
Abstract
Introduction
Musculoskeletal (MSK) pain and injuries are preventable health risks that endanger the well-being of all working Canadians, with surgeons being no exception. Despite the innovation and progress seen in modern ergonomics, the operating room has been minimally adjusted to protect surgeons. In fact, surgeons often experience work environments that rival those of industrial workers with regard to the risk of MSK injuries or disorders. The impact of these working conditions on surgeon health has been well-documented in the literature.1,3 A recent systematic review and meta-analysis identified MSK symptoms and disorders as being a possible contributor to future workforce shortage within the community of surgeons and interventionalists. 4 Increased surgical duration, awkward positions, and minimally invasive surgery have all led to an impending epidemic of surgeon disability. 5 Although the impact of MSK symptoms has been documented in Vascular Surgery, 1 Ophthalmology, 2 and Otorhinolaryngology, 3 their impact in the Plastic and Reconstructive Surgery realm has yet to be explored. As such, this survey of Canadian Plastic Surgeons and trainees sought to identify if MSK symptoms could manifest as time lost at work, disability, and even eventual early retirement due to these symptoms.
Methods
Online Survey
Using the online portal Alchemer LLC: Online Survey Software and Tools (www.alchemer.com), an online survey was used to evaluate the MSK symptoms experienced by Canadian plastic surgeons and trainees in 2021. The survey was comprised of fixed-choice response options and included 4 sections: (1) Operative experience, (2) Exercise frequency, (3) Work-related MSK symptoms, and (4) Demographics. Questions were developed by the research team and informed by a review of the literature. Responses were collected anonymously. Based on Alchemer's proprietary algorithm, the survey had an estimated completion time of 8 min with a low risk of user fatigue. To support the user experience, the survey was written at a high-school level of reading comprehension, contained a progress bar, and had the ability to save answers for future completion. The final version of the questionnaire and all associated forms were approved by the institution's research ethics board (ARISE Study ID: Pro00100307).
Study Sample
As this study aimed to perform a cross-sectional analysis of MSK symptoms among Canadian plastic surgeons and trainees, a recruitment email was disseminated to all active members of the Canadian Society of Plastic Surgeons (CSPS). To be an active member of CSPS, you must be practicing plastic surgery in Canada and certified by: (1) the Royal College of Physicians and Surgeons of Canada, (2) the American Board of Plastic Surgery, and/or (3) the Collège des médecins du Québec. Additionally, to ensure the inclusion of trainees, the recruitment email was also sent to all residents enrolled in a plastic and reconstructive surgery residency program in Canada.
The initial recruitment email was first sent out in September 2021 with a reminder email being disseminated in November 2021. The survey remained open until January 1, 2022.
Data Analysis
The data were summarized using frequency distributions. Missing responses varied by question. Reported percentages are item-specific (denominator varies). Chi-square and Fisher exact tests were used to test for associations. STATA for Mac version 14.1 was used and a significance level of P < .05 was set.
