
Abstract
Facial nerve palsy affecting the lower face may compromise essential functions such as speech and eating. The associated facial asymmetry can contribute to social isolation. Facial nerve reconstruction using a combination of interposition nerve grafts and/or nerve transfers offers significant improvement. However, these options are limited by insufficient donor nerves and unwanted synkinesis if a single donor nerve is used for the entire hemi-face. To ameliorate both limitations, we perform an ansa cervicalis to marginal mandibular nerve transfer to restore tone and symmetry to the lower third of the face. We have found this a safe and feasible technique with minimal donor site morbidity. The anatomy is favorable both in terms of donor nerve length and size match between nerves. We report 9 cases with at least 6 months follow up which demonstrate improved lower lip tone and symmetry and improved oral competence. Early donor site morbidity and postoperative complications are minimal. This method is a reliable adjunct in facial nerve reconstruction to address the marginal mandibular nerve paralysis.
Introduction
Facial nerve palsy affecting the lower face may compromise essential functions such as speech and eating. The associated facial asymmetry can contribute to social isolation. Facial nerve reconstruction using a combination of interposition nerve grafts and/or nerve transfers offers significant improvement. 1 However, these options are limited by insufficient donor nerves and unwanted synkinesis if a single donor nerve is used for the entire hemi-face. To ameliorate both limitations, we perform an ansa cervicalis to marginal mandibular nerve transfer to restore tone and symmetry to the lower third of the face. We have found this a safe and feasible technique with minimal donor site morbidity. The anatomy is favourable both in terms of donor nerve length and size match between nerves. We report 9 cases with at least 6-month follow-up, which demonstrate improved lower lip tone and symmetry and improved oral competence. Early donor site morbidity and postoperative complications are minimal. This method is a reliable adjunct in facial nerve reconstruction to address the marginal mandibular nerve paralysis.
An innovative nerve transfer for lower lip facial reanimation is presented whereby the superior root of the ansa cervicalis is transferred to the marginal mandibular branch of the facial nerve with the goal of improving lower lip tone and symmetry, as well as improving oral competence. This approach has not been well described in the existing literature.2–4 A major advantage of this technique compared to the well-described hypoglossal-to-facial nerve transfer is the preservation of lingual function.5–7
Anatomy
