
Abstract
Introduction
Hand fractures are very common injuries in the pediatric population and make up one of the most frequent fracture presentations to the emergency department. 1 Bony fracture in this population tend to heal well and hand fractures are no exception. 2 Hand fractures in the pediatric population are often well managed with immobilization alone, but a small subset require surgical intervention for reduction and fixation.3–7
However, there are relatively few studies that examine the epidemiology and outcomes of pediatric hand fractures. We performed a retrospective review of all pediatric hand fractures referred to the plastic surgery hand clinic over a 3-year period. The purpose of this study is to evaluate the epidemiology, management, and outcomes of pediatric hand fractures, where care was imparted and by whom, and offer resource utilization suggestions.
Methods
The records of all children under 18 years of age who presented to the British Columbia Children’s Hospital (BCCH) Emergency Department between November 1, 2016, and January 31, 2020, with metacarpal or phalangeal fractures and were referred to the pediatric plastic surgery hand clinic were reviewed retrospectively. Soft tissue injuries without a concomitant fracture, isolated carpal fractures, isolated joint dislocations, and patients with incomplete records were excluded. All fractures were analyzed as individual entries. Patient demographics, mechanism of injury, radiograph results, fracture classification, and specifics of treatment for each fracture were collected and their outcomes reviewed. The radiographs were reviewed with the staff surgeon when the fracture diagnosis was unclear. “Surgical” fractures were defined as injuries requiring management in an operating room setting, whereas “Nonsurgical” fractures were defined as those managed in an office or emergency department setting alone.
Descriptive statistics were used to describe our cohort with a focus on the differences between fractures requiring surgical management and those not requiring surgical management. Odds ratio and 95% confidence intervals were calculated for clinically relevant outcome predictors (ie, angulation >10°, displacement >2 mm, etc). The University of British Columbia Children’s & Women’s Research Ethics Board granted permission to conduct this study, H20-00563.
Results
A total of 559 patients were referred to the British Columbia Children’s Hospital pediatric plastic surgery hand clinic between November 2016 and January 2020. Of these, 35 had isolated soft tissue injuries, 3 had joint dislocations without fractures, and 22 were missing prereduction radiographs and were thus excluded. Therefore, 524 hand fractures in 499 patients were analyzed.