Results
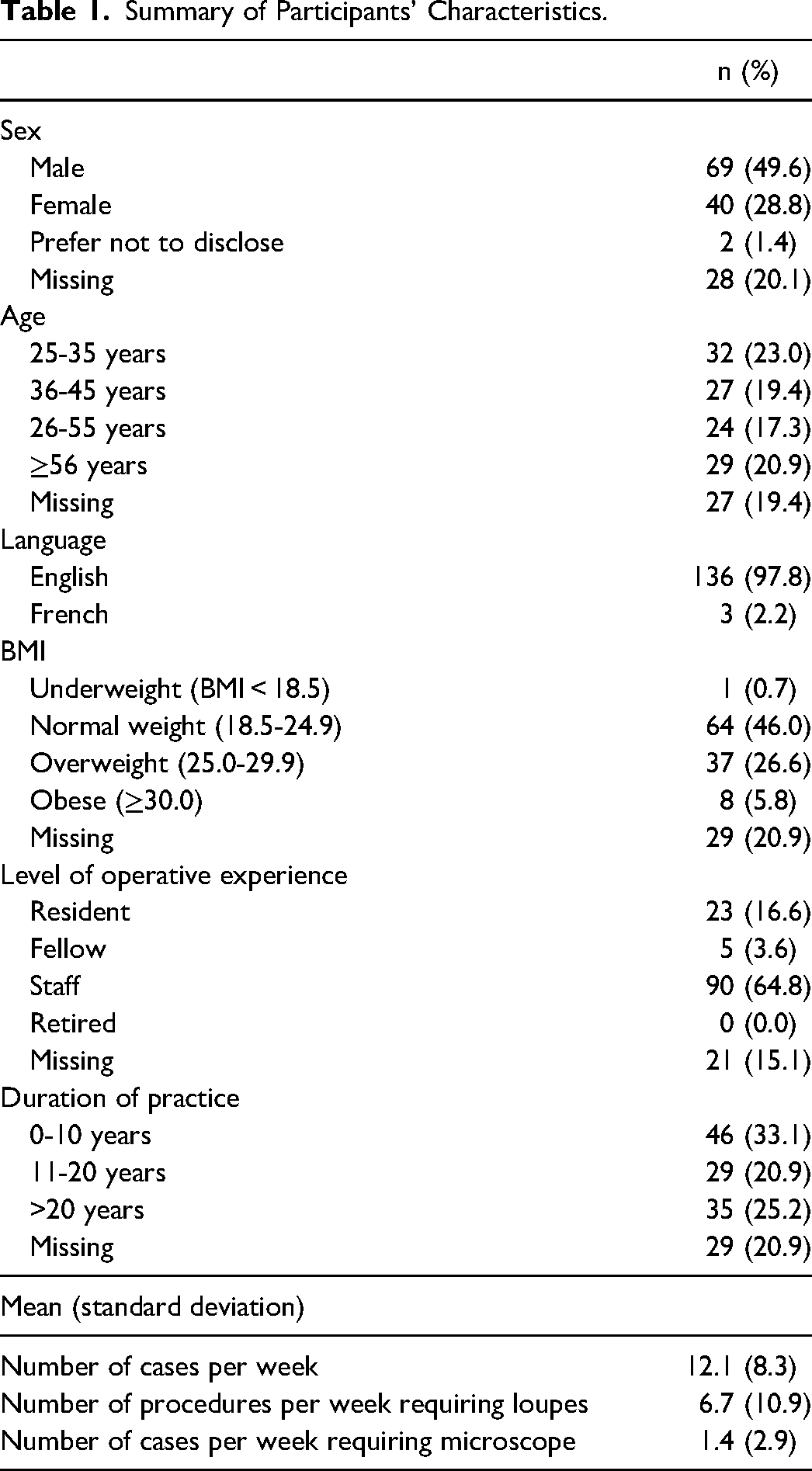
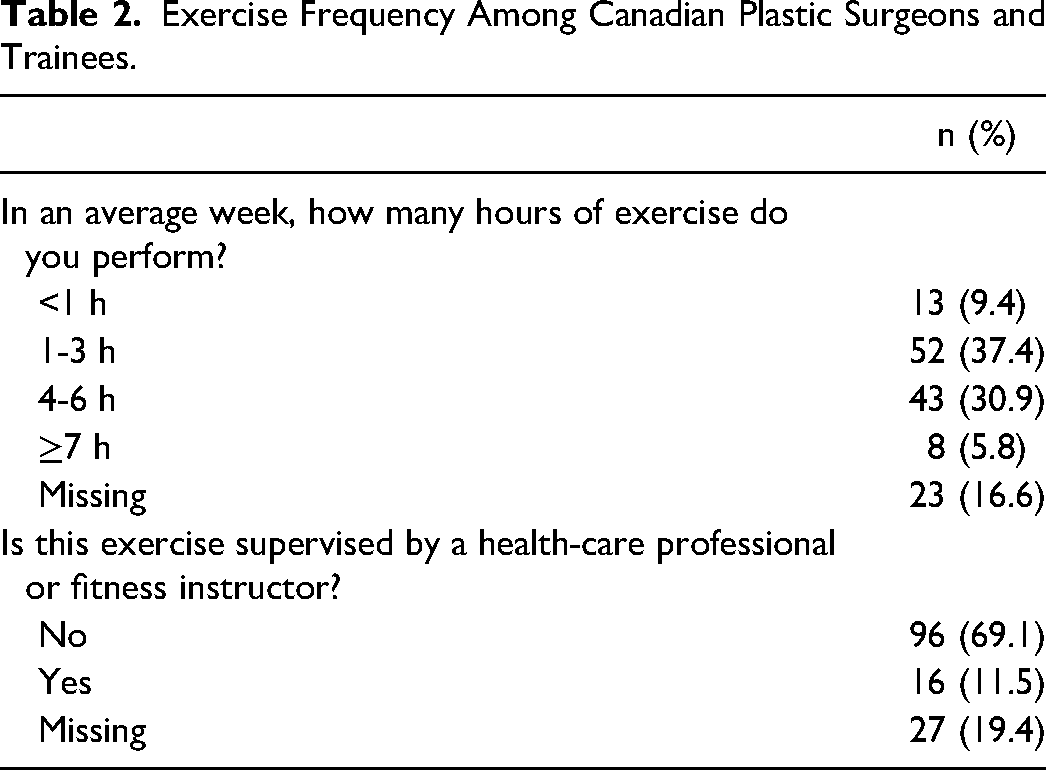
Of the 604 invitation emails distributed, a total of 139 surveys were completed (response rate = 23.0%). Among respondents, 49.6% were male, 97.8% identified English as their primary language, and 64.8% were staff physicians (Table 1). When asked about their exercise frequency, 74.1% of participants reported exercising at least 1 h per week and 30.9% were exercising 4 to 6 h per week (Table 2).
Summary of Participants’ Characteristics.
