
Abstract
Introduction
Hand fractures are common injuries in the pediatric population, occurring at rates of 448 per 100 000 children per year. 1 Children have the capacity for faster healing, better remodeling, and reduced rates of nonunion compared with their adult counterparts. 2 With only approximately 10% requiring surgical intervention, 3 most simple pediatric hand fractures can be treated with immobilization alone with splints or casts, yielding good clinical outcomes and complete bony healing in 3 to 4 weeks.4,5
A recent institutional audit identified that there was significant practice variation between surgeons managing children with simple hand injuries (ie, those not requiring surgical intervention) in terms of number of follow-up visits. For similar hand injuries, some surgeons would see a patient 2 to 3 times, while others would only see the patient once. Therefore, it is prudent to standardize care for children with simple injuries, resulting in fewer unnecessary follow-up visits and improved utilization of healthcare resources.
The objective of this study was to implement and assess a streamlined care pathway to manage children with “simple” hand injuries.
Methods
A single institution prospective study was conducted at a tertiary pediatric centre to test a streamlined care pathway for children with simple hand injuries. Based on a related retrospective review recently conducted at our institution, a sample size of convenience of 100 participants was used to determine the study duration. All patients who presented to the Plastic Surgery clinic from September to November 2021 were screened for inclusion. At our institution, all injuries distal to the carpus are referred to the plastic surgery clinic.
Simple hand injuries were defined based on previous literature,3,4 retrospective review, and expert consensus. The following hand injuries were classified as simple and included: volar plate avulsion fractures with no proximal interphalangeal (PIP) joint instability, proximal and middle phalanx Salter-Harris type 2 fractures, metacarpal neck fractures, unicortical fractures, PIP dislocations, and thumb MCP dislocations or ligamentous injuries without avulsion fractures. Patients were excluded if they had subacute injuries (presenting >28 days post-injury), open injuries, fractures requiring reduction, multiple fractures/injuries, patients requiring cast immobilization, patients with comorbidities that may preclude normal healing (osteogenesis imperfecta, immunosuppression), or if they were unable to complete telephone follow-up in English or French.
A streamlined care pathway for children with simple hand injuries was developed with input from surgeons, therapists, nurses, parents, and hospital administration (Figure 1). Patients were initially assessed and treated according to standard practice, including thermoplastic splint or buddy taping treatment. Patients and parents received both verbal and written instruction from the attending surgeon on care and reasons to seek follow-up (Appendix, Supplemental Digital Content 1). The written instructions were reviewed by all surgeons, hand therapists, and the hospital communications staff who also assisted with translation of the instruction sheet to French. No routine in-person follow-up was arranged. Participants were then contacted by telephone approximately 6 weeks post-injury to review their course and outcomes and identify if they had any concerns or need for follow-up. During this call, patients or parents completed a modified version of the brief Michigan Hand Questionnaire (MHQ) with questions adapted for a pediatric population and specifically addressing hand (rather than wrist) function (Appendix, Supplemental Digital Content 2). This included 11 items with responses on a 1 through 5 Likert scale regarding several aspects of hand function. All items were totaled and then normalized to generate a summary score on a scale of 0 to 100. Higher scores indicated better overall functioning and satisfaction. After completing the modified MHQ, participants were also asked to rate their satisfaction regarding the care they received on a 5-point scale from very dissatisfied to very satisfied.
