
Abstract
Introduction
Open tibial fractures refer to tibia fractures associated with soft-tissue injuries. These fractures can be difficult to manage, often requiring a collaborative effort between orthopedic surgery and plastic surgery teams for early irrigation, debridement, bony stabilization, and soft-tissue reconstruction. Soft-tissue reconstruction can range from local and regional flaps to more complicated free flaps, and is essential for restoring vascularity, stability, and providing coverage for vital structures such as bone, nerves, and vessels. These surgeries are typically done by plastic and reconstructive surgeons and completed after bony fixation by orthopedic surgeons. Due to the closely integrated and collaborative relationship between the two specialties, many institutions in the United Kingdom and other parts of the world have adopted “orthoplastic” teams to help manage these injuries in more efficient and streamlined manner.1-3
Despite multidisciplinary efforts, open tibial injuries confer high complication rates including infections, bony malunion or nonunion, compartment syndrome, need for revision surgery and amputation. The complexity of management and the high rates of complications have prompted vast research into coordination and centralization of care to examine and improve outcomes in open tibial fractures. Early surgical debridement, direct admission to a trauma centre with appropriate specialists available, and early soft-tissue reconstruction have been shown to reduce complication rates, number of surgeries, and length of hospital stay.4-7
A number of population-level studies have examined open tibial fracture management in the United States and Europe,8-13 but similar studies have not been performed in Canada. The characteristics of the patient population and typical management patterns in Ontario remain largely unknown. The goal of this work is to describe the characteristics of individuals with open tibial injuries in Ontario, analysing their admission locations, management patterns, complication rates, and investigating areas where care could be improved.
Methods
To conduct this study, data from ICES, previously known as the Institute for Clinical Evaluative Sciences, was used. ICES is a nonprofit research institute that holds administrative population-based linked databases, retaining a variety of health-related data for every single individual in Ontario. These datasets were linked using unique encoded identifiers and analysed at ICES. These include demographic information, different hospital encounters, diagnoses, and interventions the individual had received. For our study, those who sustained an open tibial fracture between April 1, 2009 to March 31, 2020 were identified using ICD-10 diagnostic codes (S82101, S82201, S82301). Patients were excluded if the data was incomplete, they were not Ontario resident, were aged less than 18 or greater than 105, or had previous tibia injury. Patients who did not have a record of visit to the emergency department, or a record in the Ontario Trauma Registry, as well as the record of admission to the hospital were excluded. Other than records from individual hospital emergency department, Ontario Trauma Registry collaterally records administrative data related to major traumas in Ontario and was cross-reviewed to ensure no pertinent information was missed.
Basic demographic information, relevant past medical history, and details about the injury were examined. Year of injury, mechanism of injury, presence/type of neurovascular injury, and whether the Injury Severity Score (ISS) was greater than 15 were collected. To investigate what type of hospitals they were being admitted to, we examined those admitted to trauma centre, and nontrauma centres. Nine adult trauma centres in Ontario (Winsor Regional Hospital, London Health Sciences Center, Hamilton Health Sciences, St. Michael's Hospital, Sunnybrook Health Sciences Center, Kingston General Hospital, The Ottawa Hospital, Health Sciences North, and Thunder Bay Regional Health Sciences Center) were included in the analysis. 14 One of the major outcomes that was examined was whether one had a soft-tissue reconstruction in the hospital, and if it occurred in the timeframe of 72 h. In addition, the incidence of amputation, malunion or nonunion, debridement for infection, compartment syndrome, external fixator placement, death, consultation with plastic surgery service, and length of stay in the hospital were examined.
Baseline variables were compared between those admitted to a trauma centre and a nontrauma centre using one-way analysis of variance, Kruskal–Wallis, chi-square, and the Cochran-Armitage trend test. For outcomes, Mann-Whitney U analysis was completed for continuous variables, and the odds ratio (OR) was calculated for the categorical variables. Standardized differences were also reported as a subtle measure of differences in the results where the sample size was large. 15 Regression models were further used to analyse the outcome of the two groups, those admitted to a trauma centre and a nontrauma centre. Covariates such as direct admission to a trauma centre, patient age, sex, Charlson Comorbidity Index (CCI), rurality, ISS > 15, neurovascular injury, and mechanism of injury were included.
