
Abstract
Introduction
Female-to-male gender-affirming mastectomy, involving breast tissue removal to create a more masculine chest appearance, has been associated with improved body image, gender congruence, and reduced gender dysphoria. 1 This surgery often includes the use of surgical drains, which are designed to remove excess fluid from the surgical site with the goal of reducing postoperative seroma formation. This may reduce the need for subsequent procedures and improve patient satisfaction. 2 Despite these advantages, drains may be associated with discomfort, limited mobility, and scarring, prompting some surgeons to consider drainless surgical techniques.3,4
The role of patient preferences in surgical decision-making is a key component of patient-centered care. In the context of gender-affirming mastectomy, there is limited evidence on how patients weigh the risks and benefits of drains versus drainless procedures. Understanding these preferences is essential for optimizing surgical planning and aligning postoperative expectations with patient values, while also focusing on personal aspects of identity and self-expression. 5
The standard gamble technique is a well-established method in healthcare for quantifying patient preferences associated with different treatments and health outcomes. 6 Traditionally, the standard gamble method involves presenting patients with a choice between a certain health state and a hypothetical gamble that includes 2 possible outcomes: perfect health or death. This approach provides a strong framework for understanding tradeoffs that patients are willing to make when faced with uncertain outcomes. Previously, modified versions of the standard gamble have been applied to specific clinical scenarios, including managing ureteral stones with surgical and nonsurgical treatment 7 and assessing patient preferences regarding cervical cancer treatment side effects. 8 These adjustments tailor the method to emphasize practical tradeoffs instead of theoretical extremes, enhancing its relevance for clinical applications.
In this study, a modified standard gamble approach was used to assess how patients weigh the risks associated with avoiding drains. A key concept in this study is risk tolerance, defined as the maximum level of risk an individual is willing to accept before opting for the use of drains.
By quantifying risk tolerance and exploring subjective concerns related to drain use, this study aims to
Provide insights into the preferences of transgender and gender-diverse individuals regarding their acceptance of different complication risks in surgical decision-making. Highlight the factors that influence decision-making, including prior surgical experience, age, and personal exposure to drains or seromas. Bridge the gap in existing research by incorporating patient-centered perspectives into surgical planning.
We hypothesized that patients would demonstrate a defined risk tolerance—accepting a measurable risk of seroma formation and the need for secondary procedures before preferring to have drains placed.
Methods
Study Design
This study employed a modified standard gamble approach to evaluate patient preferences for the use of postoperative drains versus drainless procedures during gender-affirming mastectomy. Participants completed a survey comprising 2 scenarios and a supplemental questionnaire assessing subjective concerns regarding the procedures.
Study Population
A 1 time survey was conducted of patients seen in the pediatric plastic surgery clinic. Transgender youth were invited to participate if they were referred for or had undergone a gender-affirming mastectomy. All youth referred for consideration of gender-affirming mastectomy were assessed by a multidisciplinary team at multiple time points to assess readiness for surgery. Demographic data, including age, gender identity, assigned sex at birth, prior surgical history, and experience with drains or seromas, were collected. A sample size of 30 was selected based on the intensive nature of the modified standard gamble process and in alignment with similar studies involving standard gamble methodology 9 and surveys within transgender populations.10,11
Modified Standard Gamble Approach
The standard gamble method quantified participants’ willingness to accept specified risks to avoid the use of drains. Two scenarios were presented:
Participants were asked to choose between accepting the risk, remaining indifferent, or preferring drains outright (placed at the time of surgery). The starting risk was 50%, adjusted iteratively by increments of 10% (increased if the risk was accepted, decreased if rejected) until the indifference point was identified. For cases where the indifference point fell between 2 tested probabilities, the midpoint was recorded.
Supplemental Questionnaire
Participants also completed a survey assessing their perceptions of surgical drain placement and omission using a 7-point Likert scale (1 = strongly disagree, 7 = strongly agree). The survey included statements evaluating concerns related to the presence of drains, such as difficulty managing, discomfort, concealability, aesthetic concerns, pain, difficulty with removal, emotional distress, perceived necessity, risk of additional complications, and scarring. Additional statements assessed concerns related to the absence of drains, including the risk of postoperative complications, impact on final surgical outcomes, and the potential need for additional procedures. Mean Likert scale scores were calculated for each statement, with higher scores indicating greater agreement with the concern.