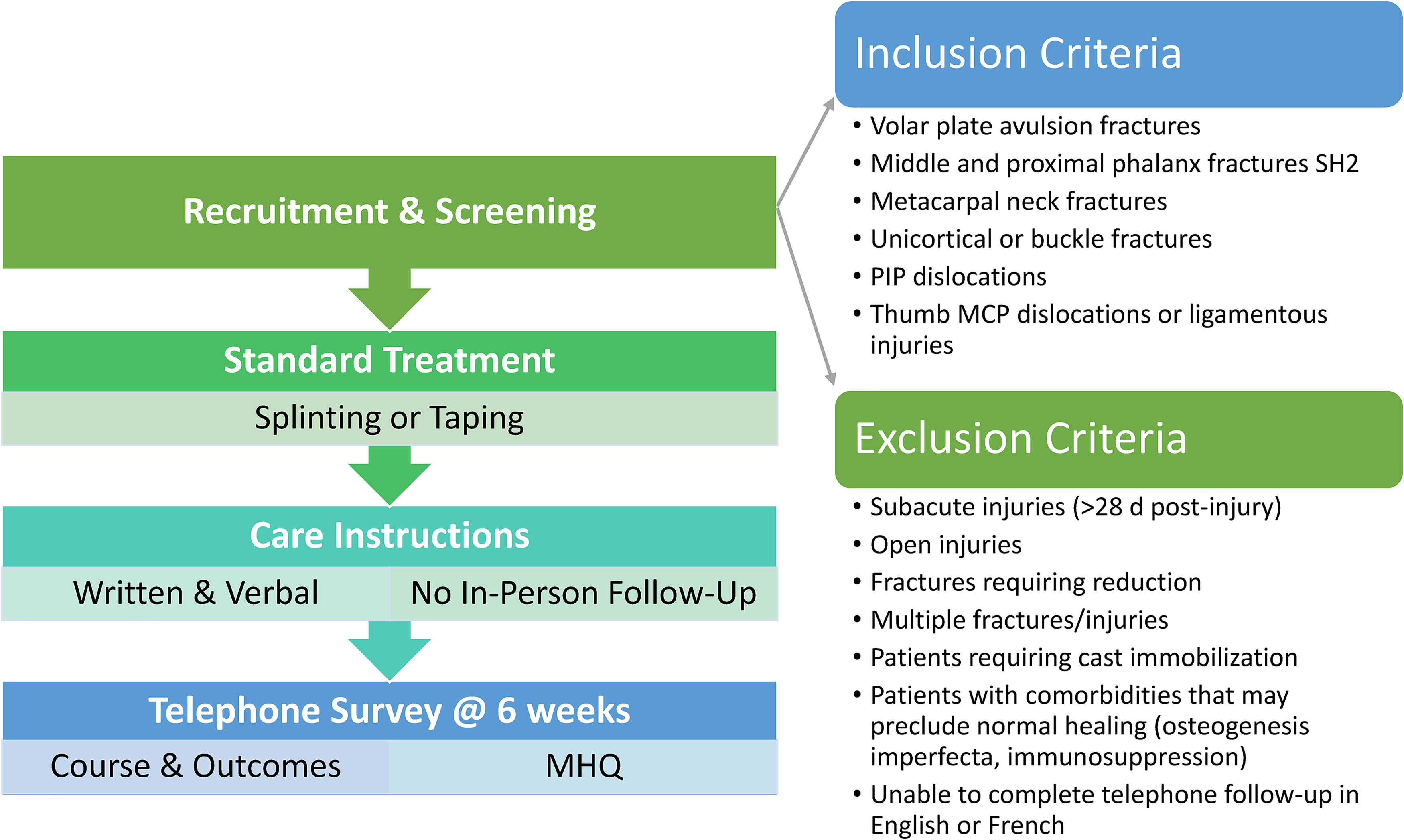
A flow diagram of the proposed streamlined care pathway for simple pediatric hand trauma.
The primary outcome of the study was the number of patients requiring follow-up visits. Secondary outcomes included change in treatment plan, modified MHQ scores, patient satisfaction, and number of follow-up visits saved. Descriptive statistics were used to characterize the population and, in particular, those patients requiring or requesting follow up.
Results
Of the 249 patients who presented to the CHEO plastic surgery clinic with hand injuries during the study time frame, 103 (41%) met the inclusion criteria for simple hand injuries and were approached to take part in the study. Two patients declined study participation, resulting in a sample size of 101 patients.
The majority of the patients were secondary school age (59%), male (64%), and had either fallen during an activity or had something hit their hand (64%). Seventy-six percent had open growth plates, and 74% received splinting treatment in clinic. The most common injury sustained was proximal phalanx Salter-Harris type 2 fractures (28%), followed by volar plate avulsion fractures (18%), metacarpal neck fractures (16%), and unicortical fractures (13%) (Table 1).
Participant Characteristics.