The ansa cervicalis has a dual origin that forms a nerve loop.8–10 The superior root originates from the C1 ventral ramus, travels with the hypoglossal nerve, then leaves to descend on the carotid sheath, giving off a motor branch to the superior belly of the omohyoid muscle.9,10 The inferior root originates from the C2 and C3 ventral rami, which descends to the level of the origin of the occipital artery, where it joins the superior root via the ansa cervicalis proper. 11 This area of the ansa cervicalis gives off motor branches to the sternothyroid, sternohyoid, and inferior belly of the omohyoid muscles9,10 (see Diagram 1). The infrahyoid muscles play an active role in swallowing through movement of the larynx. 12 The thyrohyoid muscle is not innervated by the ansa cervicalis and, therefore, helps preserve the function of swallowing. 12 The morbidity of a transection of the ansa cervicalis is thought to be minimal.2,13,14
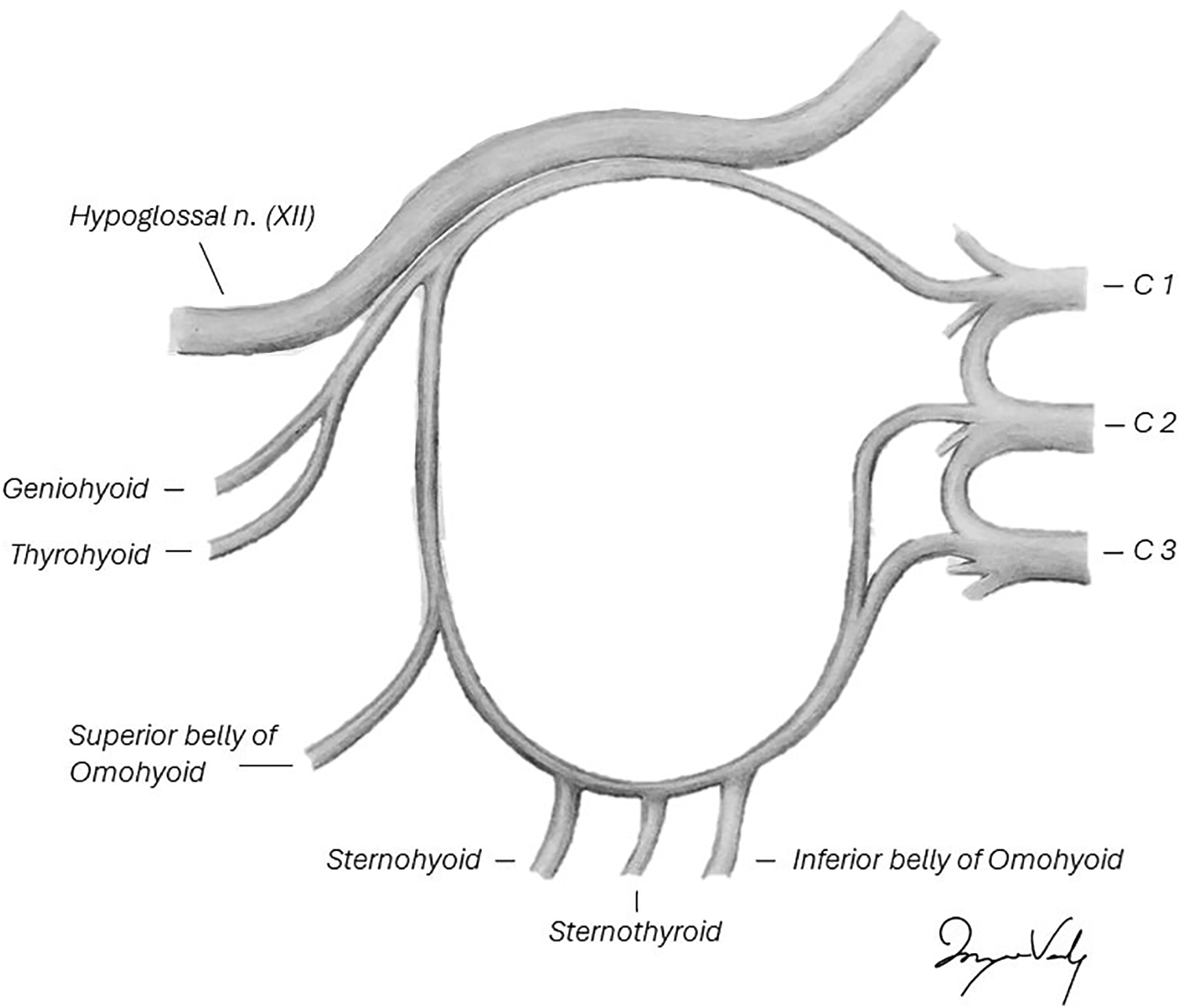
Ansa cervicalis anatomy. Legend: Anatomical illustration of the ansa cervicalis origin, course, and branches.
Technique Description
An extended facelift incision that incorporates a transverse neck crease is used, and skin flaps are elevated deep to the superficial musculoaponeurotic system (SMAS) and platysma. The marginal mandibular branch of the facial nerve is identified at the anterior-inferior border of the parotid gland in conjunction with buccal and zygomatic branches. The anterior border of the sternocleidomastoid muscle is identified and reflected laterally to expose the superficial border of the internal jugular vein, which is then exposed in a cephalad direction. Dissection is continued between the sternocleidomastoid muscle and internal jugular vein, and here the superior ramus of the ansa cervicalis can be identified running in a vertical direction (see Figure 1). The superior root is found in close relation to the internal jugular vein.8,15 A handheld nerve stimulator confirms that stimulation of the superior ramus is associated with activation of the infrahyoid muscles. The superior ramus is then followed to its take off from the inferior border of the hypoglossal nerve. Once an adequate length of the proposed nerve transfer is ascertained, the ansa cervicalis nerve is divided caudally. The inferior root is left in continuity and thus may still provide nerve input to the sternothyroid, sternohyoid, and inferior belly of the omohyoid muscles. The length is sufficient, 4 and the diameter a suitable match for the marginal mandibular branch of the facial nerve (see Supplemental Video 1 [Accessible online at https://journals.sagepub.com/doi/full/10.1177/22925503251386749]). If the intention is to harvest the ansa cervicalis at the time of oncologic neck dissection in the setting of head and neck cancer, it is important to communicate to the ablative surgeon the need to preserve the full length of the ansa cervicalis.
