
Abstract
Background:
A Streamlined Care In Pediatric Hand Injuries (SCI-PHI) pathway was developed to reduce unnecessary follow-ups and improve health care resource utilization. This study aimed to investigate the post-implementation outcomes of patients treated with this previously developed SCI-PHI pathway.
Methods:
Participants were contacted 12 months post-injury to complete a questionnaire, including a modified version of the Michigan Hand Questionnaire and the Patient-Reported Outcomes Measurement Information System upper extremity score.
Results:
Ninety-four percent of patients had a pain-free return to activity, and 93% were satisfied with the appearance and function of their injured hand. Five patients (4%) had questions that were answered over the phone, and 5 patients (4%) requested follow-up with the surgical team. No patients required any intervention beyond reassurance. There was a consequent 27% reduction in visits.
Conclusions:
The SCI-PHI pathway for children with simple hand injuries demonstrates good patient-reported outcomes and satisfaction. This has the potential to save significant resources for both families and the health care system.
Introduction
Hand fractures are the second most common fractures in children. 1 While a small portion of these fractures require operative management, more than 80% heal well with immobilization with or without closed reduction. 2 Despite these “simple fractures” healing well without the need for surgical intervention, many are over-treated with unnecessary follow-ups and radiographs, resulting in the inefficient utilization of health care resources.
The Streamlined Care In Pediatric Hand Injuries (SCI-PHI) pathway was previously developed and implemented at our institution in 2021 to improve resource utilization. 3 Eligible children with simple hand injuries were treated with either buddy taping or immobilization, standardized care instructions (Supplemental Appendix A), and no scheduled follow-up. In this initial study, most patients with simple hand fractures healed effectively without requiring follow-up visits, suggesting that verbal and written care instructions were adequate, and a significant reduction in health care resources could be realized. 3 The primary objective of this study was to evaluate post-implementation outcomes of the SCI-PHI pathway, which has been in routine use in our clinic for more than 2 years.
Methods
Following Research Ethics Board approval, a retrospective review of children (<18 years of age) who presented with hand injuries to an outpatient Plastic Surgery clinic at a tertiary pediatric center was completed. Patients were identified from a prospectively maintained database. All children treated from July to December 2022 with the previously developed SCI-PHI pathway were included. 3 Patients were prospectively included in the SCI-PHI pathway at the discretion of the attending fellowship-trained Pediatric Plastic Surgeon if their injury was thought to be a “simple” hand injury that could be treated conservatively and without the need for scheduled follow-up. Simple hand injuries were defined previously to include various fractures such as undisplaced or buckle fractures and Salter-Harris type 2 (SH2) fractures of the proximal or middle phalanx, with the full list available in Supplemental Appendix B. Unlike the previous prospective validation study, however, patients were not formally screened to ensure that they met the previous inclusion criteria. All other management was performed following the SCI-PHI pathway: patients received splint or taping treatment, standardized instructions, and no scheduled follow-up.
Patients treated with the SCI-PHI pathway were contacted by telephone 12 months post-injury to complete, individually or by parent proxy, a 1-time telephone questionnaire. Patients were excluded if they could not complete the telephone questionnaires in English or French. When unavailable, patients were contacted up to 4 times to complete the questionnaire. For non-responders, a retrospective chart review was performed to identify any additional clinic or emergency department visits for the same injury.
Those who indicated concerns or requested a follow-up were scheduled for reassessment in the plastic surgery clinic. Two patient-reported outcome measures were used to evaluate the outcomes: the brief Michigan Hand Questionnaire (MHQ) and the Patient-Reported Outcomes Measurement Information System (PROMIS) score. The MHQ is a well-established tool used to evaluate subjective domains of hand function in patients with hand disorders. 4 The PROMIS upper extremity score is a questionnaire evaluating the physical function of a patient’s upper extremity. 5 It has been validated in the pediatric population and via telephone and parent proxies.6-8
The primary outcome of this study was patient or parent-proxy-reported PROMIS and satisfaction scores. Secondary outcomes included patient-reported splinting duration, results of the brief MHQ, deviation from the care pathway, such as the need for additional follow-up visits or a change in the treatment plan, and the number of visits saved. Visits saved were calculated based on the assumption that all patients with a hand injury would require at least 2 visits (initial consultation and 1 follow-up to ensure adequate healing). As such, the percentage of visits saved would be calculated by dividing the number of visits with the SCI-PHI pathway compared with the number of visits expected (at least 2 visits) without using the pathway.