The anatomic location of hand fractures is shown in Figure 1. Commonly fractured sites were the base of the fifth proximal phalanx (11.3%), the base of the first proximal phalanx (11.1%), and the head of the fifth proximal phalanx (6.9%). Overall, the most commonly fractured finger was the fifth finger (36.8%), and the most commonly fractured bone was the proximal phalanx (46.2%).
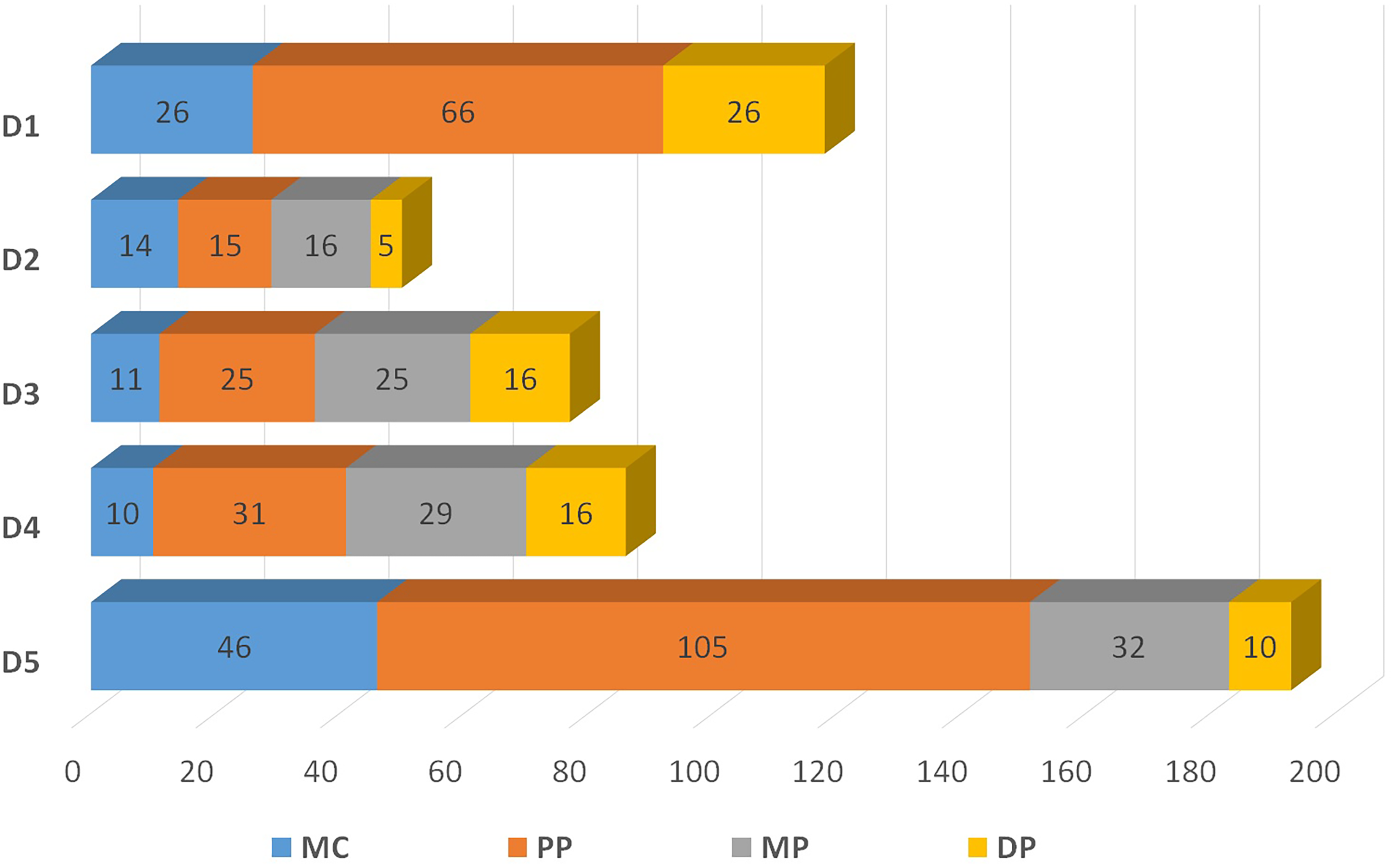
Distribution of fractures by bone. The number on each bone reflects a total number of fractures occurring in each bone.
Twice as many boys experienced hand fractures as girls. Figure 2 represents their age at the time of fracture by sex. The median age of hand fractures in the entire cohort was 11 years (mean = 11.1). The median age of hand fractures for boys was 12 years, while the median age of hand fractures for girls was 11 years. Common mechanisms of pediatric hand fractures were ball-related sports injury (44.6%) and fall-related injury (25.6%). Males were twice as likely to be involved in the sport-related and ball-related injuries, whereas crush injuries were similar between the 2 sexes.
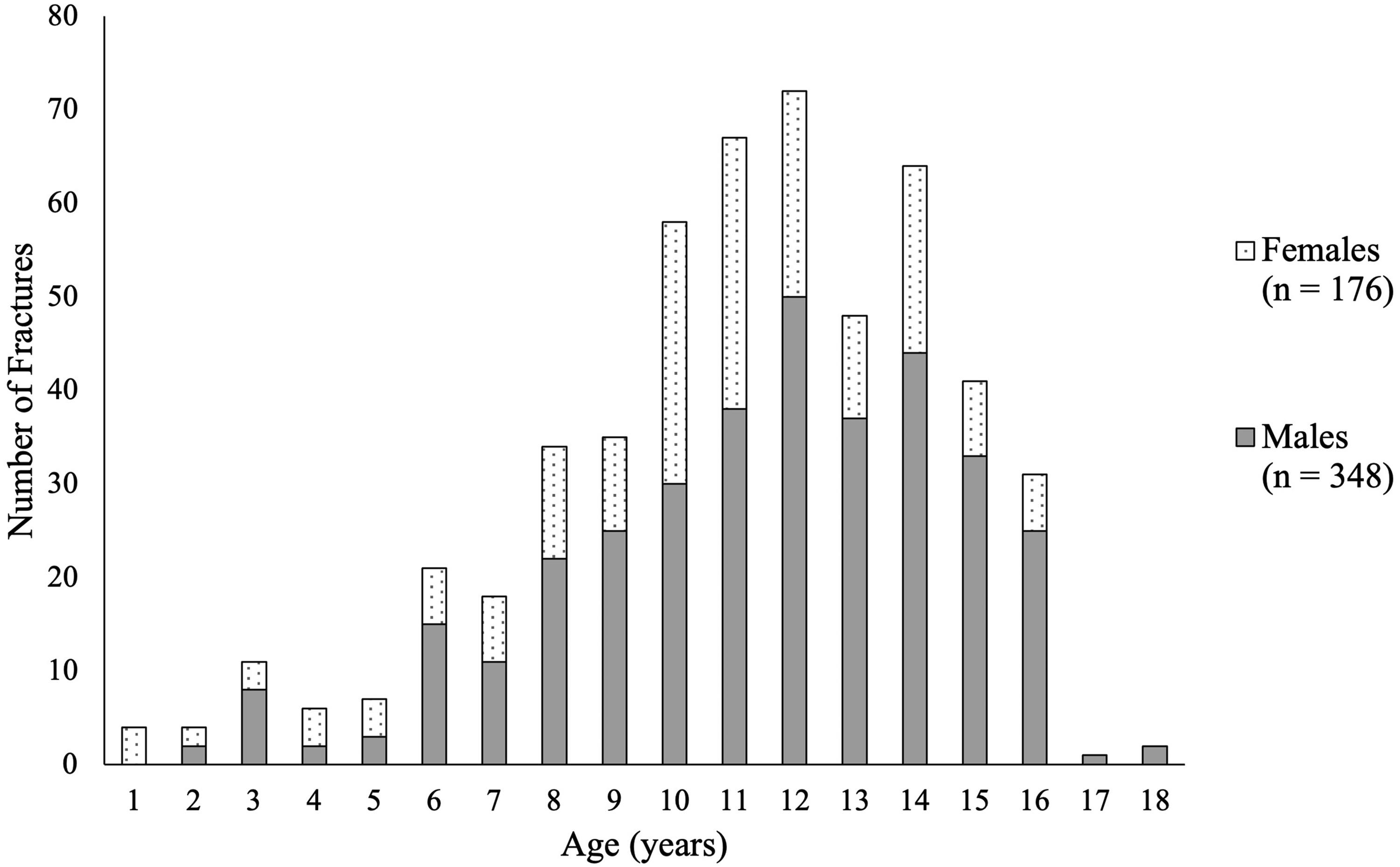
Proportion of hand fractures by age and sex [might this look better as a stacked bar graph?].
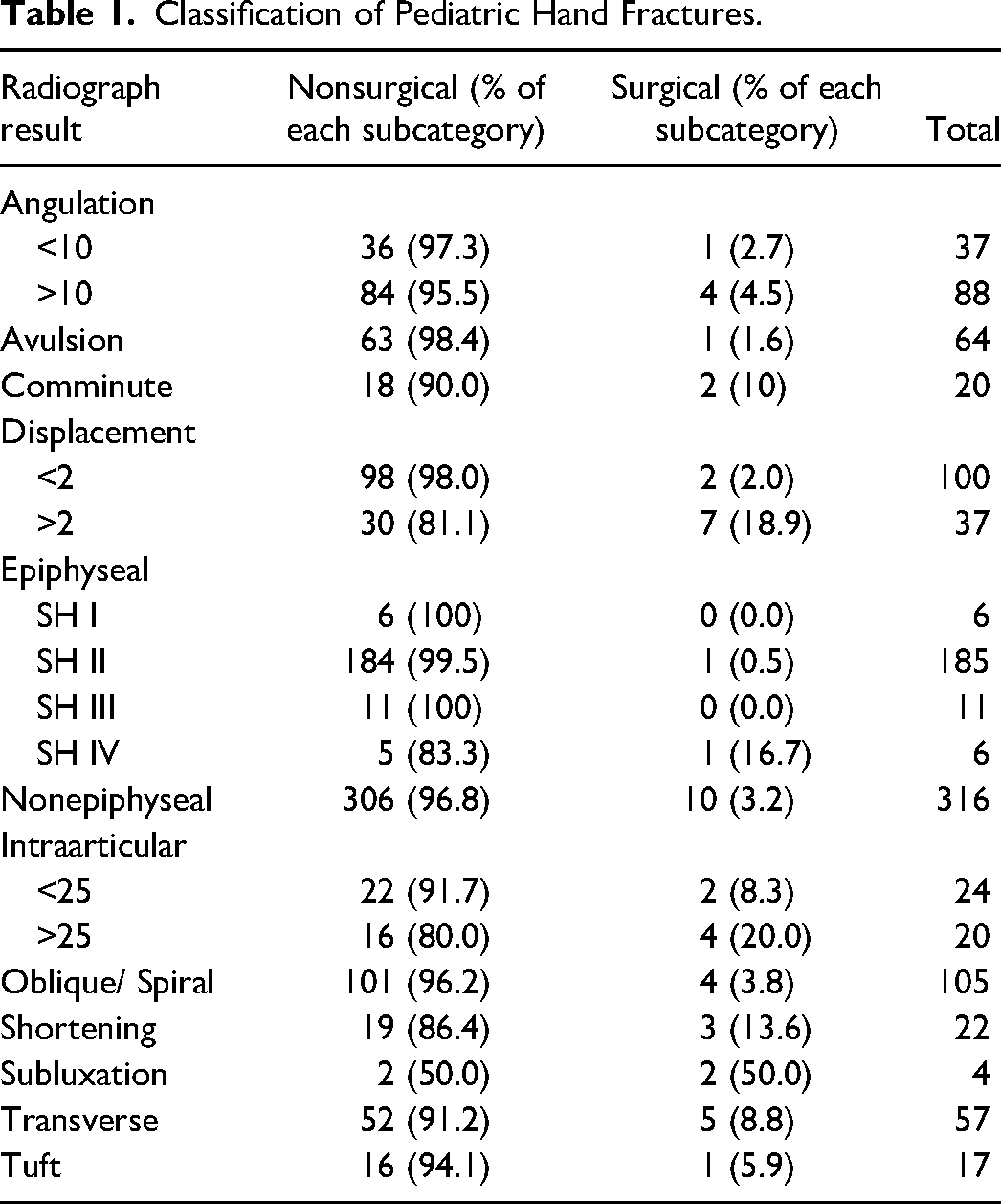