Exercise Frequency Among Canadian Plastic Surgeons and Trainees.
Musculoskeletal Symptoms Among Canadian Plastic Surgeons and Trainees
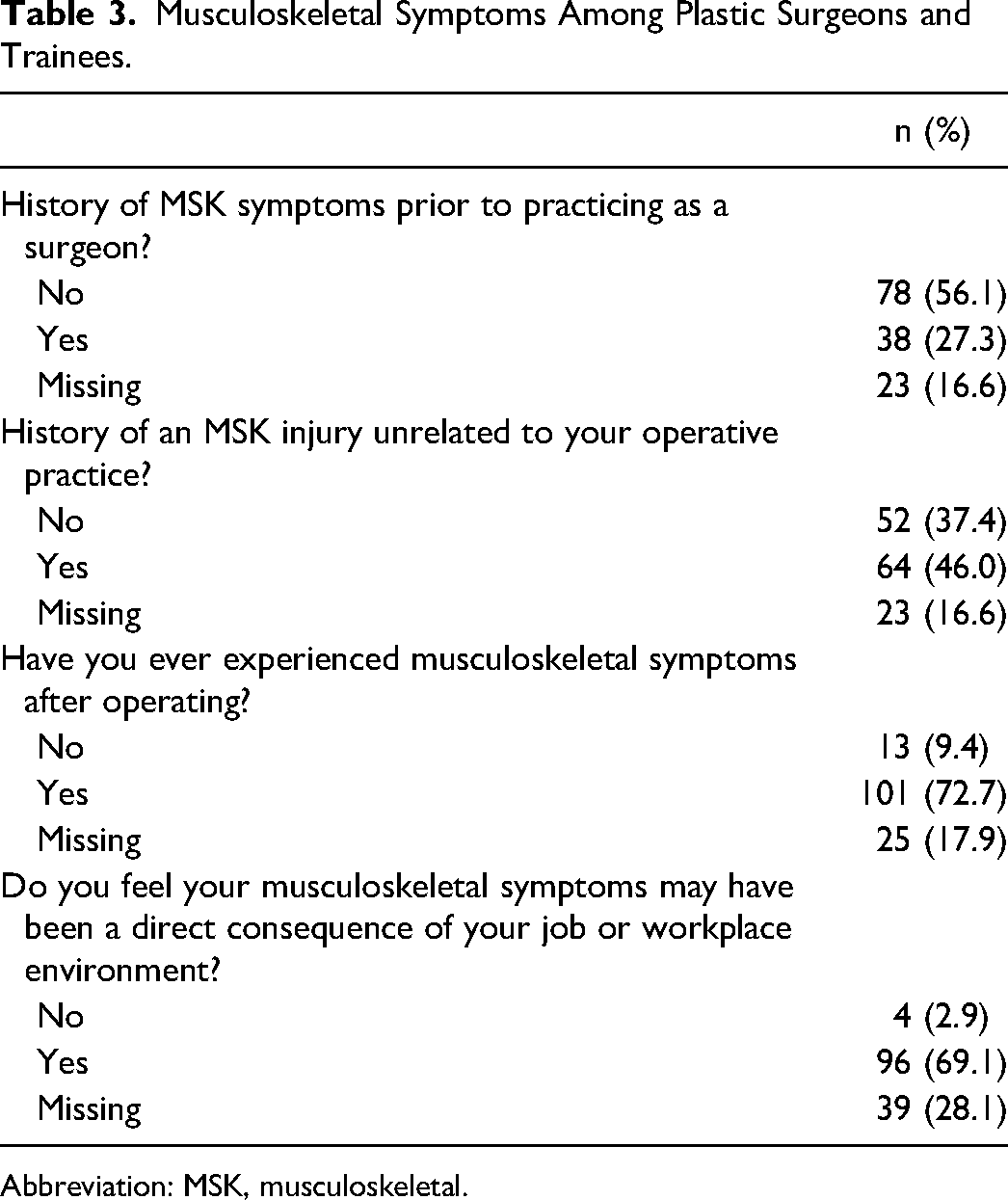
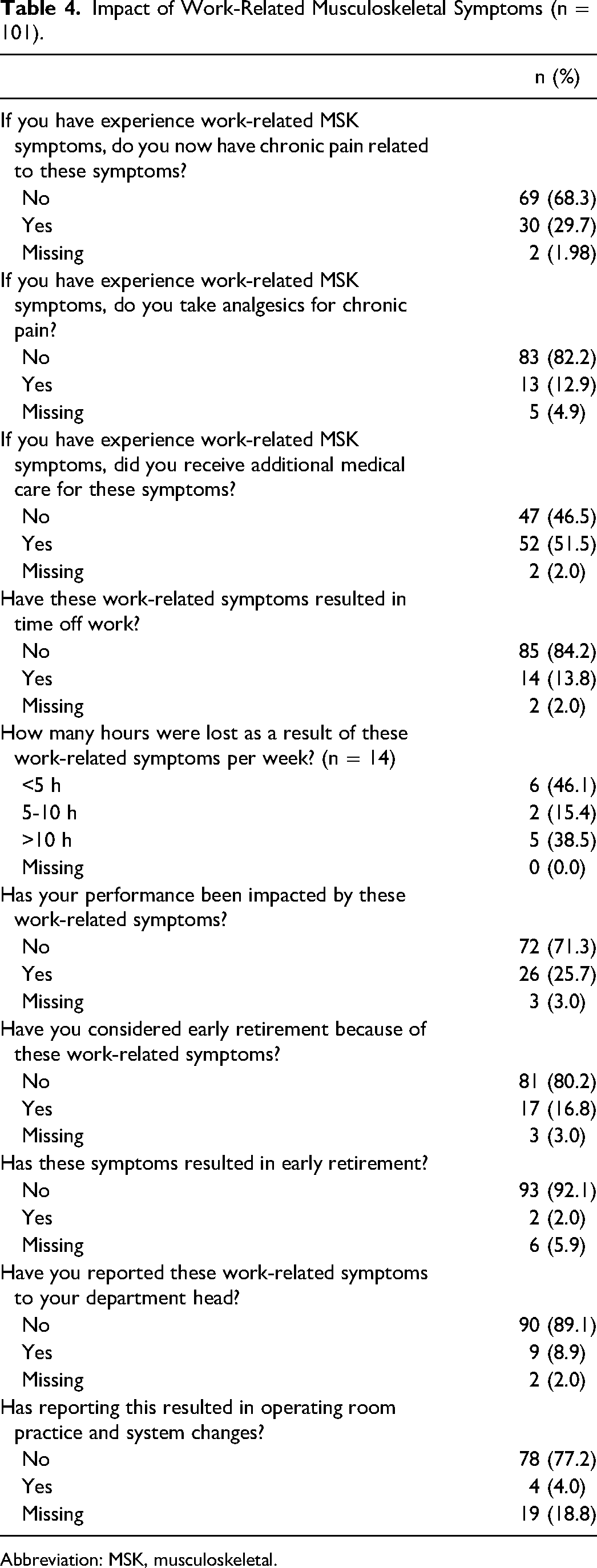
Musculoskeletal symptoms were common among Canadian plastic surgeons and trainees with 72.7% of respondents reporting having experienced MKS symptoms after operating (Table 3). Among those with work-related MSK symptoms, 29.7% reported that they have developed chronic pain and 13.8% of respondents