Results
During the study period, 449 patients with hand injuries were referred to the plastic surgery clinic. Two hundred and forty-eight of these children (55%) were determined to have “simple” hand injuries and were thus treated with the SCI-PHI pathway and included in the study. Of the 248 participants, 125 (50%) responded to the telephone follow-up survey. No participants were excluded (Figure 1). Five (4%) of those interviews were completed by patients, while the other 120 (96%) interviews were completed by parent proxies. The mean follow-up period was 12.8 months (SD = 1.2). Of the responders, 68% of patients were male, with a mean age of 11.8 (SD = 1.2). Most patients had open growth plates (74%) and did not require closed reduction (86%) at the time of consultation. There were no significant differences between the study population, telephone non-responders, and the previous study population when comparing sex, laterality of hand injury, physeal status, or recommended treatment demographics (Tables 1 and 2). Overall, the most common fractures were Salter-Harris 2 proximal phalanx (21%), metacarpal neck (18%), proximal interphalangeal (PIP) volar plate avulsion (11%), and distal phalanx (11%) fractures (Table 1).
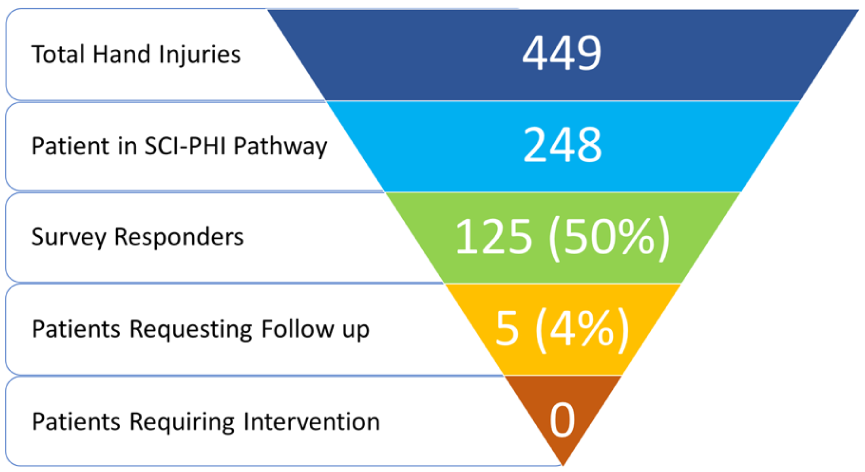
Study population.
Study Population Demographics.
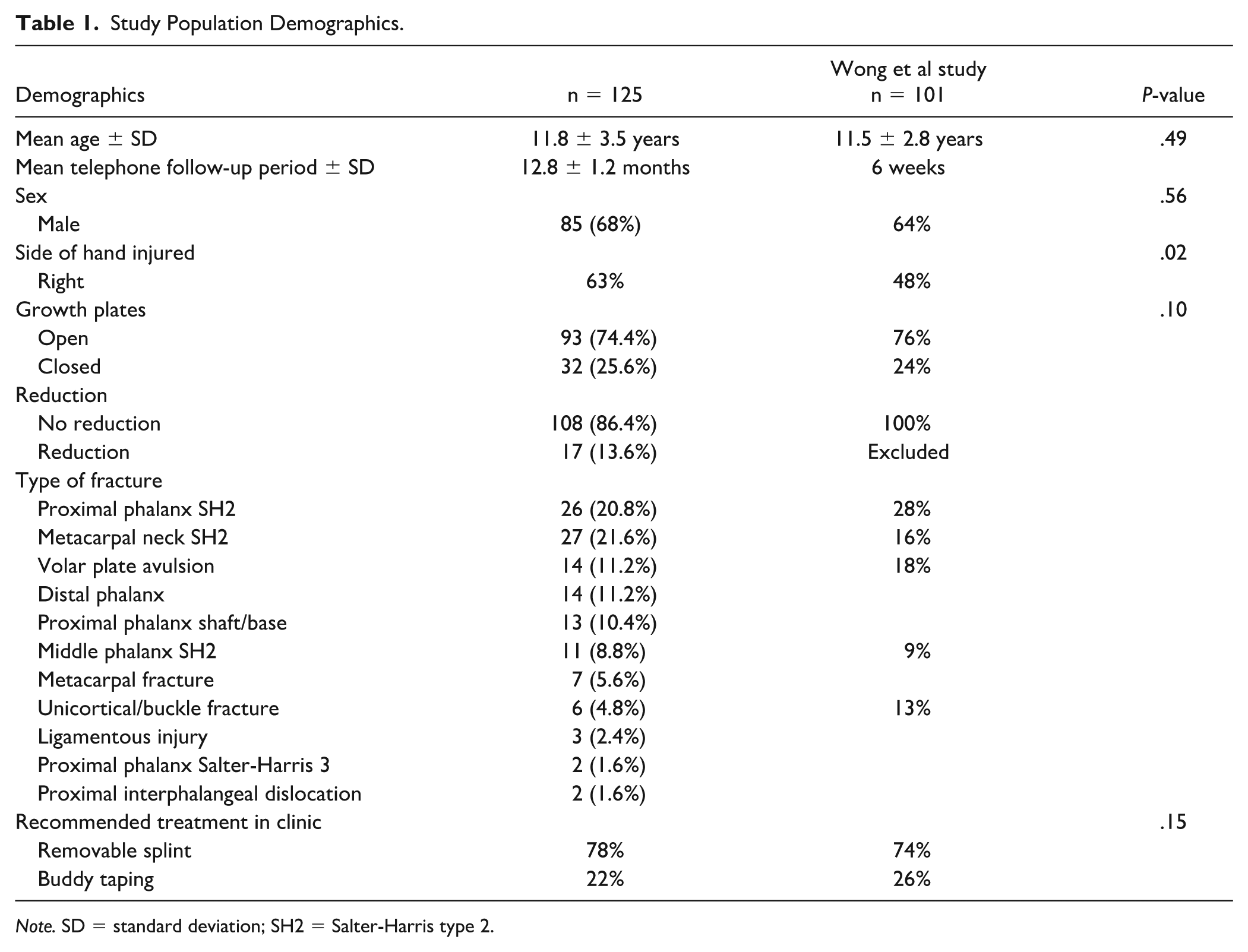
Note. SD = standard deviation; SH2 = Salter-Harris type 2.
Study Population Demographics for Non-Responders.
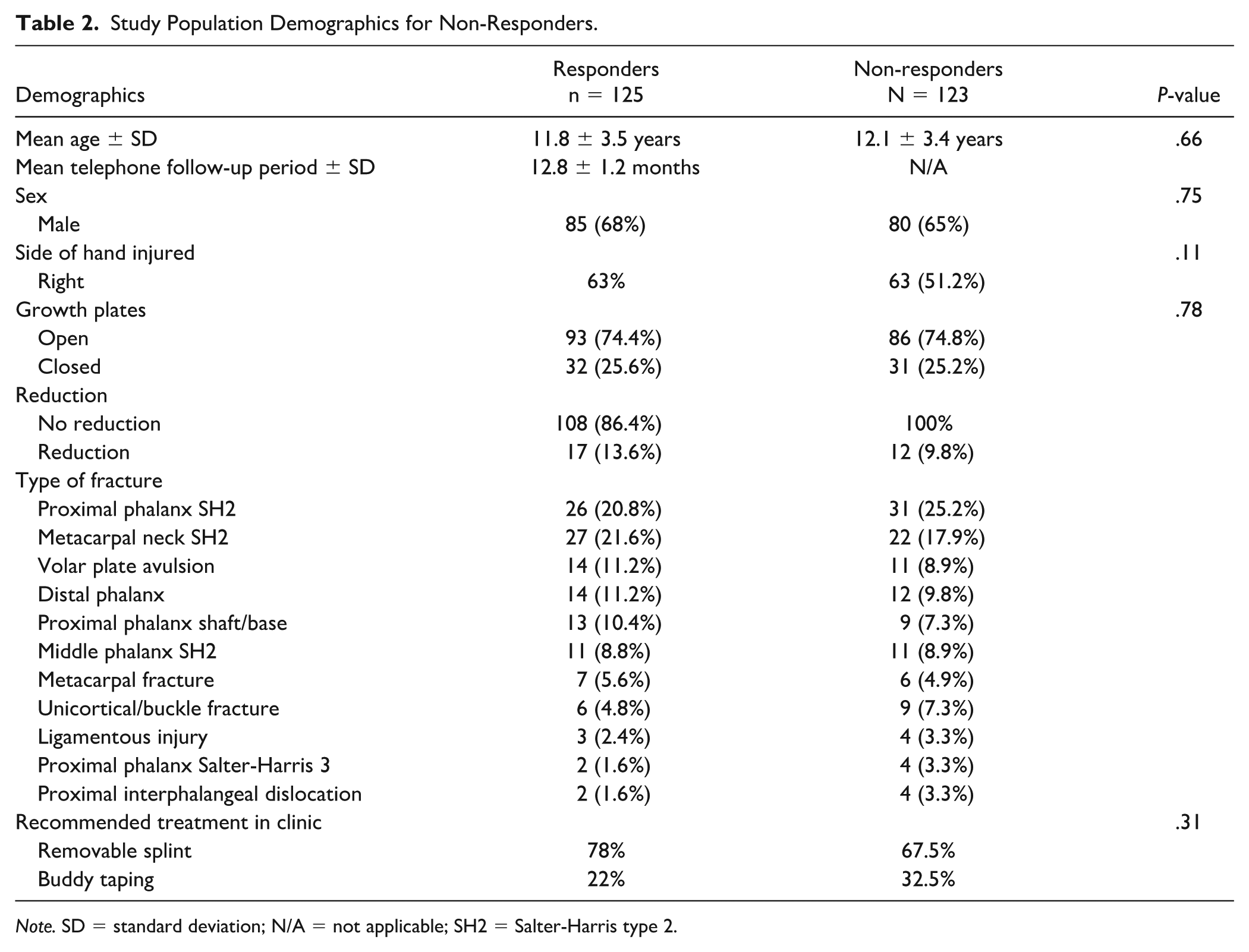
Note. SD = standard deviation; N/A = not applicable; SH2 = Salter-Harris type 2.
From the telephone questionnaire, 117 (94%) patients reported a pain-free return to activities at the time of their interview and 116 (93%) were very satisfied with the appearance and function of their injured hand. The mean splinting or buddy taping time among patients was 4.3 weeks (SD = 1.5) (Figure 2), and the mean return to full activity was 6.5 weeks (SD = 2.4) (Figure 2). In total, 5 patients (4%) requested follow-up with their surgeon, all of whom received reassurance and no further intervention. An additional 5 patients (4%) had general questions that were addressed over the phone and were not considered as follow-up. As a result, of the 449 pediatric hand fractures treated during the study period, 243 required 1 initial assessment with no follow-up, resulting in 243 saved visits, representing a 27% reduction compared with the 898 visits typically required under the standard minimum 2-visit protocol.