Results
A total of 4240 patients who had open tibial fractures and met the inclusion and exclusion criteria were identified. When stratified by admission location, 1722 patients were admitted to a trauma centre, and 2471 patients were admitted to a nontrauma centre. The baseline characteristics of the cohort population are described in Table 1. The mean age of the cohort population was 47, and more than two-thirds of the patients were males. Motor-vehicle collisions (MVC) were the most common cause of the injury, accounting for almost half of the identified patients, followed by falls.
Baseline Variables of the Cohort Population.
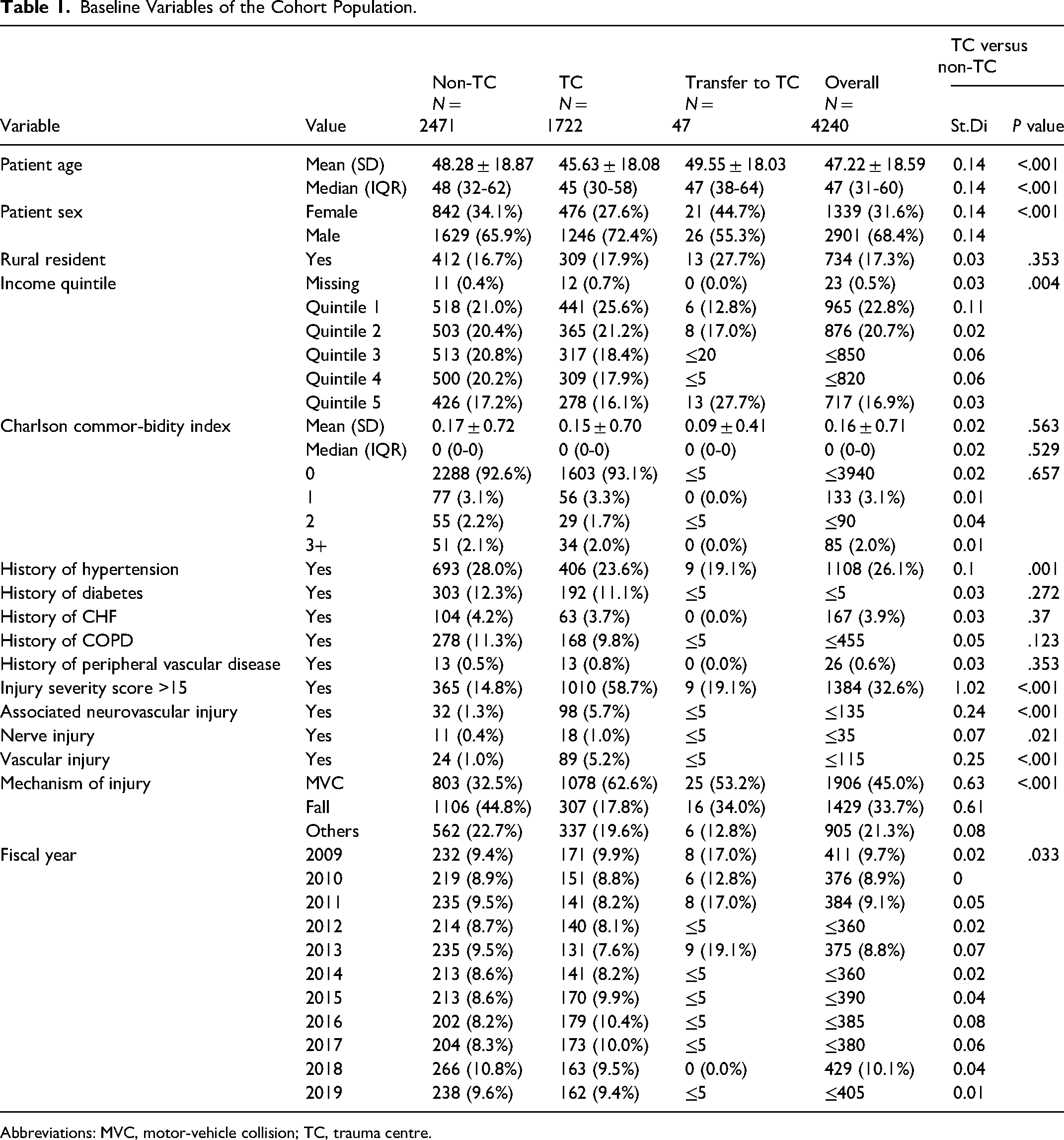
Abbreviations: MVC, motor-vehicle collision; TC, trauma centre.