Clinical characteristics of fractures are shown in Table 1. There were 316 (60.3%) nonepiphyseal fractures and 208 (39.7%) epiphyseal fractures. Of the 208 epiphyseal fractures, the majority of fractures (88.9%) were Salter-Harris Type II. A total of 57 of all fractures were transverse (10.9%), 105 (20%) were either oblique or spiral fractures, and 17 (3.2%) were tuft fractures. Most of the fractures were extra-articular (90%), without angulation (76%), and without displacement (74%).
Classification of Pediatric Hand Fractures.
The most common fracture management was immobilization alone without reduction (75% of all fractures). A total of 23% of fractures required closed reduction outside of the operating room, either with local anesthetic or conscious sedation. Of the fractures that received a closed reduction, the ER physician attempted the reduction first in 73% of cases and were successful (defined by an absence of a repeat reduction or further intervention) 82% of the time. Only 12 fractures (2.3%) required surgery. Of the surgical cases, 10 were closed reduction with k-wire fixation, one was an open reduction with k-wire fixation and one was a closed reduction with no fixation (1.9%, 0.2%, and 0.2% of all fractures, respectively). Fractures that required surgery were more likely to have greater than 10° of angulation (OR 7.3 [95% CI 2.1-24.7]), greater than 2 mm of displacement (OR 14.8 [95% CI 4.3-50.6]), intra-articular (OR 12.5 [95% CI 3.8-40.5]), or transverse (OR 6.3 [95% CI 1.9-20.6]) in nature when compared to nonsurgical fractures (Figure 3).