reported having to take time off work secondary to their symptoms (Table 4). Furthermore, 25.7% of respondents endorsed that their MSK symptoms had a direct consequential impact on their surgical performance. In fact, 16.8% of respondents indicated that they have considered early retirement and 2.0% of respondents had to take early retirement because of these symptoms. When asked about which body parts respondents experienced their work-related MSK symptoms, the neck (76.2%) and back (72.2%) were most frequently affected (Table 5). There was no significant difference in work-related MSK symptoms with regard to age (P = .09), sex (P = .5), BMI (P = .8), exercise frequency (P = .06), or loupe declination (P = .4).
Musculoskeletal Symptoms Among Plastic Surgeons and Trainees.
Abbreviation: MSK, musculoskeletal.
Impact of Work-Related Musculoskeletal Symptoms (n = 101).
Abbreviation: MSK, musculoskeletal.
Body Parts Most Affecting by MSK Symptoms After Operating.
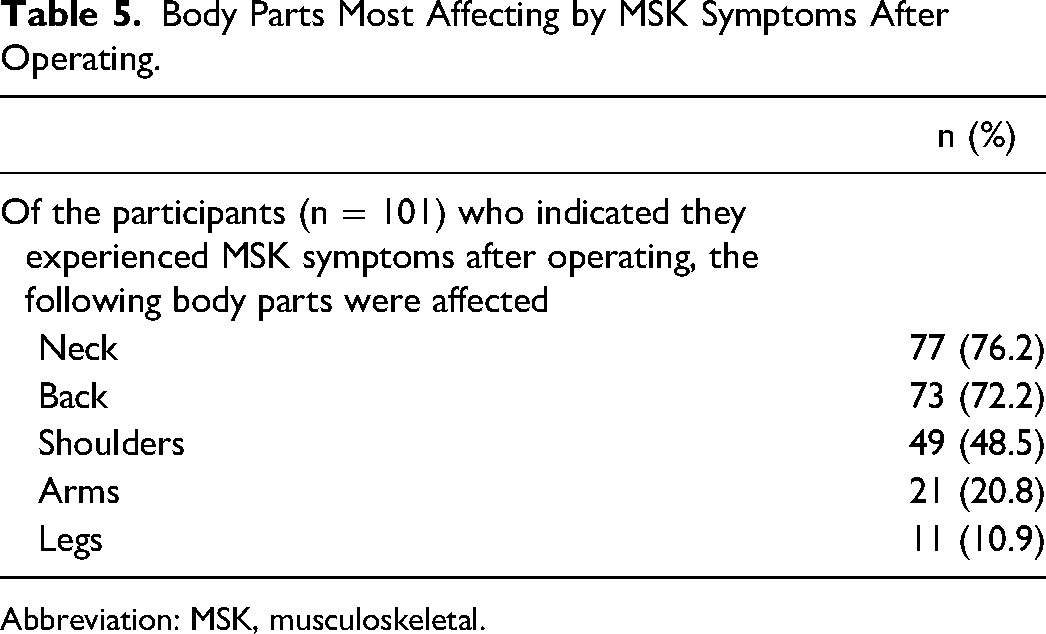
Abbreviation: MSK, musculoskeletal.
