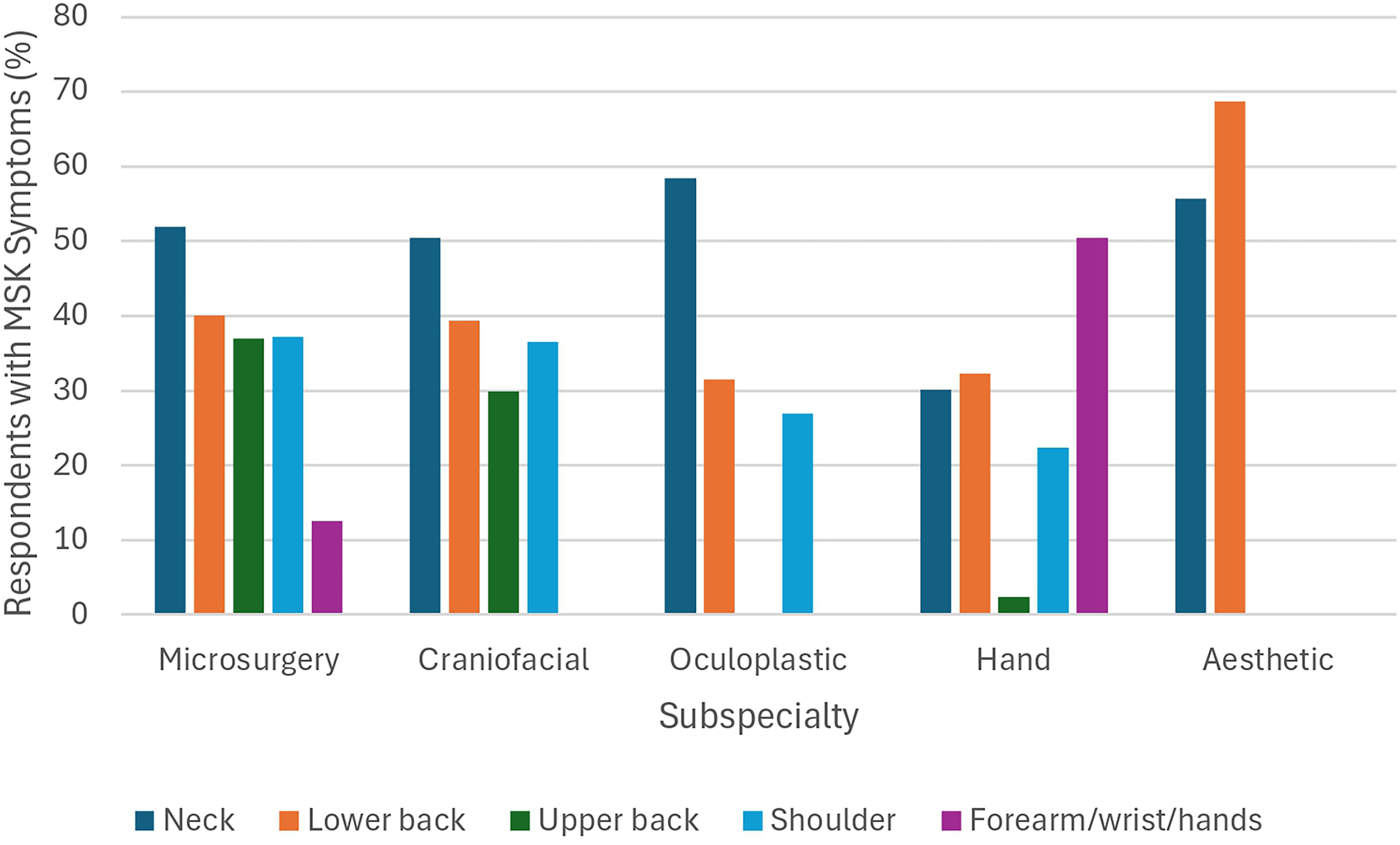
Bar chart of the prevalence of musculoskeletal (MSK) symptoms among body sites by subspecialty.
Qualitative Analysis of Ergonomic Risk Factors
The 3 most common significant ergonomic risk factors were years in practice (4 studies), caseload (4 studies), and age (3 studies). Alqahtani et al 29 reported that the number of work-related injuries in hand surgeons increased with years of practice. Craniofacial surgeons in practice for over 15 years had double the odds of having MSK symptoms. 28 Alzayadneh et al 30 noted a significant relationship between pain intensity and years of rhinoplasty practice. Plastic surgeons with over 20 years in practice had 3.39 times the odds of developing carpal tunnel syndrome. 31 Two studies found that years in practice were not a significant risk factor.
Regarding case volume, Alqahtani et al 29 reported a significant association between increased work-related injuries and higher caseload among hand surgeons. Weekly caseload was significantly associated with greater pain intensity and disability index in aesthetic surgeons. 30 Craniofacial surgeons who operated 3 or more days per week experienced significantly more lower back pain. 32 Interestingly, an annual caseload under 100 was a significant protective factor against MSK symptoms. 9 Two studies did not identify case volume as a significant risk factor.26,28
Concerning age, Khansa et al 9 found an increased MSK symptom prevalence in 45- to 54-year-old plastic surgeons. Older hand surgeons experienced significantly more work-related injuries. 29 Older plastic surgeons had a significantly higher incidence of cervical injuries. 33 Six studies did not report any significant injury differences by age.26,30,32–35
All investigated risk factors were summarized (see Table, Supplemental Digital Content 10).