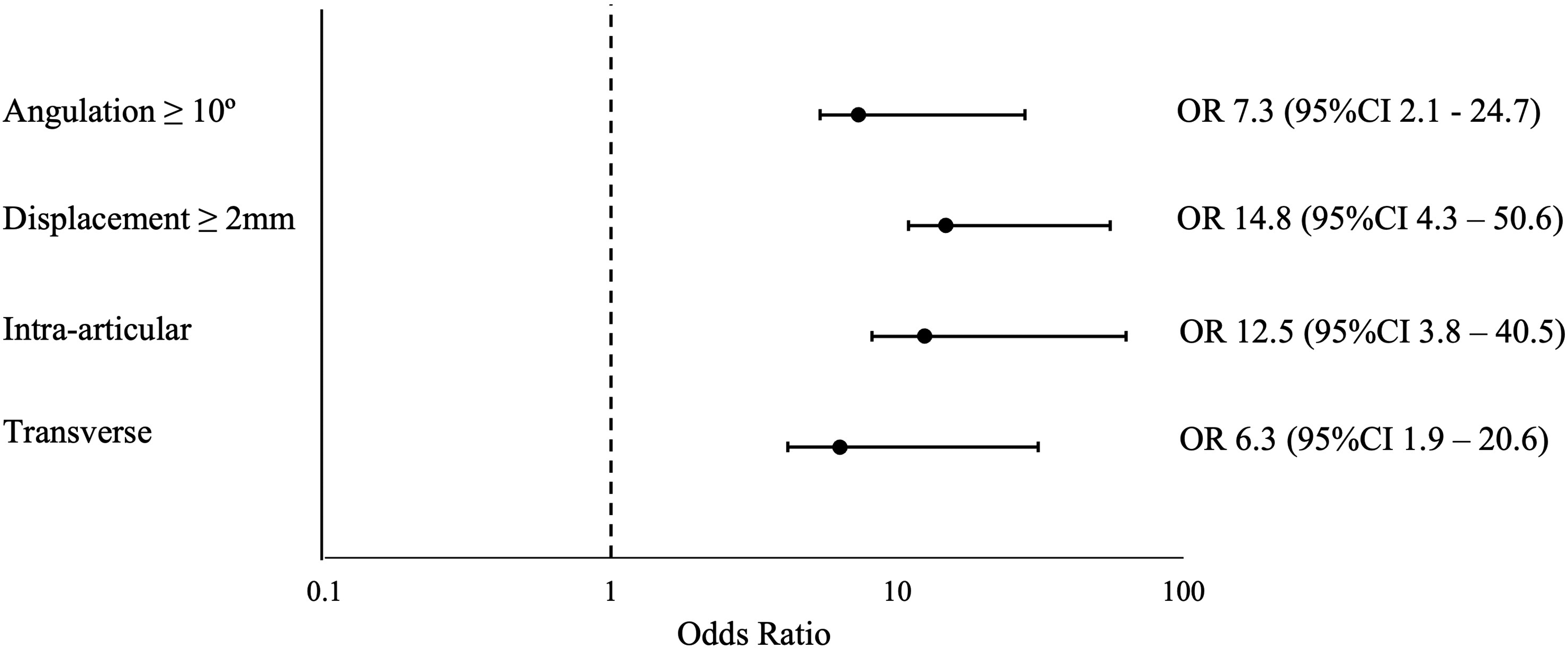
Odds ratios for clinically relevant characteristics of fractures requiring surgery.