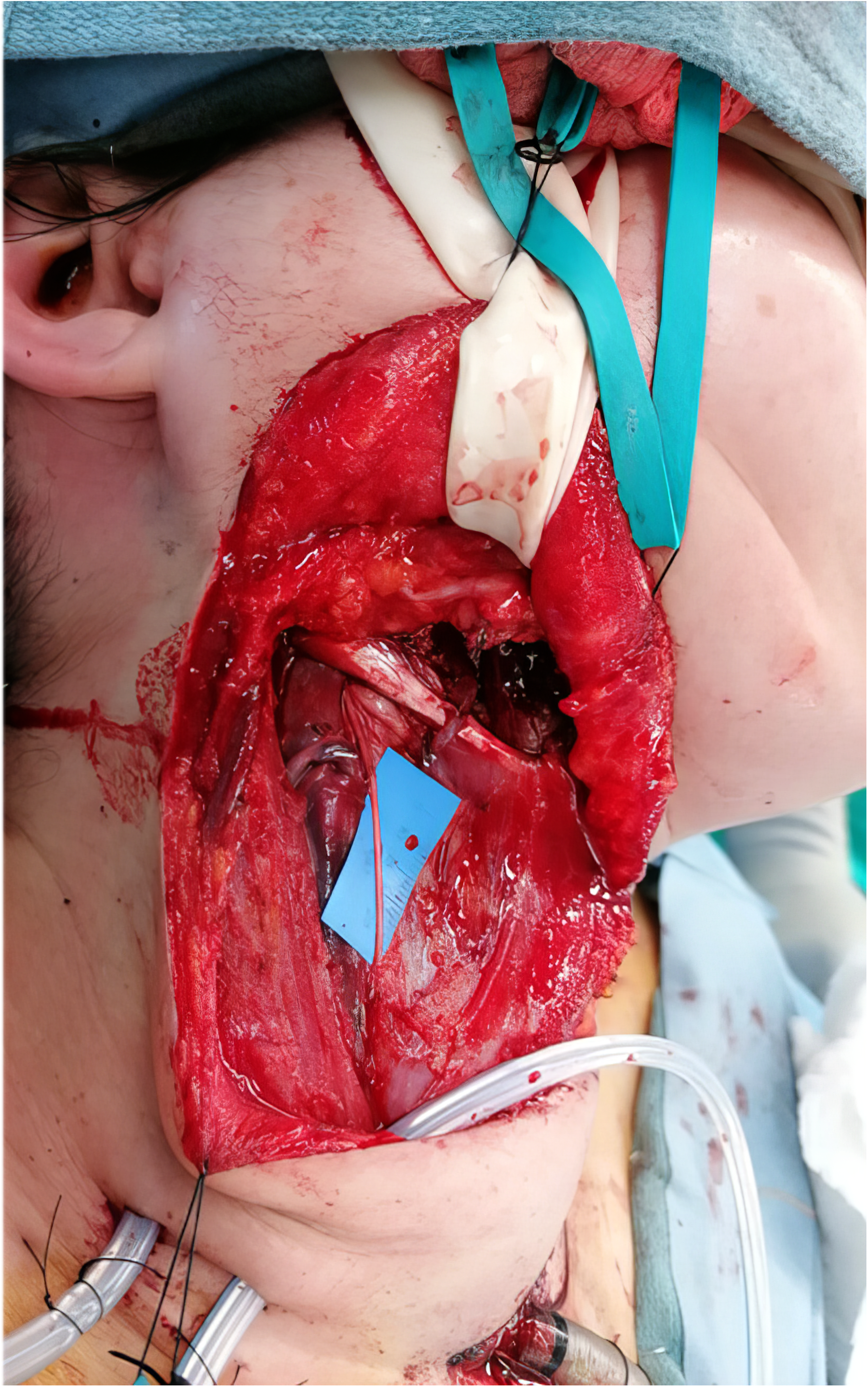
Ansa cervicalis dissection. Legend: The superior root of the ansa cerviclis nerve can be found running in a vertical direction, in close relation to the sternocleidomastoid muscle.
Results
Nine ansa cervicalis to marginal mandibular nerve transfers were performed between 2021 and 2024 (see Table 1). Mandibular nerve palsy was part of a complete facial nerve palsy in all cases; that is, we did not do isolated marginal mandibular nerve palsy cases. In all cases, the nerve transfer was anatomically possible, and the nerve repair was completed without tension. In all cases, the ansa cervicalis was a good match to the marginal mandibular nerve in terms of size. No early postoperative complications or donor site morbidities were documented in any of the 9 patients.
Results.