Discussion
Our study found that (1) 72.0% of plastic surgeons have experienced a work-related MSK injury, with the highest prevalence in aesthetic surgeons, followed by microsurgeons, hand- and craniofacial surgeons; (2) the most common risk factors were years in practice, caseload, and age, while female gender was nonsignificant; and (3) the most reported impact was worrying about future disability.
These results illuminate how the effects of work-related injury extend beyond physical health to mental well-being and career longevity. Intense, repetitive physical demands predispose surgeons to injury and are reflected in this study, as 38.6% of plastic surgeons worried about future disability due to injury. Given the established impacts of MSK symptoms, it is unsurprising that surgeons have concerns regarding their future operative ability. Ruitenburg et al 36 found that 1 in 7 surgeons experienced challenges coping with physical operative demands due to reductions in their physical well-being. Scarcella et al 37 found that 53.7% of injured craniofacial surgeons experienced sleep difficulties due to symptoms. While Yakkanti et al 38 noted that 20 of 60 orthopedic surgeons required early retirement due to injury, our search only found 1 study reporting on early retirement, which occurred in 2% of plastic surgeons. 34 Future research is needed to fully characterize how injuries affect career longevity, given the paucity of literature on this topic.
Moreover, work-related MSK injuries can affect the volume and quality of patient care. Precisely, 10.1% and 5.9% of plastic surgeons reported taking time off and decreasing their caseload, respectively, due to injury. These findings are consistent with studies of other surgical specialties, where 0% of general, 39 8% of vascular, 40 and 12% of orthopedic surgeons 38 with work-related injuries took time off due to symptoms. Furthermore, MSK injuries likely impact the quality of care. Szeto et al 41 found that over 50% of injured general surgeons reported impaired operative performance. The working culture in surgical departments may pressure surgeons to sustain operative volume without taking time off for injury to avoid negative perception by colleagues. This perceptual fear has been reported as a significant ergonomic barrier. 42
Unsurprisingly, the most reported risk factors were years in practice, caseload, and age. With increasing years in practice and caseloads, surgeons are exposed to cumulative operative demands, increasing the likelihood of injury. Aging impacts surgeons’ endurance and ability to meet these physical demands. Resultantly, multi-faceted approaches are essential to reduce injuries, including optimizing caseload management and practicing core, neck, thoracic spine, and shoulder/internal rotation exercises.9,28,31,43,44 Nevertheless, these risk factors were not identified as significant in multiple studies, potentially due to studies that did not aim to identify risk factors, inconsistency in evidence, and variable study designs. Future research is needed to clarify the role of these factors in MSK injury development.
When analyzed by subspecialty, microsurgeons, craniofacial, and oculoplastic surgeons experienced injuries most often in the neck, followed by the lower back and shoulder (Figure 6). This finding is consistent with prevalent injury locations reported across surgical specialties. 45 Hand surgeons were mostly affected in their forearms/wrists/hands. Further investigation can identify subspecialty-specific causes of injury.
To address and prevent MSK issues, regular exercise and stretching were recommended for all subspecialties.9,26,28,30,31,44,46 Ergonomic education during surgical training was recommended for craniofacial 32 and hand surgeons.27,46 Awareness of ergonomic interventions is a key protective factor against injury.42,47–49 Thus, ergonomic education is a valuable tool to enhance knowledge and protect the health of plastic surgeons altogether. In total, 52% of plastic surgery residents developed MSK symptoms during the first 2 years of residency, and only 22% reported having ergonomics training. 50 Fanning et al 51 described how current resident well-being resources are insufficient to treat injuries, underscoring the need for resource development targeting resident physical health. Our findings can inform the development of tailored subspecialty-specific ergonomics training for residents.27,34 Novel technology development also presents an opportunity for ergonomic improvement. A study found that the use of a posture training device led to plastic surgeons spending a greater proportion of operating time in the neutral/upright posture. 52
Our systematic search did not identify studies representing all subspecialties; breast, pediatric, and burn surgeons may also encounter ergonomic barriers, injuries, and their sequelae. Studies have reported that nipple-sparing mastectomy is associated with increased physical demand and prolonged awkward positioning, promoting shoulder and trunk injuries.53,54 Future studies are needed to identify MSK injuries related to additional breast procedures and the breast subspecialty entirely. Furthermore, Gabrielson and Wei 55 found that pediatric otolaryngologists may be predisposed to higher pain rates compared to adult otolaryngologists due to smaller surgical fields and instruments. 55 This association would likely hold true in a study of pediatric versus adult plastic surgeons. No studies have investigated the ergonomics of burn surgeons. We hypothesize that the strength and endurance required for reconstructive burn procedures increase one's ergonomic risk. Further research can characterize the injury prevalence and risk factors among breast, pediatric, and burn surgeons to inform targeted ergonomic interventions.