Although MSK symptoms were common among Canadian plastic surgeons and trainees, they remain largely unreported. When asked if respondents had reported their work-related MSK symptoms to their department head, only 8.9% stated they had (Table 4). Moreover, only 4.0% of respondents noted that reporting symptoms actually resulted in either change in the operating room or systematic changes.
Discussion
Regardless of their role as attending or resident physicians, Canadian plastic surgeons are at risk of MSK pain and injuries as a result of their work environment. These MSK symptoms are in part preventable and share a common etiology. The procedural work involved in plastic surgery requires many hours of standing, often without breaks or antifatigue mats, awkward positioning, and the use of nonergonomically designed tools and instruments.6,7 Moreover, as efforts are made to increase the number of procedures performed under local or regional anesthetic, plastic surgeons are increasingly working outside of the operating room. This may exponentiate the amount of time surgeons are subject to awkward posturing as they fight to operate in small, poorly lit clinic rooms that were never designed for this type of practice.
Our results suggest that MSK symptoms are far from uncommon among Canadian plastic surgeons. Moreover, these MSK symptoms are rarely reported and despite overwhelming support for improved ergonomics, few efforts have been made to apply them in the operating room.6,7 It is well reported in the literature that there is an inherent culture among physicians of underreporting pain or injuries sustained while at work, despite the physical toll being similar to coal miners, manufacturing laborers, and physical therapists. 4 This is driven by the acceptance of the current surgical culture that prioritizes patient-first care in exchange for the physical demand and pain associated with their occupation. 7
As such, there is a need for a culture of acceptance towards adopting improved ergonomics within the operating room, and new attitudes about pain and disability as the result of time spent operating. Decreasing MSK symptoms is contingent on change to current practice for those already living with symptoms, alongside the introduction of preventative strategies. For example, a study investigating cervical spine morbidity in United Kingdom consultant plastic surgeons found that static postures, namely head-forward posture, made worse by operating with loupe magnification, were more likely to experience cervical morbidity. 8 Interestingly, this study identified MSK symptoms in the form of cervical morbidity to be most highly impacted by time spent operating using loupes, especially for older respondents. 7 Motion capture imaging in this study also demonstrated that operating with loupe magnification causes anterior flexion of the neck, resulting in a protracted position anterior to that of neutral posture. Given our understanding that nonanatomic positioning for prolonged periods contributes to cervical morbidity, it is not surprising that our study found that neck pain was the most commonly reported MSK symptom among our respondents.5,7,9
Without major institutional change, many of the day-to-day exposure risks for MSK symptoms may be unavoidable, especially as a trainee. Most job postings in Canada offer 1 to 2 operative days a week in addition to procedural clinic time. 8 Anecdotally, most residents spend more time in the operating room as well as the emergency department late at night doing bedside procedures. This would imply that residents may be most vulnerable to develop MSK symptoms during their training period. Prolonged work hours, overtime shifts, and limited breaks are risk factors described by the Center for Disease Control and Prevention for the development of MSK symptoms. 10 These are inevitable risk factors for surgical trainees, and the compound effect of these risk factors as an attending appears to lead to long-term morbidity.7,9
Without the implementation of large-scale changes, these work conditions are unlikely to change. In 2017, Hallbeck et al introduced microbreaks as a way to mitigate MSK symptoms in their operating rooms. 9 Adapted from nonsurgical fields, microbreaks are short breaks, lasting approximately 1 to 2 min, typically taken every 20 to 30 min that have been shown to reduce fatigue. 9 These microbreaks are not the same as repositioning or changing positions, rather these microbreaks involved a structured set of brief exercises and stretching.9,11 The adoption of these microbreaks was shown to decrease error9,12 and reduce MSK symptoms, both subjectively and objectively, 12 without increasing the duration of surgery. 9 In combination with optimal table height, proper positioning of the patient, and ergonomic equipment including antifatigue mats and loupes with a proper declination angle, microbreaks could be incorporated to optimize the surgical experience.9,13
Although reactionary measures to address risk factors for MSK symptom is essential, it is also vital to consider preventative measures. In 2017, the Duke University School of Medicine introduced a new ergonomic program to improve surgeon and trainee health. 13 In collaboration with their Ergonomics Division, the School of Medicine led a program to teach learners about appropriate positioning and ergonomics in the OR. Aside from the abovementioned strategies to decrease surgeon morbidity, they assigned “coaches” to train junior residents, in an effort for this knowledge and expertise to be passed down year-to-year. 13 A small group of students took part in an innovative workshop where they were fitted with a device that vibrated when they slouched. 13 This in turn lead to 76% of students correcting their posture, in comparison to the group who were told their posture was being evaluated by the device but received no vibration feedback. Given these results, residency programs across Canada should recognize the importance of ergonomics and urge staff physicians to critically appraise and correct the operative posture of residence and continue to advocate for their well-being.