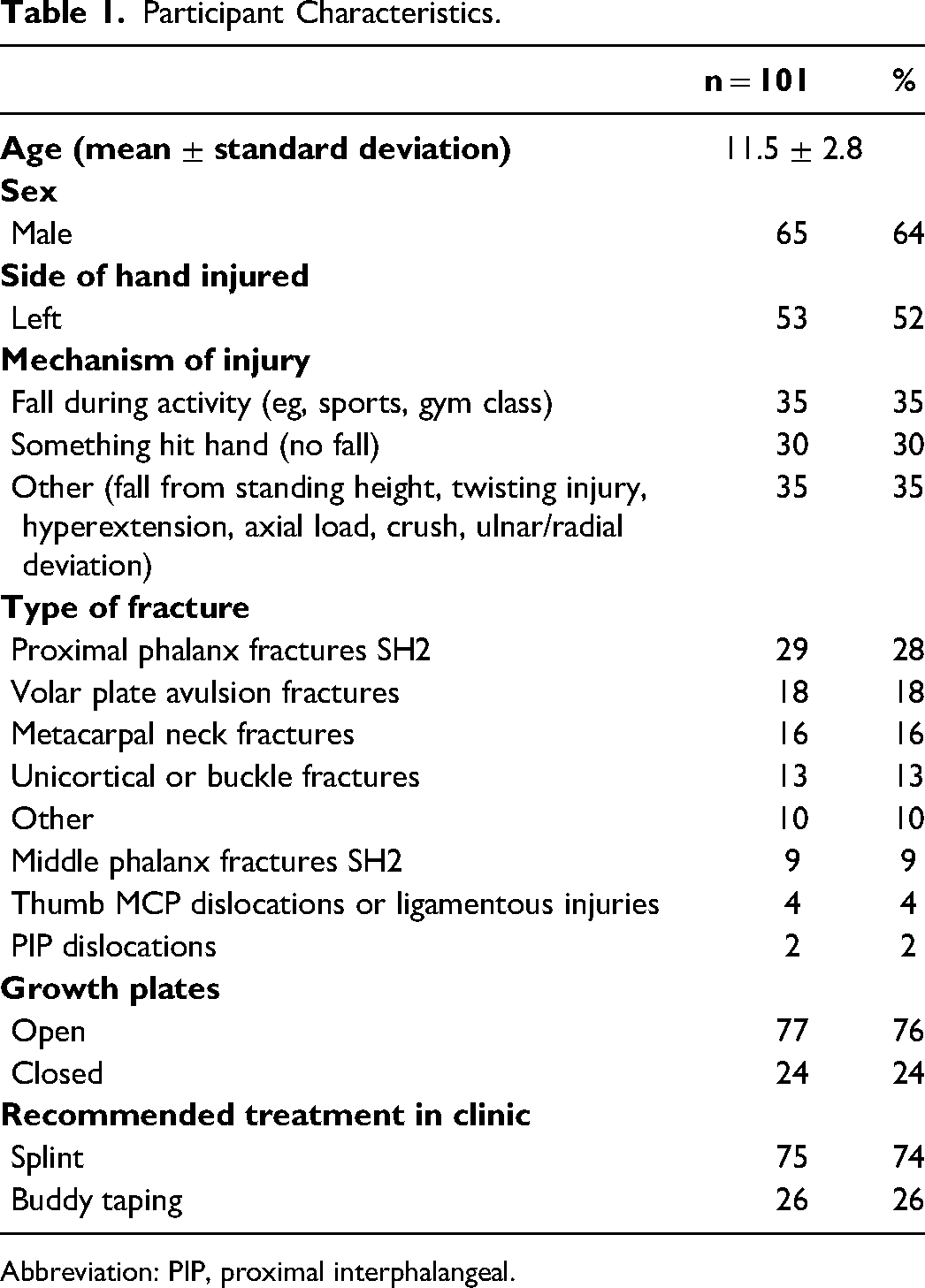
Abbreviation: PIP, proximal interphalangeal.