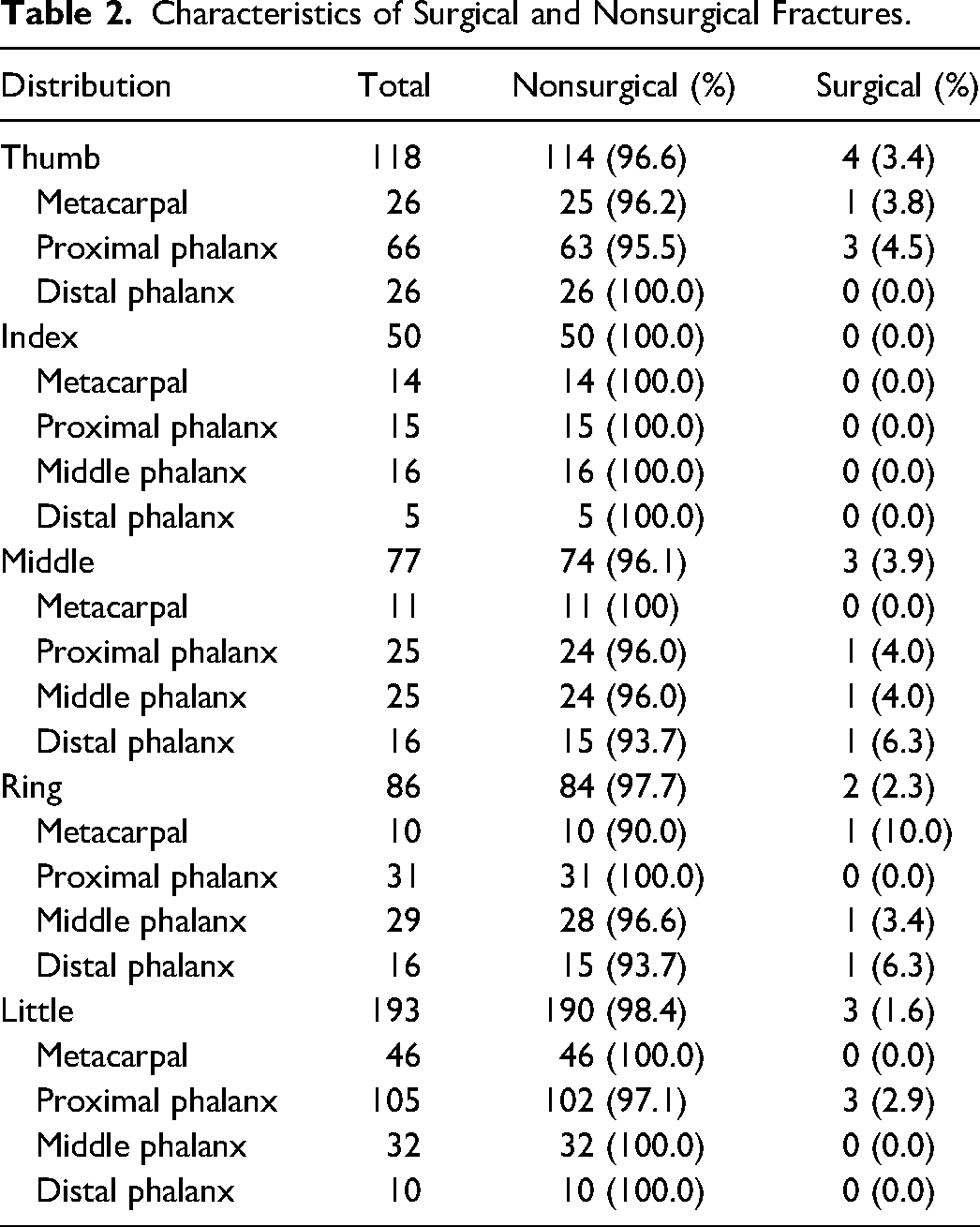
Children age 8 years and older made up 77% of surgical candidates and required a median number of 3.5 clinical visits (range 2-5). Nonsurgical candidates had a median of 2.0 clinic visits (range 1-5). Of the 12 surgical cases, there was a 0% reoperation rate, no documented infection, and 1 (0.2%) unsatisfactory surgical reduction that did not require further intervention given no functional deficit. Table 2 describes the characteristics of surgical and nonsurgical fractures.
Characteristics of Surgical and Nonsurgical Fractures.
Discussion
Epidemiology
This retrospective study identifies the etiology, characterization, and management of 524 pediatric hand fractures referred to the British Columbia Children’s Hospital plastic surgery hand clinic. Fractures of the pediatric population appear to be twice as common in boys than girls. The most common mechanisms of injury include sport-related injuries, followed by falls and crush injuries. Nonepiphyseal fractures made up more than half the fracture type, but Salter-Harris Type II was the most common fracture classification. The most commonly fractured bone was the fifth digit proximal phalanx. Our data on the etiology and characteristics of pediatric hand fractures presented is consistent with previously published literature.4–6 Small variations in findings may be attributable to differences in geographical location thus differences in hobbies between our study cohort and the population of previously published data.