As our data were collected via a survey, it is subject to a number of limitations and potential biases. Given the impact of MSK symptoms, our survey is at risk of response bias where those that are impacted by these symptoms may be more likely to respond. The percentage of MSK symptoms within our sample, however, was similar to prior data published in the literature. It should also be noted that our response rate of 23% is less than the ∼30% response rates typically reported among Canadian surgeons.14,16 Although efforts were made to optimize our survey, web-based surveys have been traditionally shown to be associated with lower response rates. 14
With respect to MSK symptoms reported in our survey, we depend on the subjective experience of the respondent and did not require any formal diagnoses. Although we felt the subjective experience of the surgeon was most important for this study, the risk of both under- and overreporting of symptoms is possible. One particular concern for this study was the risk of underreporting the true percentage of MSK symptoms. The literature highlights the culture of underreporting MSK symptoms among surgeons and as such, there exists the potential for a social desirability bias in these data, where MSK symptoms are seen as either a poor reflection of surgical technique or the lack of fortitude to excel in the field of plastic surgery.
Another limitation is that the data in this study focused on Canadian plastic surgeons and may not be generalizable to other specialties or even other countries. Although long procedures and awkward positioning are not specific to plastic surgery, there is a high number of procedures performed outside of the operating room with or without loupes in unfavorable conditions (eg, clinic or the emergency department). Moreover, as plastic surgeons in Canada operate under a publicly funded system, institutional investment into ergonomic improvement may vary when compared to other countries.
Finally, this study's exploration of the association between exercise and MSK symptoms was rudimentary. As a novel topic, this study provides insights into the rates of exercise among Canadian plastic surgeons; however, further exploration into the impact of various types of exercise such as yoga, weightlifting, or running on MSK symptoms related to a career in plastic surgery is warranted. In fact, based on the frequency of MSK symptoms among Canadian plastic surgeons and trainees, we believe future research should focus on developing formal interventions or protocols to optimize surgeon ergonomics and MSK health. As most Canadian residency programs are now structured according to the Competence by Design framework, formalized assessment of posture and ergonomics may be beneficial.
Conclusion
Musculoskeletal pain and injuries are a common, yet underreported outcome of performing plastic surgery as a trainee or attending surgeon in Canada. It is often the result of awkward positioning, lengthy operations, and a culture of working through the pain. Given the ubiquity of symptoms experienced by surgeons and the resulting time off work and early retirement, a culture shift towards the prioritization of ergonomics in the operating room and clinic is imperative. In doing so, the risk of MSK injuries assumed by Canadian plastic surgeons can be mitigated, thus prolonging surgeon health and practice.
Footnotes
Authors’ Note
This work was presented at the 2022 Annual Meeting of the CSPS in Québec City, Québec. Subsequently, this was presented at the American Society of Plastic Surgeons’ Annual Meeting in Boston. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study. Ethics approval was obtained by the University of Alberta Research Ethics Board (ARISE Pro00100307).
Author Contributions
GT was the lead author for this project and responsible for project conception and proposal development. GT was also involved in all remaining aspects of this project including survey development, data collection, analysis, and results dissemination. SXD was involved in survey development, data collection, data analysis, and results dissemination. JNW was the principal investigator for this project and was involved in proposal development, survey development, data analysis, and results dissemination. All authors wrote, read, revised, and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.