Statistical Analysis
Descriptive statistics, including the mean, median, standard deviation (SD), and interquartile range (IQR), were computed. For the subgroup analysis, both means and medians were calculated, and statistical tests were conducted to assess differences between groups. Given the nonnormal distribution of the data, as indicated by visual inspection and skewness, nonparametric tests were employed. The Mann–Whitney U test was used for comparisons between 2 independent groups (eg, prior surgery vs no prior surgery), while the Kruskal–Wallis test was applied for comparisons across multiple age groups. These tests were selected for their suitability in analyzing small sample sizes and ordinal data distributions. For the supplementary survey, mean values were computed for each concern rating to summarize patient perceptions regarding drains versus drainless procedures, and 95% confidence intervals (95% CI) were calculated. All statistical analyses were performed using Python.
Results
Participants had a mean age of 17.6 years (SD = 1.3) and identified as 80% trans male, 17% nonbinary, and 3% gender nonconforming. Forty-seven percent of participants had previously undergone gender-affirming mastectomy (with drains). Two patients had a seroma requiring needle aspiration in clinic (Table 1).
Demographic and Clinical Characteristics of the Study Participants.
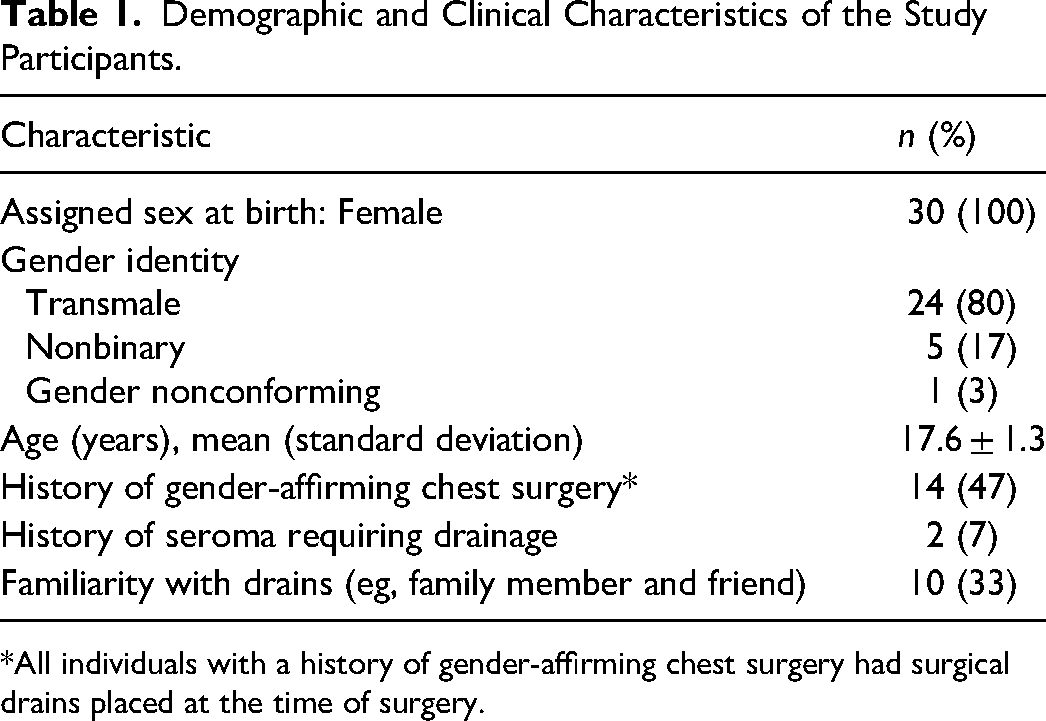
*All individuals with a history of gender-affirming chest surgery had surgical drains placed at the time of surgery.
The median risk tolerance for seroma formation was 15% (IQR: 5.5%–25%), and the median risk tolerance for requiring a secondary procedure due to complications was 10% (IQR: 1%–15%) (Figure 1).