Surgical Rates
Most fractures were managed non-operatively with approximately one-quarter of the fractures requiring closed reduction. Of those patients that received closed reduction, 11 fractures required 4 or more appointments. Even though these fractures did not go on to receive surgery, the surgeons felt close monitoring was warranted. At our institution, surgeons will perform serial assessments and radiographs for spiral metacarpal fractures, condylar head fractures, and middle phalanx fractures as they feel these fractures are at risk for loss of reduction. In a scoping review of 20 studies on pediatric hand fractures by Hartley et al, 7 surgical rates ranged from 0% to 32.9%. Our site-specific surgical rate of 2.3% is lower than most of the other studies. Our finding was most similar to that of Davis and Stothard, 8 a review of over 600 fractures with a documented referral rate of 100% and reported a surgical rate of 2.9%. Clearly, when more stringent criteria for referral were applied, such as open fractures, those with displacement and malrotation, the reported surgical rates were significantly higher, from 12% to 32.9%.4,9
Other studies with higher surgical rates did not always report whether there were center-specific referral criteria.7,10,11 At our center, we currently do not have any exclusion criteria for referral of hand fracture patients to plastic surgery from the emergency department or primary care physician. Furthermore, the definition of surgical management could be different between studies. We did not count closed reduction as an operative case; only patients that went to the operating room were defined as operative cases in our series. Other authors may have slightly different definitions for an operative case. It is unclear whether a closed reduction that took place in the OR but without general anesthesia (GA) counted towards “surgical management” as most studies did not specify this detail. At our institution, almost all closed reductions take place outside the OR, either at the bedside or in the clinic setting contributing to our low surgical rate. Moreover, we have the luxury of conscious sedation in the emergency department which facilitates the timely disposition of these patients and avoids delays to access in the operating room, whereas this may not be the case at other centers.
Resource Utilization
In our study population, 75% of patients had uncomplicated fractures which required immobilization alone. At our center, these generally simple and stable fracture referrals consistently are referred for outpatient follow-up to the plastic surgery hand clinic. Given our analysis, rarely do these fractures result in the need for any active intervention by the plastic surgeon while in clinic, other than simple patient education and maintenance of immobilization. Rarely do these patients require referral to a hand therapist. This would suggest that not all hand fractures seen in the ED require the involvement of a plastic surgeon and it would be safe to outsource this visit. In the orthopedic literature, Stepanyan et al 12 examined outcomes of pediatric clavicle fractures and showed that closed, minimally displaced fractures with or without angulation can be well managed in the primary care setting without the involvement of the orthopedic specialist. Doing so improves healthcare value by decreasing the opportunity cost of the clinic visit at no detriment to the patient.13,14 Furthermore, a recent study by Fuschini et al 15 evaluated the management of simple orthopedic fractures in the primary care setting without visits to an orthopedic clinic. These injuries included volar plate avulsions, proximal phalanx, and metacarpal fractures. The study demonstrated that utilizing a primary care pathway for a referral from the ED for low-risk orthopedic injuries was a safe, cost-effective alternative. Future research should determine criteria for referral such that these uncomplicated patients may be followed in a primary care or sports medicine clinic which may be more convenient for the family without added risk. Furthermore, healthcare value will be enhanced as the opportunity cost always falls toward urgent/emergent referrals13,14; by decreasing demand for outpatient clinic access in our high resource utilization Canadian healthcare system, another long waiting elective patient can be prioritized for access.
Limitations
Limitations of this study include its retrospective study design. Furthermore, while fracture management and outcome of surgical fractures were reported, long-term outcomes of nonsurgical fractures were not always available, presumably given their favorable outcomes.
Conclusions
Nonsurgical treatment of pediatric hand fractures offers very encouraging outcomes. Our results suggest that patients generally do well and management of these fractures is usually possible in the ED or clinic setting and rarely require the consumption of operating room resources. Furthermore, the vast majority of patients can very likely be safely and effectively followed outside of the plastic surgery hand clinic and future research should focus on indications for which patients require a plastic surgeon’s active management.
Footnotes
Acknowledgments
We would like to acknowledge Dr. Marija Bucevska, Clinical Research Coordinator at UBC/BC Children's Hospital for the administrative support provided for this projects and help with Figure 1.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Department of Surgery, University of Calgary Cumming School of Medicine (grant number The Sharpest Knife Grant). Additionally, Sabrina Wei received a summer studentship grant from the Summer Student Research Program, University of British Columbia.