When the characteristics were compared between those who were admitted to trauma centre versus nontrauma centre, the trauma centre group had a lower mean age, greater proportion of males, and more likely to have been admitted from MVC. The trauma centre group also had a greater rate of associated neurovascular injury.
Different management patterns such as whether the individual had a soft-tissue reconstruction, external fixation, or amputation were assessed. Their long-term outcomes, such as incidence of infections, malunion or nonunion, and compartment syndrome for up to 1 year were also assessed. Table 2 shows the unadjusted odds of the above outcomes between those directly admitted to TC compared to those admitted to nontrauma centre. Our analysis demonstrated that greater proportion of the trauma centre group had soft-tissue reconstruction in 90 days (OR 3.54, P < .0001). The trauma centre group also had a greater proportion of people who had very early soft-tissue coverage within 72 h (OR 1.75, P = .0066). In contrast to the total proportion being larger, the trauma centre group had longer time to soft-tissue surgery, compared to those who had surgery in a nontrauma centre. The trauma centre group also had a longer stay in the hospital as demonstrated in Table 3.
Categorical Outcomes of Individuals with Open Tibia Fractures, Comparing Those who Were Admitted to a TC to Those Admitted to a non-TC.
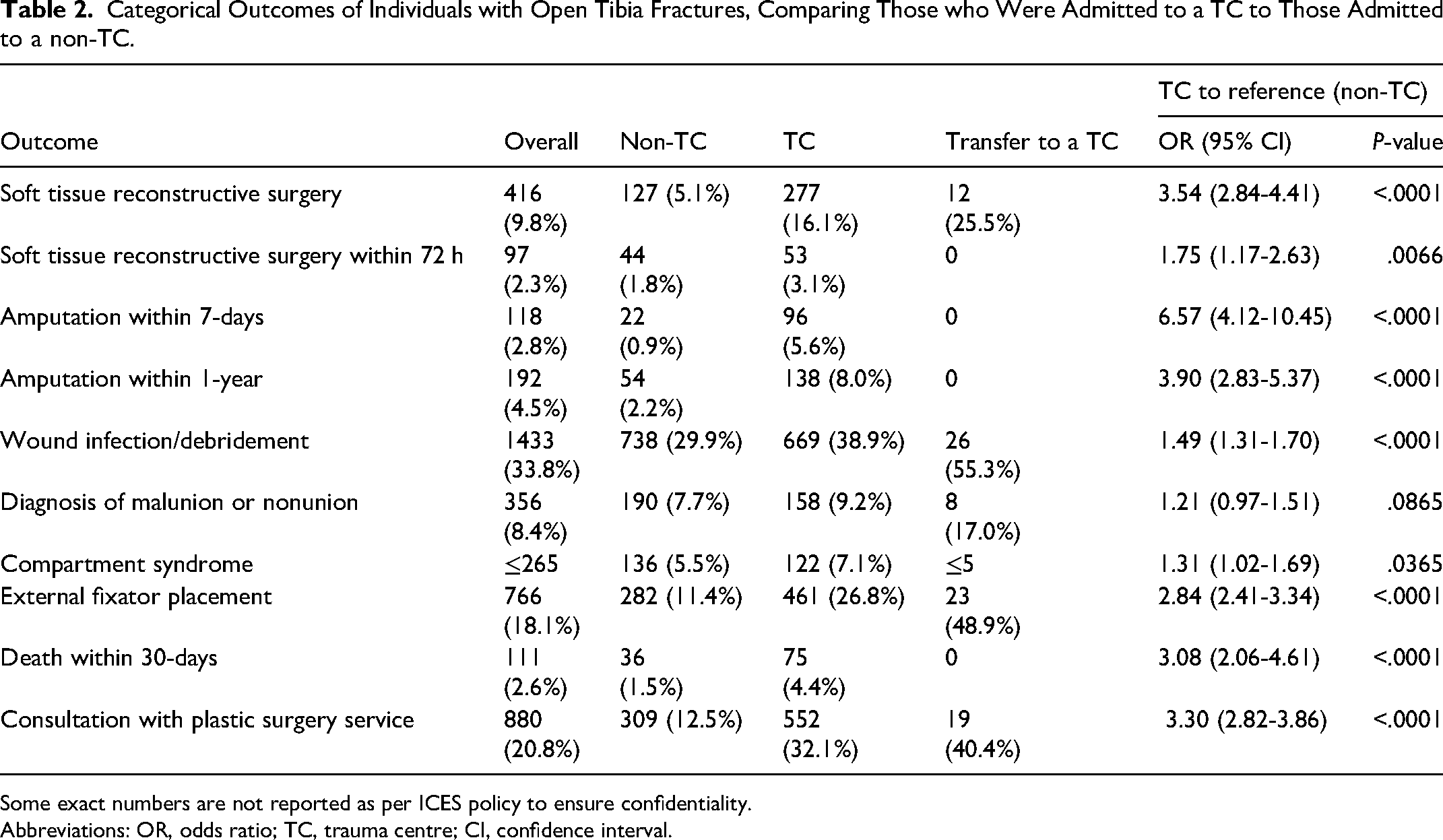
Some exact numbers are not reported as per ICES policy to ensure confidentiality.