Telephone Follow-Up
Sixty-one patients (60%) completed the telephone follow-up (Figures 2 and 3). The remaining 40% were unreachable after 2 to 3 attempts. Fifty-five (90%) patients did not report problems during healing, and 52 (85%) had resumed all activities without limitations. Of the 9 patients who had not resumed all pre-injury activities, 4 sustained PIP volar plate avulsion fractures and 2 sustained thumb and finger Salter-Harris 2 proximal phalanx fractures. The remaining 3 sustained a unicortical fracture, middle phalanx fracture, and metacarpal neck fracture. Fifty-eight (95%) patients were satisfied with the appearance of their hand; the remaining 3 patients who were not satisfied sustained PIP-related injuries (2 volar plate avulsion fractures and 1 PIP dislocation). In other words, 44% of patients who had not resumed all activities and all patients with low satisfaction regarding appearance had injuries involving the PIP joint. A total of 10 (16%) patients, including 7 of the 9 patients that had not resumed all preinjury activities, requested a follow-up visit, but 4 did not show or cancelled. The remaining 6 (60%) were all provided with reassurance and none required any change in treatment plan. No involvement of hand therapy was required aside from initial fabrication of removable thermoplastic splints.
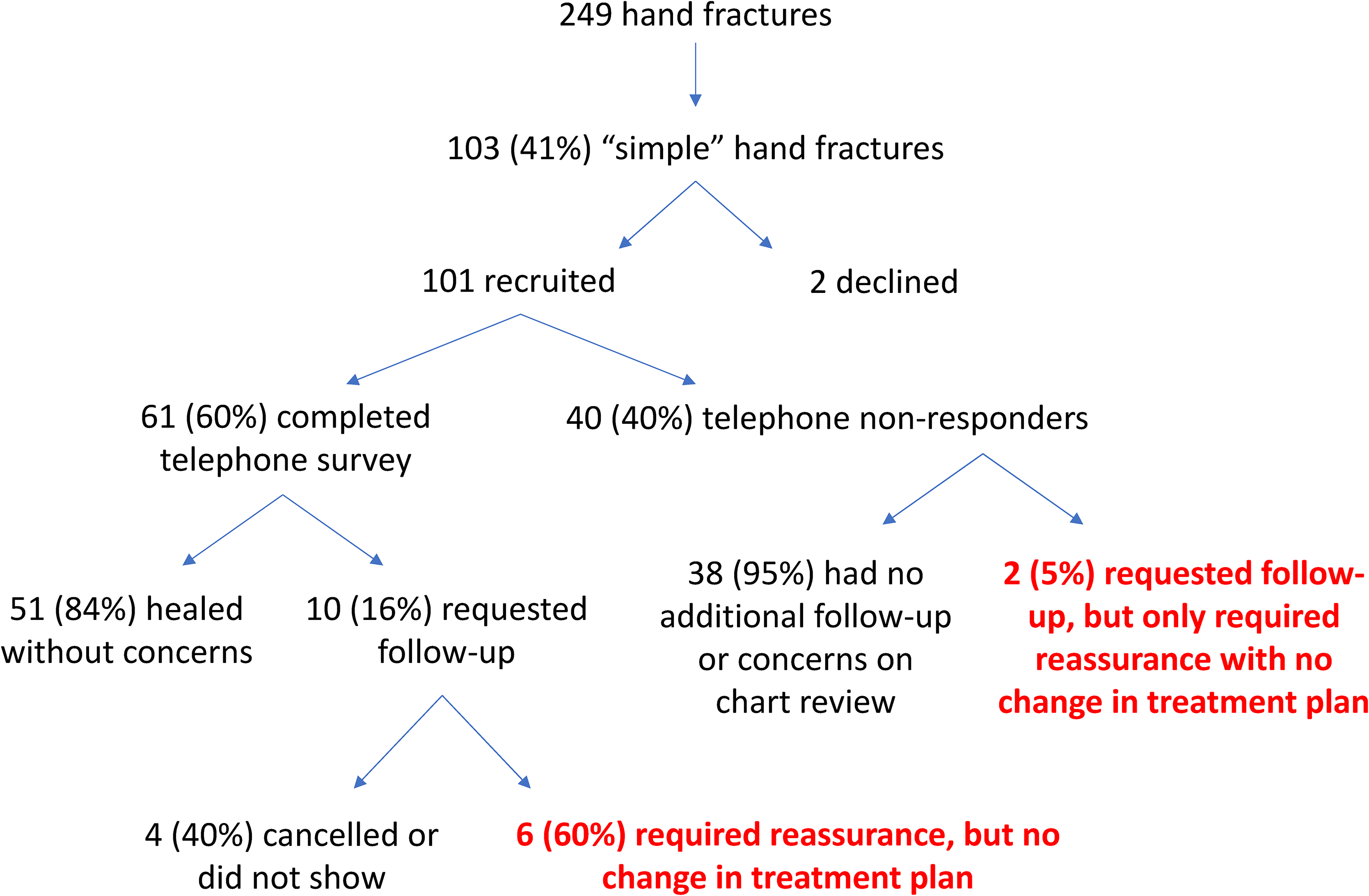
A flow diagram of the study results.