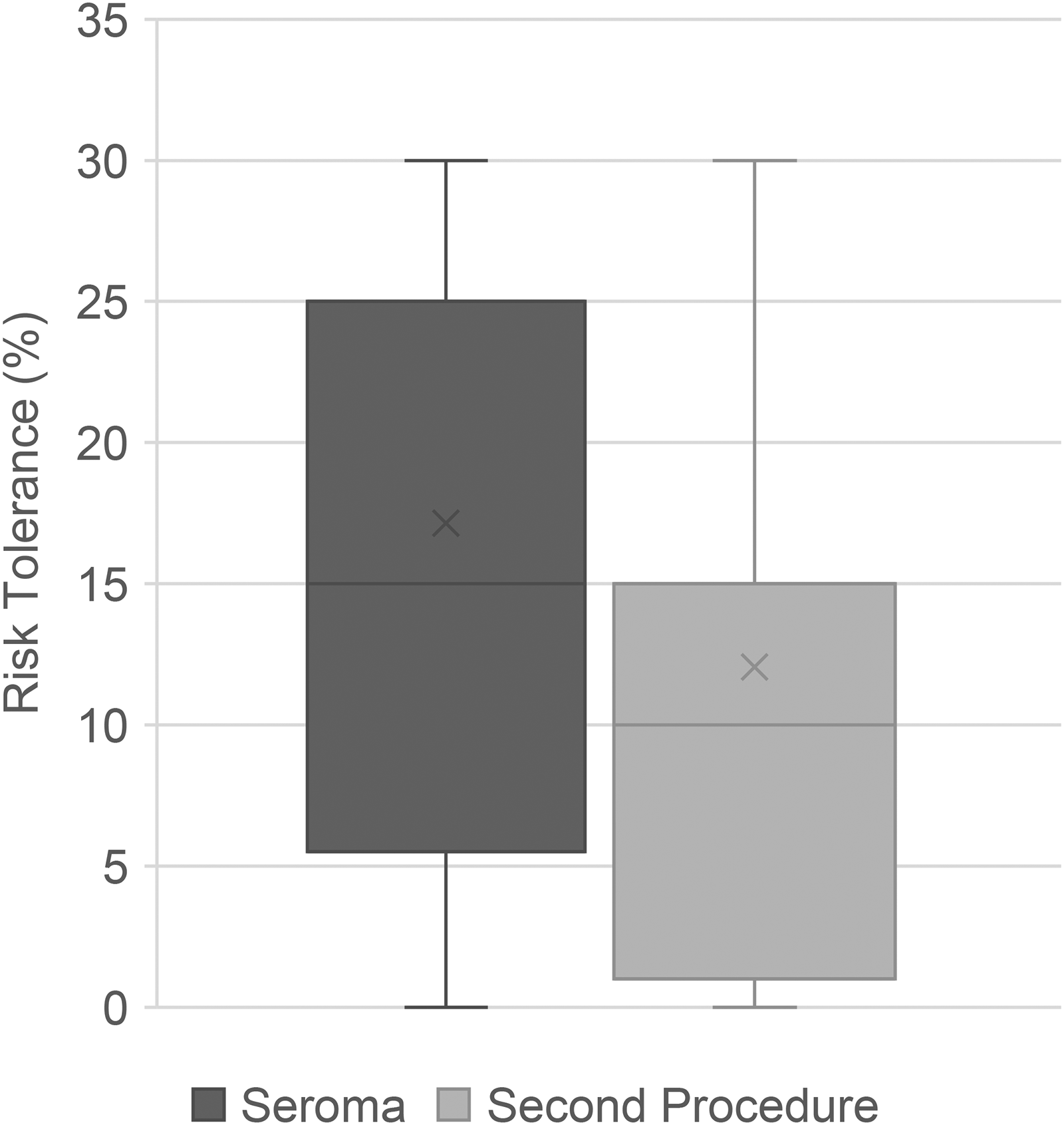
Box plot comparing the risk tolerance for seroma and second procedure.
Subgroup Analysis
Participants with a history of gender-affirming mastectomy demonstrated a risk tolerance for seroma formation that was nearly identical to those without prior surgery (p = 0.867). Similarly, the willingness to accept the risk of requiring a second procedure showed minimal variation between the 2 groups (p = 0.659).
Risk tolerance was further examined across age groups, with no significant differences observed for both seroma risk (p = 0.974) and need for second procedure (p = 0.957).
Supplemental Survey
Supplementary survey findings (Figure 2) identified factors influencing participants’ views on drain placement versus drainless procedures. Patients were most concerned about complications associated with drainless procedures (mean [SD] = 5.1 [0.61]) and concealment challenges with drains (mean [SD] = 6.3 [0.88]).