Abbreviations: OR, odds ratio; TC, trauma centre; CI, confidence interval.
Continuous Outcomes

Regression analysis was performed considering multiple variables that were found significant in the initial baseline analysis. They were used to identify adjusted odds of patient outcomes. When adjusted, there was still significantly higher odds (OR 1.89, P < .0001) of having a soft-tissue reconstructive surgery in a trauma centre versus nontrauma centre in 90 days (Table 4). When we examined soft-tissue reconstruction within 72 h, admission location did not have a significant effect. There were increased odds of amputation in a trauma centre, for both early (7 days, OR 2.32) and late time period (1 year, OR 1.79). We saw that in addition to admission location, other associated injuries such as whether ISS was greater than 15 or not, and the presence of a nerve and/or vascular injury affected the odds of amputation (Table 5).
Regression Analysis on Soft Tissue Reconstruction and Those Within 72 h.
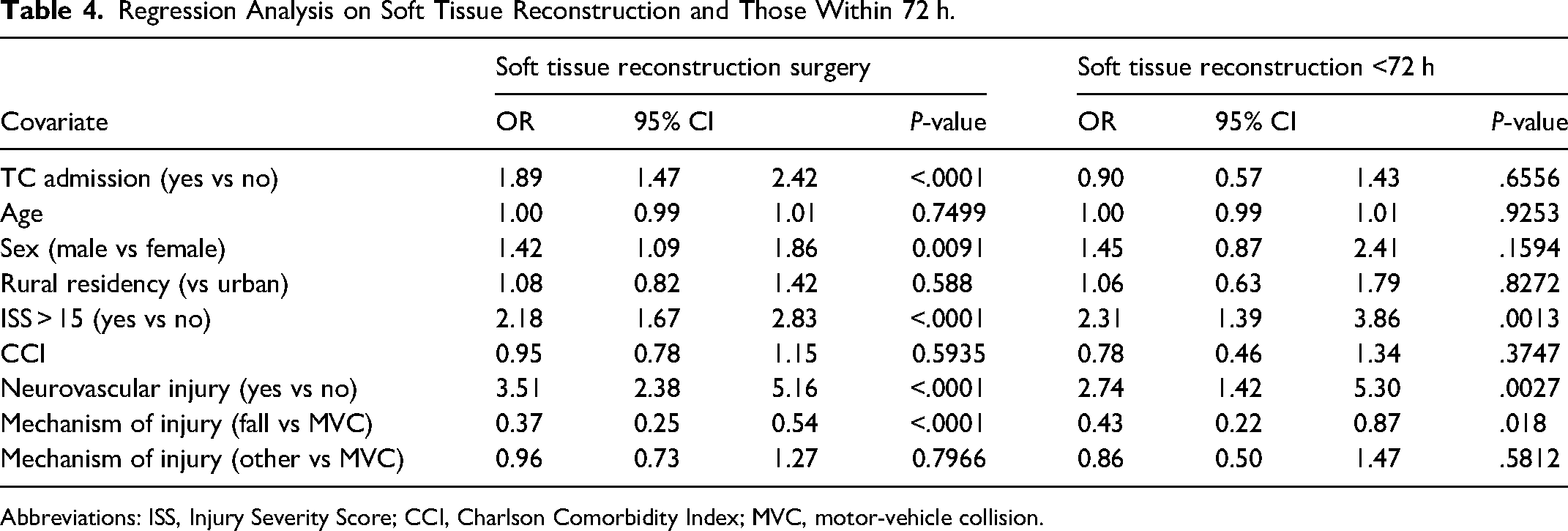
Abbreviations: ISS, Injury Severity Score; CCI, Charlson Comorbidity Index; MVC, motor-vehicle collision.