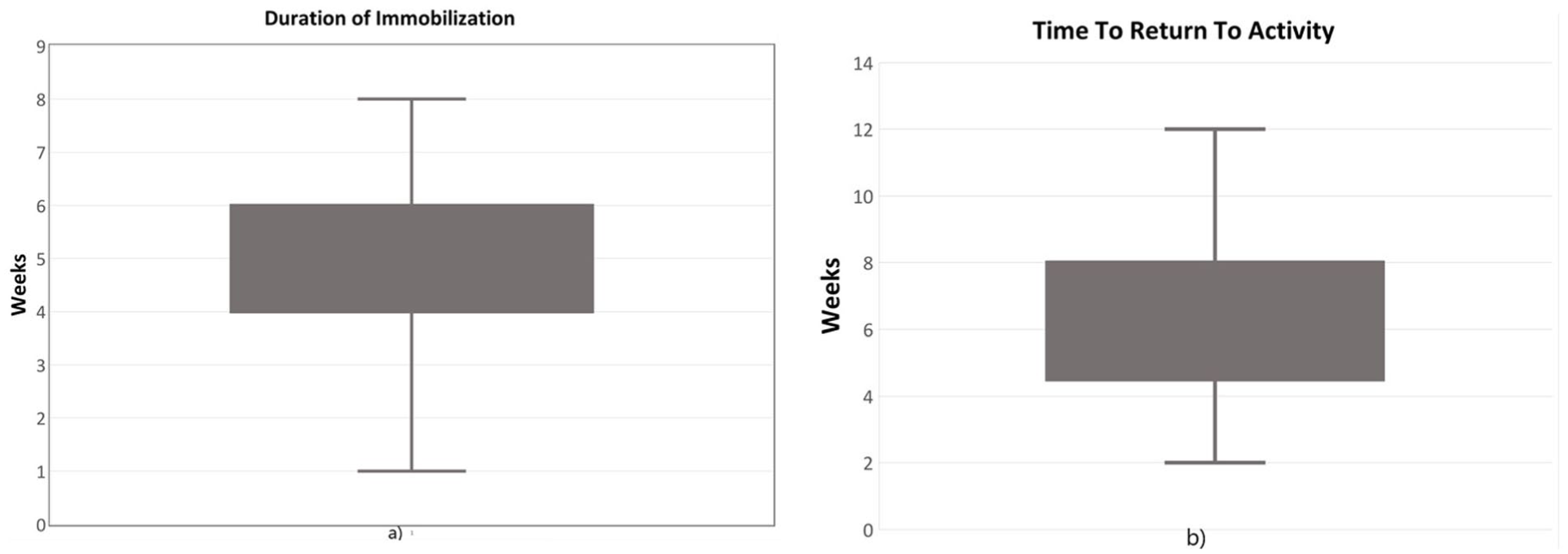
Outcomes of treatment (a) Duration of immobilization. (b) Time to return to activity.
Patient-Reported Outcomes Measurement Information System upper extremity scores were graded out of 32 points and converted into a T-score. 5 Most respondents (n = 120, 96%) reported a perfect score of 32/32. 9 The 5 patients with imperfect scores consisted of 3 volar plate avulsions (T-scores = 40, 45, and 45), a metacarpal neck fracture (T-score = 35), and a distal phalanx fracture (T-score = 35). The mean brief MHQ score was 97.9 (SD = 5.2). In addition, patient satisfaction was assessed, with 5 (4%) reporting dissatisfaction. PIP-related injuries, specifically volar plate avulsion fractures, accounted for 2 of the 5 less satisfied patients. No patient required further intervention aside from reassurance, and following chart reviews, survey non-responders had no evidence of unscheduled follow-ups.
Discussion
Pediatric hand fractures are a common presentation in plastic surgery clinics. Most of these fractures are treated with immobilization with or without closed reduction and do not require surgical intervention. 2 A previous study by Wong et al 3 showed promising results when a streamlined care pathway for simple pediatric hand injuries with no routine follow-up was prospectively evaluated. The current study confirmed that, even with longer follow-ups, patients continued to function well and were satisfied with their outcomes. Significant reductions in patient visits were again realized. Moreover, this post-implementation study demonstrated the application of the pathway to a wider variety of hand fractures.
Overall, patients progressed well with only 4% requesting follow-up, an improvement from the 16% requesting follow-up in the previous study. Patients who did report decreased satisfaction had concerns with the aesthetic appearance of their hand or finger rather than functional limitations.