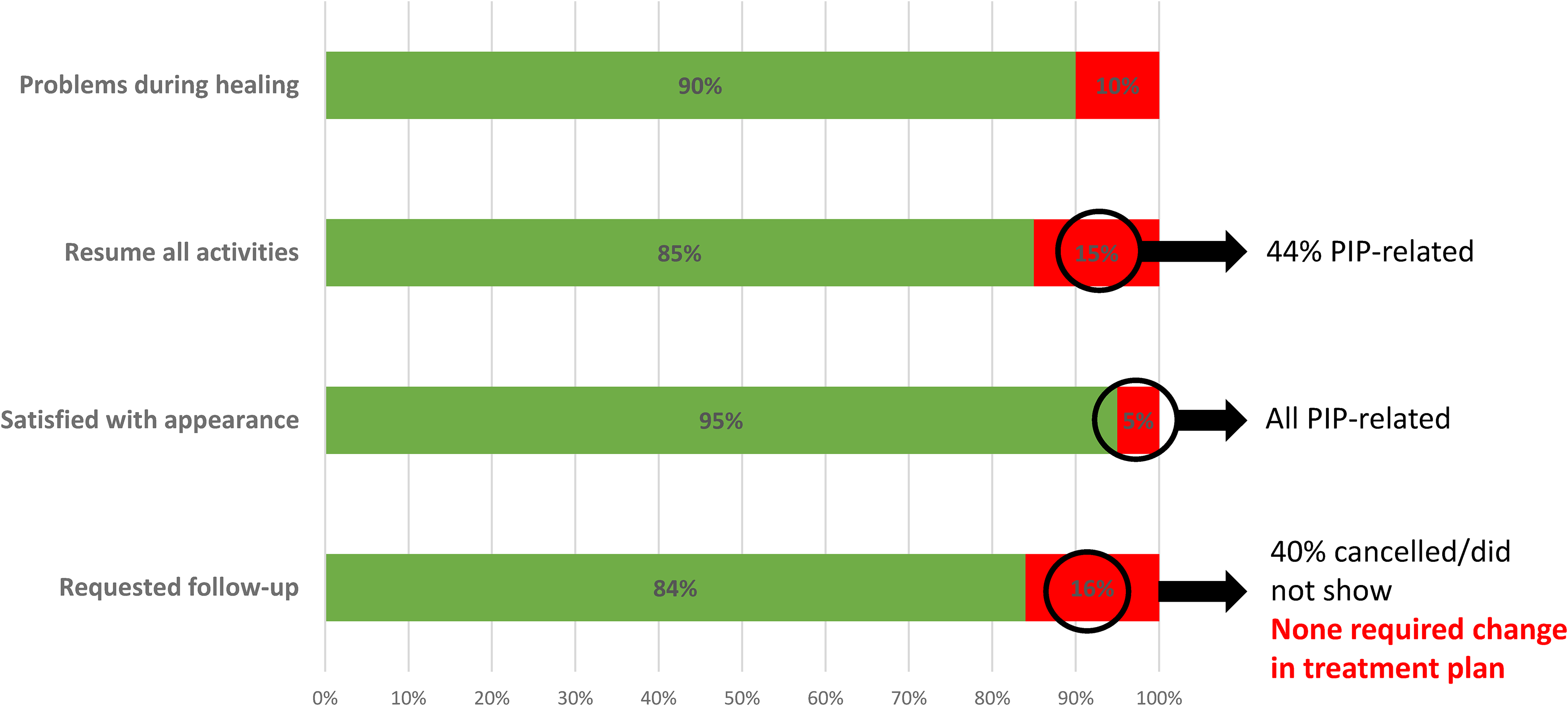
A bar diagram of the telephone follow-up results.