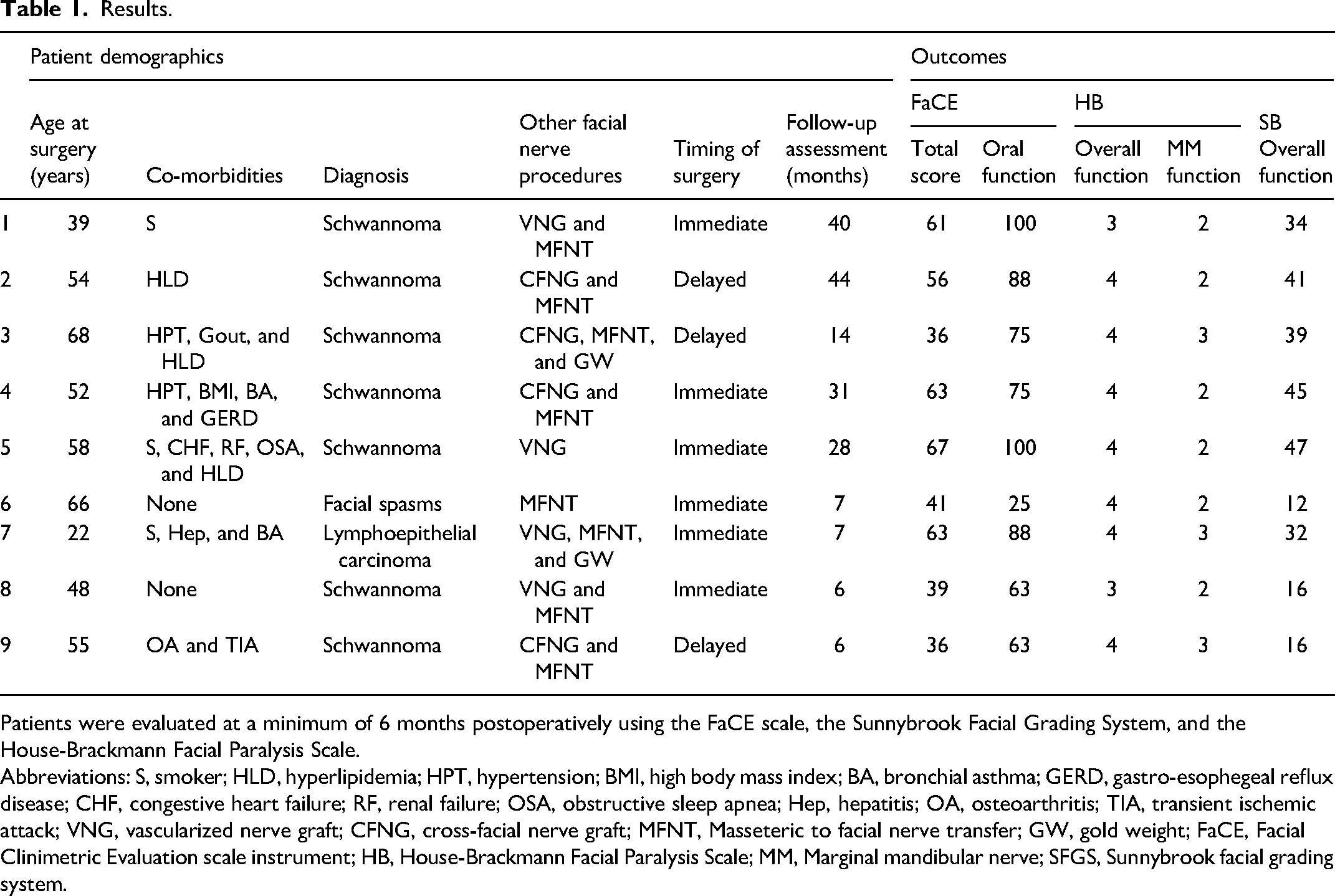
Patients were evaluated at a minimum of 6 months postoperatively using the FaCE scale, the Sunnybrook Facial Grading System, and the House-Brackmann Facial Paralysis Scale.
Abbreviations: S, smoker; HLD, hyperlipidemia; HPT, hypertension; BMI, high body mass index; BA, bronchial asthma; GERD, gastro-esophegeal reflux disease; CHF, congestive heart failure; RF, renal failure; OSA, obstructive sleep apnea; Hep, hepatitis; OA, osteoarthritis; TIA, transient ischemic attack; VNG, vascularized nerve graft; CFNG, cross-facial nerve graft; MFNT, Masseteric to facial nerve transfer; GW, gold weight; FaCE, Facial Clinimetric Evaluation scale instrument; HB, House-Brackmann Facial Paralysis Scale; MM, Marginal mandibular nerve; SFGS, Sunnybrook facial grading system.