Patients treated with the SCI-PHI pathway had similar demographics compared with those in the initial study and other studies of children with hand injuries referred to plastic surgeons.2,3,10,11 In PIP-related injuries, there were high levels of satisfaction and few follow-up requests. However, as in previous studies, there was an overrepresentation of PIP-related injuries among unsatisfied patients. 12 They also represented 2 of the 5 patients requesting follow-up. While no change in management was indicated, surgeons should provide additional counseling and ensure clear expectations when including them in the SCI-PHI pathway, due to concerns for dissatisfaction. Further investigation into the underlying causes of dissatisfaction and follow-up requests among PIP patients would be beneficial in future studies.
Implementing the streamlined approach to simple pediatric hand fractures provides benefits to both the patient and the health care system. It allows for better resource allocation in the hospital by reducing unnecessary follow-ups for patients who do not require further intervention. This study saved 243 visits, reducing patients requiring follow-up by 27%. Patients, furthermore, benefit from fewer unnecessary appointments and the associated cost and travel time. 11 This is not a unique concept. Hartley et al 13 developed the Calgary Kids’ Hand Rule for Emergency Physicians to identify simple versus complex pediatric hand fractures. Those identified as simple could be safely managed without referral to a plastic surgeon. In a single-payer system such as Canada, adoption of any strategy to safely decrease health care utilization should meet little resistance due to the additional benefits of decreasing wait times for other patients. There is precedence for similar strategies to reduce dependency on the health care system for children with distal radius buckle fractures.14,15 Implementation of any new management strategy in clinical care may require assessment of barriers to knowledge use and adaption to the local context. Knowledge translation strategies are well described by MacDermid and Graham. 16
The limitations of this study include the small sample size, limited response rate, and the risk of single-institution bias. Despite the 50% response rate, non-responders did not appear to have any issues necessitating additional visits to the Emergency Department or Plastic Surgery clinic, as evidenced by chart review. In addition, the risk for response bias is mitigated as non-respondents did not have any differences in study demographics (Table 2). Patients who may have had concerns would most likely call the clinic since the institution is the only pediatric center in a large region. In addition, while the inclusion of patients in the SCI-PHI pathway was at the discretion of the treating surgeon, the patients included in the pathway have expanded since the initial study. At a minimum, consequently, this study supports increased confidence in the use of the SCI-PHI pathway for the injury types described in the original study (Supplemental Appendix B).
Conclusions
This study confirms the safe and effective utility of a streamlined care pathway for simple pediatric hand injuries, obviating the need for routine follow-up. Patients reported satisfactory long-term function and outcomes. This pathway will help improve resource utilization in the hospital and relieve the health care burden on patients.
Supplemental Material
sj-docx-2-han-10.1177_15589447261415640 – Supplemental material for Post-Implementation Outcomes of a Streamlined Care in Pediatric Hand Injuries Pathway
Supplemental material, sj-docx-2-han-10.1177_15589447261415640 for Post-Implementation Outcomes of a Streamlined Care in Pediatric Hand Injuries Pathway by Koorosh Kashanian, Yonatan Fortinsky, Sivim Sohail, Claudia Malic, Yvonne Ying and Kevin Cheung in HAND
Supplemental Material
sj-pdf-1-han-10.1177_15589447261415640 – Supplemental material for Post-Implementation Outcomes of a Streamlined Care in Pediatric Hand Injuries Pathway
Supplemental material, sj-pdf-1-han-10.1177_15589447261415640 for Post-Implementation Outcomes of a Streamlined Care in Pediatric Hand Injuries Pathway by Koorosh Kashanian, Yonatan Fortinsky, Sivim Sohail, Claudia Malic, Yvonne Ying and Kevin Cheung in HAND
Footnotes
Acknowledgements
None.
Contributorship
KC and KK researched literature and conceived the study. All authors were involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. YF wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Ethical Approval
Ethical approval was not sought for this article because this project was a quality improvement initiative determined by Research Ethics Board to not require approval. This study was completed by the Helsinki Declaration as revised in 2013.
Statement of Human and Animal Rights
Ethical approval was not sought for this article because this project was a quality improvement initiative determined by the Research Ethics Board not to require approval. There were no concerns for human or animal rights.
Statement of Informed Consent
Verbal informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The dataset supporting this study’s findings is available from the corresponding author upon reasonable request.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.