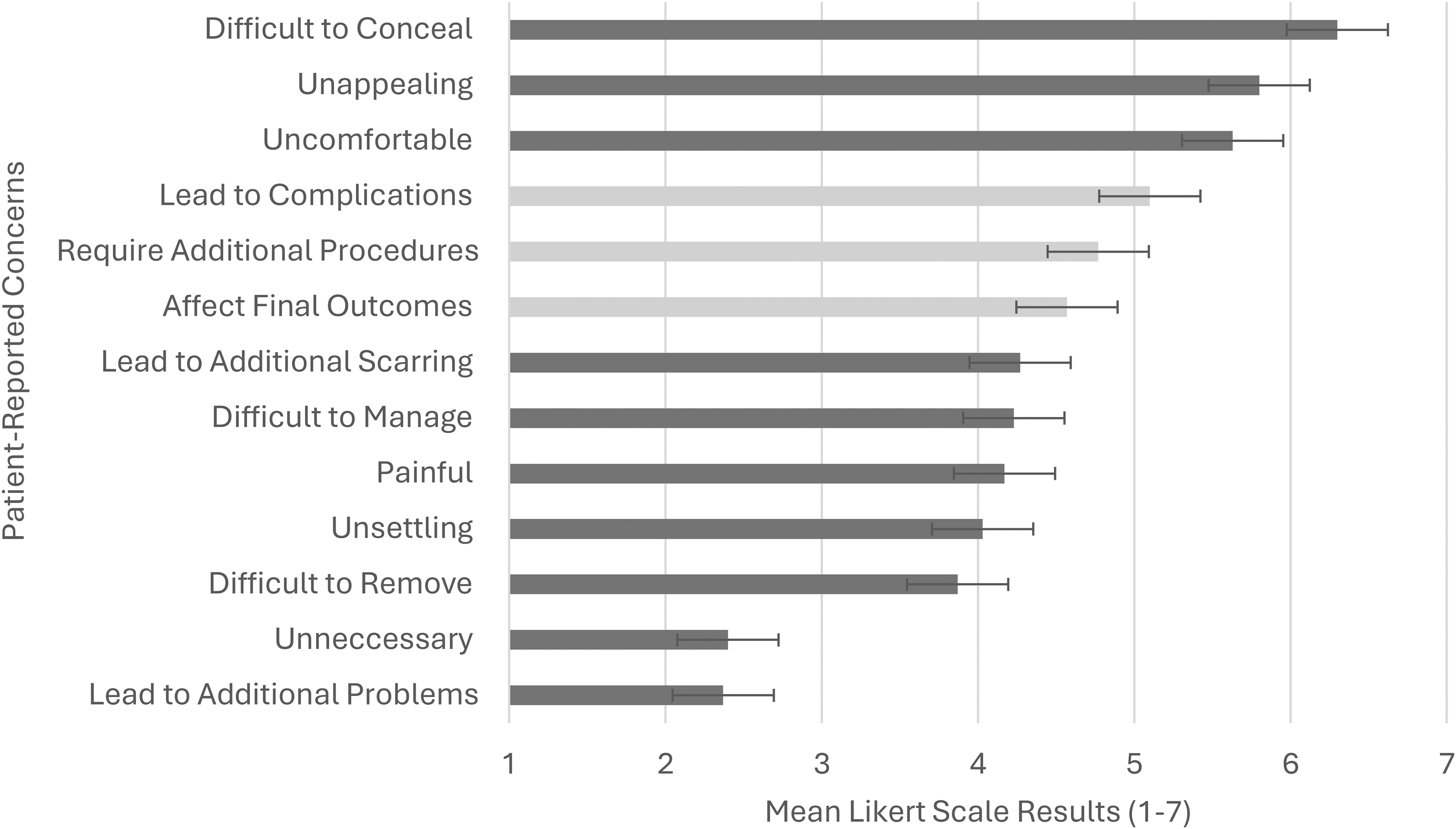
Mean likert scale ratings for participant concerns regarding the presence and absence of postoperative drains. Darker bars represent concerns associated with drain placement, while lighter bars represent concerns associated with drainless procedures. Higher Scores indicate greater concern (1 = strongly disagree, 7 = strongly agree).
Discussion
The role of postoperative drains in gender-affirming mastectomy remains a topic of ongoing debate, with no clear consensus. While systematic reviews comparing drain and drainless techniques in breast surgery exist, they have reported highly variable outcomes—some suggesting a modest reduction in seroma rates with drains, while others show no consistent benefit. Most of these studies, however, focus on mastectomies performed for breast cancer, where patient goals and risk tolerance may differ.
A systematic review by Janis et al, 2 analyzing 14 randomized controlled trials (2263 breast cancer patients), examined the impact of closed-suction drains on postoperative seroma formation. Of these studies, 4 found a significant reduction in seroma rates with drains, while 10 did not. However, when the data were aggregated, there was a significantly lower incidence of seromas in patients with drains (18.5%) compared to those without drains (27%) (p < 0.001). Notably, this patient population primarily included individuals undergoing mastectomy and axillary lymph node dissection, rather than simple mastectomy. Another systematic review by De Rooij et al, 12 analyzing 8 studies on mastectomy in breast cancer patients, similarly found no significant difference in symptomatic seroma rates between drain and no-drain groups (odds ratio: 0.90; 95% CI: 0.42–1.94). Symptomatic seromas occurred in 13%–57% of patients with drains and 7%–67% of patients without drains, again reflecting substantial variability in outcomes.