For participants that were unable to be reached for telephone follow up, electronic patient charts were reviewed 6 months after injury to determine if any complications or unintended visits occurred. Two of the 40 patients that did not respond for telephone follow up requested additional in-person follow-up—one for residual PIP swelling without associated pain and the other for parental concern of ongoing pain despite no reported pain by the patient. In these 2 cases, only reassurance was required with no change in treatment plan.
The mean modified MHQ score was 82.2 ± 25.2. Nine (15%) patients had a normalized summary score less than 50 with lower scores in sensation and appearance affecting daily activities (mean 2.9 ± 0.6 and 3.1 ± 1.2 out of 5, respectively).
Regarding patient satisfaction, 58 (95%) of the 61 telephone responders were “very satisfied” with the care they received. The remaining 3 patients were “somewhat satisfied” with no patients reporting being dissatisfied.
Visits Saved
During the study period, there were 406 total clinic visits related to the 249 hand injury patients. This included the 101 patients participating in the pathway. Assuming that each study participant would require a minimum of 1 follow-up visit in addition to the initial consultation prior to implementation of the hand pathway, 101 visits (22%) were saved.
Discussion
Hand injuries are common injuries in the pediatric population. A significant proportion of pediatric hand injuries do not require surgery and can be treated with immobilization or early protected motion alone.3,4 A lack of consistency in treating simple hand injuries may lead to many being overtreated with unnecessary follow-up visits and excessive utilization of healthcare resources. This study introduced a streamlined care pathway to simplify and safely guide management of children with “simple” hand injuries, allowing for standardized care for children with hand injuries and ultimately fewer follow-up assessments in busy fracture clinics.
The demographics and characteristics of the pediatric hand injuries in this study are consistent with those reported previously in the literature.3,6,7 Fractures of the pediatric population appear to be twice as common in boys than girls, and Salter-Harris Type II fractures were the most common fracture pattern. Common mechanisms of injury included sport-related injuries, falls, and direct impact injuries.
Overall, patients in the streamlined care pathway did well. The majority were satisfied, had resumed normal function, and did not require additional follow up or radiographs. Our study results also reinforced the notoriously challenging nature of PIP injuries. 8 Forty-four percent of patients who had not resumed all activities and all patients with low satisfaction regarding appearance had injuries involving the PIP joint. None of the patients requesting or seen for reassessment, however, required any surgical intervention or change in management. The PIP joint has a well-known predilection for stiffness, pain, arthritis, and residual deformities caused by soft tissue imbalance or adhesions. 9 To address this, we have amended the instruction sheet and our discussion with patients and parents to set appropriate expectations specifically for PIP injuries. This includes an understanding that swelling and deformity may persist for several months, and in some cases, may be permanent. Patients and families are still instructed to contact us if pain or limitations in motion persist beyond 8 weeks from injury.
Of the patients who requested follow-up in our study, patients only required reassurance without any change in treatment plan. This suggests that follow-up may not be necessary for a simple hand injury for which complications rarely develop and treatment decisions do not change after initial consultation. By simplifying care of these injuries, implementing this pathway may result in more efficient care with fewer in-person follow-ups and thereby substantial savings for both families and the healthcare system. Follow-up appointments also directly impact the waiting times for other patients. 10 Furthermore, clinical pathways are an important educational resource for physicians; clinical guidelines have been shown to be significantly superior in guiding treatment decisions for pediatric trauma care, compared to commonly available information online and in textbooks. 11
Crawford et al demonstrated the significant cost savings by implementing a clinical pathway for proximal humerus fractures, another fracture often managed nonoperatively, in a single-payer health care system in Ontario, Canada. 10 In this study, costs considered included initial and repeat follow-up orthopaedic assessments, shoulder radiographic series, and associated radiologist assessments. Additional costs to the patient and family associated with missed school/work, child care, and parking were not considered in this study but may be equally important.10,12 Similarly, a recent study by Fucshini et al 13 of both adults and children analyzed the outcomes for management of simple orthopedic injuries after implementation of a primary care pathway without direct orthopedic specialist review. This study demonstrated reduced demand on hospital resources and provided a safe, cost-effective alternative to a resource-restricted specialist outpatient service. In this study, hand injuries including volar plate avulsions, metacarpal fractures, and phalanx fractures were found to be the most common upper limb injury suitable for utilization of the primary care pathway. This suggests the possibility of expanding our current pathway to obviate the need for assessment by a plastic surgeon altogether.