Given the very low certainty evidence used in this review, we recommend that future research implement prospective and case-control designs to strengthen the evidence certainty. Randomized controlled trials would be ethically inappropriate given the injury risk inherent to this investigation. This study is subject to misclassification bias due to reliance on self-report surveys. Injury prevalence may be overestimated due to responder bias. 31 Selection bias is present due to convenience sampling. In-person surveys may have introduced social desirability bias. Injured physicians may have been unable to attend these events, potentially leading to an underestimation of the most impactful injuries. 31 High heterogeneity warrants caution in interpreting our subspecialty-specific findings. Participants may have had a baseline level of pain/strain that was not identified in our study; we cannot definitively attribute observed MSK symptoms solely to work-related causes. We included studies that investigated any pain/strain, rather than exclusively long-term pain symptoms leading to lifestyle limitations. Our search did not identify studies investigating injuries in breast, pediatric, and burn surgeons.
Conclusion
Overall, very low certainty evidence supports that 72% of plastic surgeons have experienced a work-related MSK injury, with aesthetic surgeons reporting the highest prevalence. The neck, lower back, and upper back were most often affected. Our findings underscore the necessity of tailored ergonomic solutions to improve the health and well-being of plastic surgeons while potentially preserving career longevity. Future research should focus on (1) identifying burn, pediatric, and breast-specific needs; and (2) developing subspecialty-specific intraoperative interventions and/or workload/physical conditioning solutions.
Supplemental Material
sj-docx-1-psg-10.1177_22925503251392594 - Supplemental material for Prevalence, Risk Factors, and Impacts of Musculoskeletal Injuries Among Plastic Surgeons: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-psg-10.1177_22925503251392594 for Prevalence, Risk Factors, and Impacts of Musculoskeletal Injuries Among Plastic Surgeons: A Systematic Review and Meta-Analysis by Alexis E. Mah, Beverley Osei, Brendan K. Tao, Brandon Chai, Katherine Zhu, Madeleine Wong, Orlin Chowdhury, Jeffrey Chen and Achilles Thoma in Plastic Surgery
Supplemental Material
sj-docx-2-psg-10.1177_22925503251392594 - Supplemental material for Prevalence, Risk Factors, and Impacts of Musculoskeletal Injuries Among Plastic Surgeons: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-psg-10.1177_22925503251392594 for Prevalence, Risk Factors, and Impacts of Musculoskeletal Injuries Among Plastic Surgeons: A Systematic Review and Meta-Analysis by Alexis E. Mah, Beverley Osei, Brendan K. Tao, Brandon Chai, Katherine Zhu, Madeleine Wong, Orlin Chowdhury, Jeffrey Chen and Achilles Thoma in Plastic Surgery
Supplemental Material
sj-docx-3-psg-10.1177_22925503251392594 - Supplemental material for Prevalence, Risk Factors, and Impacts of Musculoskeletal Injuries Among Plastic Surgeons: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-3-psg-10.1177_22925503251392594 for Prevalence, Risk Factors, and Impacts of Musculoskeletal Injuries Among Plastic Surgeons: A Systematic Review and Meta-Analysis by Alexis E. Mah, Beverley Osei, Brendan K. Tao, Brandon Chai, Katherine Zhu, Madeleine Wong, Orlin Chowdhury, Jeffrey Chen and Achilles Thoma in Plastic Surgery
Supplemental Material
sj-docx-4-psg-10.1177_22925503251392594 - Supplemental material for Prevalence, Risk Factors, and Impacts of Musculoskeletal Injuries Among Plastic Surgeons: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-4-psg-10.1177_22925503251392594 for Prevalence, Risk Factors, and Impacts of Musculoskeletal Injuries Among Plastic Surgeons: A Systematic Review and Meta-Analysis by Alexis E. Mah, Beverley Osei, Brendan K. Tao, Brandon Chai, Katherine Zhu, Madeleine Wong, Orlin Chowdhury, Jeffrey Chen and Achilles Thoma in Plastic Surgery
Supplemental Material
sj-docx-5-psg-10.1177_22925503251392594 - Supplemental material for Prevalence, Risk Factors, and Impacts of Musculoskeletal Injuries Among Plastic Surgeons: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-5-psg-10.1177_22925503251392594 for Prevalence, Risk Factors, and Impacts of Musculoskeletal Injuries Among Plastic Surgeons: A Systematic Review and Meta-Analysis by Alexis E. Mah, Beverley Osei, Brendan K. Tao, Brandon Chai, Katherine Zhu, Madeleine Wong, Orlin Chowdhury, Jeffrey Chen and Achilles Thoma in Plastic Surgery
Supplemental Material
Footnotes
Author Contributions
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability
Datasets generated and/or analyzed during this review are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The requirement for institutional review board approval was waived as this work relied entirely on published primary research. The results will neither disseminate nor generate surgeon-identifiable information. This article does not contain any studies with human or animal subjects.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.