Regression Analysis on Amputation as Outcome.
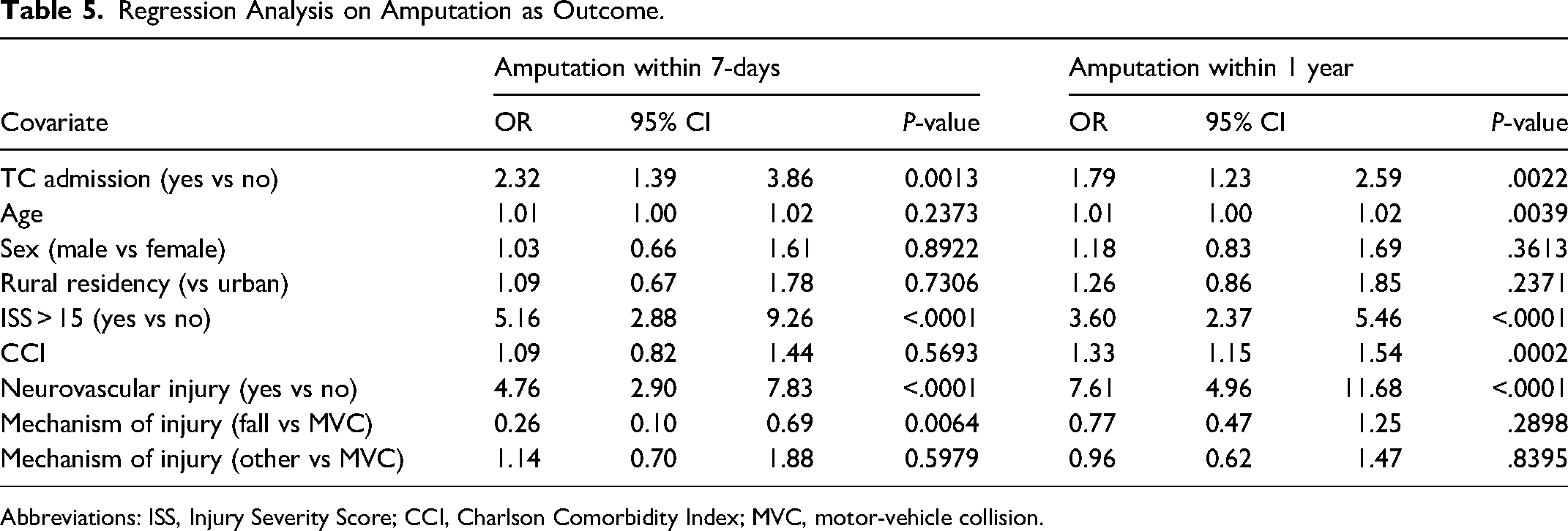
Abbreviations: ISS, Injury Severity Score; CCI, Charlson Comorbidity Index; MVC, motor-vehicle collision.
Other complication rates examined are summarized in Table 6. Admission location did not have a significant impact on the odds of infection requiring debridement or hardware removal. Admission location also did not influence the odds of malunion or nonunion. In contrast, we saw trauma centre admission significantly increased odds of having external fixation. and greater odds of having a plastic surgery consultation. Compartment syndrome was the only complication that had decreased odds in the trauma centre group. Overall, other covariates such as having ISS > 15 and the presence of neuro-vascular injury had much greater impact on the odds of developing major complications including wound infection and compartment syndrome, and placement of external fixator.
Regression Analysis on Other Secondary Variables Including Wound Infection, External Fixation, Plastic Surgery Consultation, Compartment Syndrome, Malunion or Nonunion, and Death Within 30 Days.