Studies examining patients undergoing gender-affirming mastectomy are limited to retrospective studies, but further reflect inconsistency in the evidence. A retrospective chart review by Gallagher et al 13 of 153 patients undergoing gender-affirming chest surgery found that drainless techniques were associated with lower rates of hematoma, infection (2%), wound dehiscence (1%), and nipple necrosis (0.7%), with no reported cases of seroma. The authors compared their series to a historical cohort of mastectomy patients with drains (n = 1334), the drainless group had significantly lower rates of hematoma (0.3% vs 2.9%, p = 0.0036), acute reoperation (0.3% vs 3.1%, p = 0.0024), and revision surgery (2.6% vs 8.7%, p = 0.0001), along with a shorter hospital stay. No comment was made regarding differences in rates of seroma. It is important to note that most comparative studies on drain use in breast surgery rely on historical data, are confounded by patient factors and heterogeneity, and are further limited by variation in surgical technique.2,12,13
While these studies highlight variability in the reported rate of seroma formation with and without the use of drains, our study found that the median seroma risk patients were willing to accept to avoid postoperative drains was 15%. When the risks of seroma exceeded this threshold, patients preferred postoperative drains. This may be contrary to the prevailing perception that patients universally dislike drains and suggests that surgeons may use this data to guide counseling and drain use based on their observed seroma risk. These findings underscore the importance of individualized preoperative counseling that incorporates both clinical evidence and patient preferences.
Patients with and without a history of prior gender-affirming mastectomy demonstrated similar levels of risk tolerance for seroma formation and secondary procedures. This suggests that having prior surgery experience may not strongly influence decision-making, though the study was not powered to detect a difference. This consistency between groups strengthens our findings, suggesting that patients can make informed decisions even without prior surgical experience.
Beyond objective risk tolerance, the supplementary survey findings provide additional insights into patient concerns. Participants expressed concern about drainless procedures, particularly regarding the risk of complications and the potential need for a secondary procedure. In contrast, concerns about drains were centered around discomfort and concealability. These findings reinforce prior research on negative perceptions of drains while also highlighting that some patients prioritize minimizing postoperative complications over avoiding the inconvenience of drains.
Given the lack of definitive clinical evidence favoring the use of drains or not, patient perspectives should be incorporated into surgical planning. However, decision-making is inherently influenced by the framing of risks and benefits. Our findings, therefore, support individualized discussions as a complement to clinical judgment and professional opinion.
Limitations and Future Directions
This study provides valuable insight into patient risk tolerance following gender-affirming mastectomy; however, some considerations should be noted. Given that the study was conducted among adolescents, the results may not be generalizable to older populations or those considering other surgical procedures. As with all patients, capacity for consent should be assessed individually, as the ability to understand risks and benefits can vary. All participants were older adolescents with an average age just over 17 years and were judged to have capacity, but this may not be the case for younger adolescents or all patient groups. Future research should explore whether similar patterns of risk tolerance exist in other gender-affirming surgeries or broader reconstructive procedures.
Conclusion
The results of this study highlight the importance of shared decision-making in gender-affirming mastectomy, recognizing both quantitative risk tolerance and qualitative patient concerns. Participants demonstrated greater willingness to accept seroma formation, with a median risk tolerance of 15%, compared to re-intervention, for which the median acceptable risk was 10%. Based on prior research showing variable seroma rates with drainless techniques, these findings suggest that a significant portion of patients may not be comfortable accepting the level of risk reported in the literature. These insights can help guide nuanced, patient-centered conversations about drain use. Strengths of this study include the use of a validated decision analysis method, a clinically relevant patient sample, and a focus on a population historically underrepresented in surgical outcomes research.
Footnotes
Author Contributions
Sumeet Sekhon: Study design, data collection, analysis, and manuscript drafting. Vincent Dinh: Data collection and manuscript review. Nicolas Mitsakakis: Statistical analysis, interpretation of results, and manuscript review. Kevin Cheung: Supervision, study design, and manuscript review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the Helsinki Declaration. This study was approved by the Research Ethics Board of the Children's Hospital of Eastern Ontario (Protocol No. 24/33X).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from all participants.