At our centre, simple and stable hand injuries are consistently referred for outpatient plastic surgery follow-up. As demonstrated in both our analysis and existing literature, these injuries rarely require any surgical intervention or change in treatment plan. The majority of patients heal well with education and reassurance. While our study limited itself to the inclusion of specific fracture patterns, Baykan et al report validation of the Calgary Kids’ Hand Rule, a clinical prediction rule for emergency physicians to predict “complex” fractures that require surgical referral (and conversely those that do not). 14 Further development and implementation of such a rule, in conjunction with a streamlined care pathway, may enable broader inclusion and applicability of children with simple hand injuries.
Limitations of this study include its single institution and patient-reported nature of outcomes, perhaps affecting generalizability and objective assessment, respectively. Furthermore, the MHQ was utilized for its convenience, ease-of-use, and established responsiveness; however, it is not validated in the pediatric population, over telephone, or by proxy (parent). In addition, there may be an element of both nonresponse bias and proxy (parent) bias. Due to the risk of nonresponse bias, the results may overestimate the proportion of simple fractures that need follow-up. We attempted to address this by performing a chart review of all the nonresponders 6 months after injury to determine if any complications or unintended visits occurred. Ultimately, further research is required to determine the possibility of expanding the criteria of “simple” hand injuries to include other injuries often managed conservatively, such as nail injuries, mallet fingers, and stable fractures treated with closed reduction alone.
Conclusion
This study suggests that the majority of patients with simple pediatric hand injuries heal well without routine follow-up visits. Care may be streamlined with standardized verbal and written instructions. Uptake of a hand pathway such as this can make a significant quantitative impact by relieving socioeconomic costs and improving healthcare utilization. Proximal interphalangeal injuries, however, may require additional counselling about expectations, such as swelling, stiffness, and time to heal.
Supplemental Material
sj-docx-1-psg-10.1177_22925503241249755 - Supplemental material for Streamlining the Management of Children With Simple Hand Injuries
Supplemental material, sj-docx-1-psg-10.1177_22925503241249755 for Streamlining the Management of Children With Simple Hand Injuries by Lauren Wong, Zina Sabir, Patrick Sachsalber, Yvonne Ying, Claudia Malic and Kevin Cheung in Plastic Surgery
Supplemental Material
sj-pdf-2-psg-10.1177_22925503241249755 - Supplemental material for Streamlining the Management of Children With Simple Hand Injuries
Supplemental material, sj-pdf-2-psg-10.1177_22925503241249755 for Streamlining the Management of Children With Simple Hand Injuries by Lauren Wong, Zina Sabir, Patrick Sachsalber, Yvonne Ying, Claudia Malic and Kevin Cheung in Plastic Surgery
Footnotes
Authors’ Note
Review Committee: Research Ethics Board, Children's Hospital of Eastern Ontario Research Institute. Ethics Committee Reference Number: Protocol 21–104x. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study. Informed consent was obtained from all individual participants included in the study. Presented at: Canadian Society of Plastic Surgeons (CSPS) Annual Meeting; June 2023, Whistler, BC.
Authors Contributions
Dr Lauren Wong contributed to study recruitment, data collection, data analysis, manuscript writing and review, and manuscript submission. Zina Sabir contributed to data collection. Patrick Sachsalber contributed to study organization and data collection. Dr Yvonne Ying contributed to study recruitment and manuscript review. Dr Claudia Malic contributed to study recruitment and manuscript review. Dr Kevin Cheung contributed to protocol writing and submission, REB submission, study recruitment, and manuscript review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.