All 9 patients were seen for a follow-up evaluation at a minimum of 6 months postoperatively. We assessed patients using the Facial Clinimetric Evaluation (FaCE) scale, 16 the Sunnybrook Facial Grading System (SB), 17 and the House-Brackmann Facial Paralysis Scale (HB). 18 Both the FaCe scale and the SB were scored out of 100, with 100 being normal facial function.16,19 The HB is scored from 1 to 6, with 1 being normal facial function. 18 To help assess the lower lip more directly, we calculated an overall facial score using the FaCe scale as well as an oral function score in isolation. As shown in Table 1, 8 out of 9 patients scored above 60 with the oral function component, and of these, 4 patients scored above 80. When using the HB scale, we scored the overall facial function as well as the marginal mandibular function in isolation. All patients scored 3 or lower when the marginal mandibular branch was evaluated in isolation. All patients exhibited good function of the marginal mandibular branch using SB, with good lower lip tone and oral competence.
Pre- and postoperative images of a patient receiving ansa cervicalis to marginal mandibular nerve transfer, cross-face nerve graft, and masseter to buccal branch nerve transfers demonstrate good improvement (see Figure 2). A major improvement is seen in symmetry and lower lip tone. The lower lip height is similar to the normal side position when compared to the preoperative photograph.

Pre- and postoperative photographs. Legend: Pre- and postoperative images of a patient receiving ansa cervicalis to marginal mandibular nerve transfer, cross-face nerve graft, and masseter to buccal branch nerve transfers demonstrate good improvement.
Electromyography demonstrates that lower lip musculature is innervated via the nerve transfer (see Supplemental Video 2 [Accessible online at https://journals.sagepub.com/doi/full/10.1177/22925503251386749]). The lower lip is activated by the swallow activation. Notably, no patient complained of donor site concerns.
Discussion
Facial nerve palsy is a debilitating state in which the essential functions of eating, speaking, and expressing emotions are compromised.20–22 Most efforts for reconstruction have been focused on the periorbital and midface areas to protect the eye from excessive exposure to the external environment and to create a socially acceptable smile.23,24 The marginal mandibular branch is often neglected in facial nerve reconstruction, even though its paralysis can result in asymmetry and drooping of the lower lip, which may in turn affect speech, oral competence, and emotional expression.23,24
This unique technique of lower lip facial reanimation, using a nerve transfer from the superior ramus of the ansa cervicalis to the marginal mandibular nerve, can provide lower lip tone and symmetry, and thereby improve oral competence. Reinnervation occurs between 5 and 6 months, demonstrated clinically as improved commissure and lower lip position or by EMG study.
Ansa to marginal mandibular nerve transfer is now standard of care in Calgary for complete facial nerve reconstruction in young patients presenting at < 9 months from inciting paralyzing event, as it is associated with few negative consequences and helps lower lip position and function.
Limitations
This retrospective study is limited by the absence of a control group and the lack of formal preoperative functional assessment. In all cases, the marginal mandibular nerve was completely transected, and function was therefore assumed to be zero. Further prospective studies with appropriate control groups are planned to evaluate our results more objectively and strengthen the evidence base.
Supplemental Material
Supplemental Material
Footnotes
Previous Presentations
APRASSA Congress & ISAPS Symposium on Facial Aesthetics, Cape Town, South Africa; October 5, 2024—Awarded second place for Best Clinical Paper.
Acknowledgments
We acknowledge Myriam Verly, MD, for her contribution in drawing the anatomy illustration featured in this article.
Consent Statement
All patients provided written consent for the publication of their information and images/videos.
Authors’ Contributions
Marieta Van der Vyver: author, data collection, evaluation of patients, and surgical team. Eva Lindell-Jonsson: literature review, and review and editing. Kristin N. L. Bell: post op evaluation of patients. Ashvir Singh: data collection and surgical team. Shamir P. Chandarana: review and editing and surgical team. Alan Robertson Harrop: review and editing. Robert D. Hart, Wayne T. Matthews, Ashley Hinther, Charles David McKenzie, and Jennifer K. L. Matthews: surgical team. Christiaan Schrag: principal investigator, technique description, review and editing, and surgical team.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this paper is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.