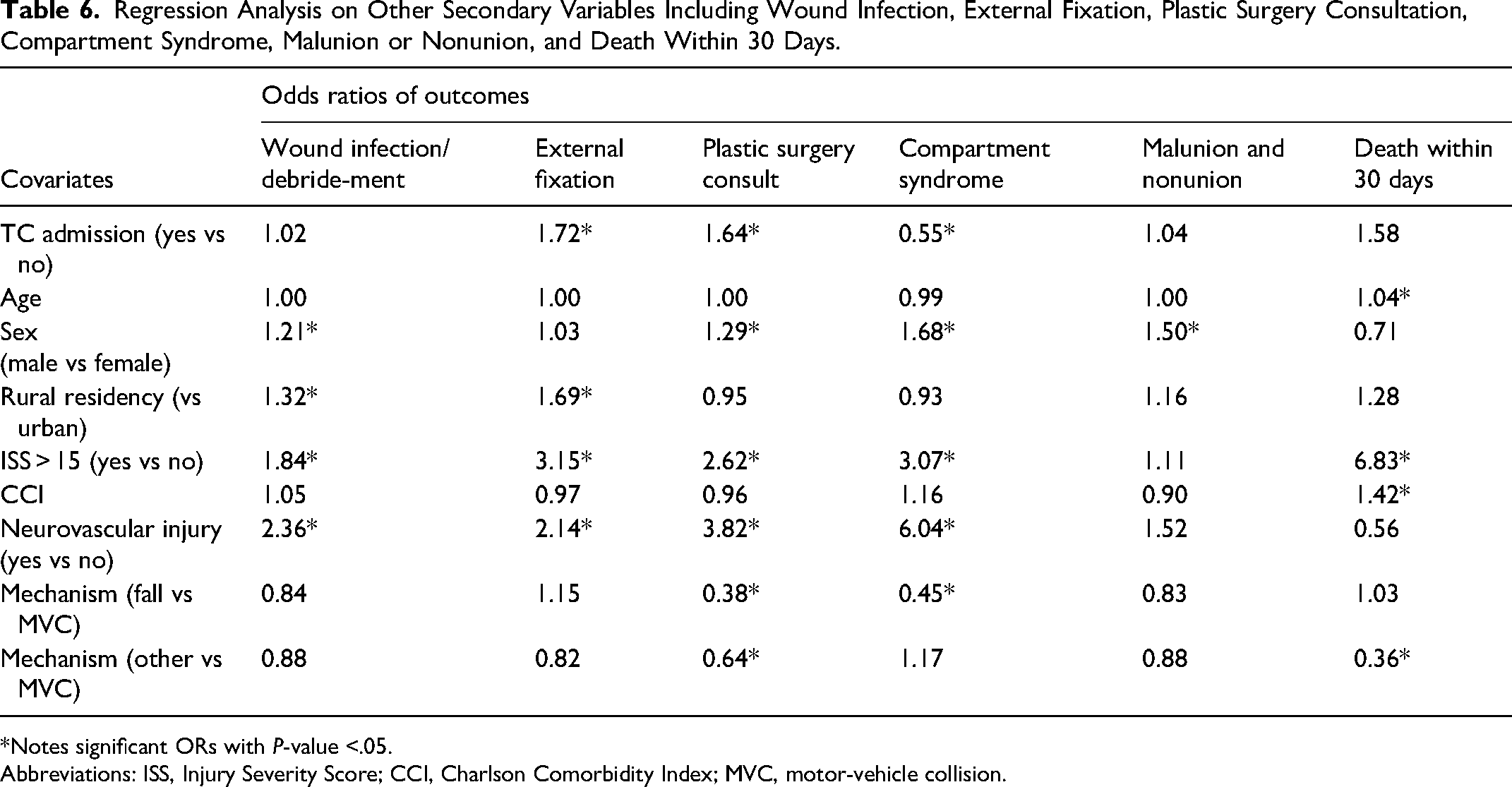
*Notes significant ORs with P-value <.05.
Abbreviations: ISS, Injury Severity Score; CCI, Charlson Comorbidity Index; MVC, motor-vehicle collision.
30-day mortality was assessed in this population. While trauma centre admission did not result in significant differences in the odds of death within 30 days, ISS > 15, age, and pre-existing comorbidities as represented by CCI, were significantly associated with increased odds (Table 6). Lastly, the length of stay in the hospital was examined. Due to the significant overdispersion of the variable, negative binomial model was used instead of a regression model. While all variables affected the length of hospital stay, trauma centre admission was associated with increased length of stay (Table 7).
Binomial Regression Analysis on Length of Stay in the Hospital.
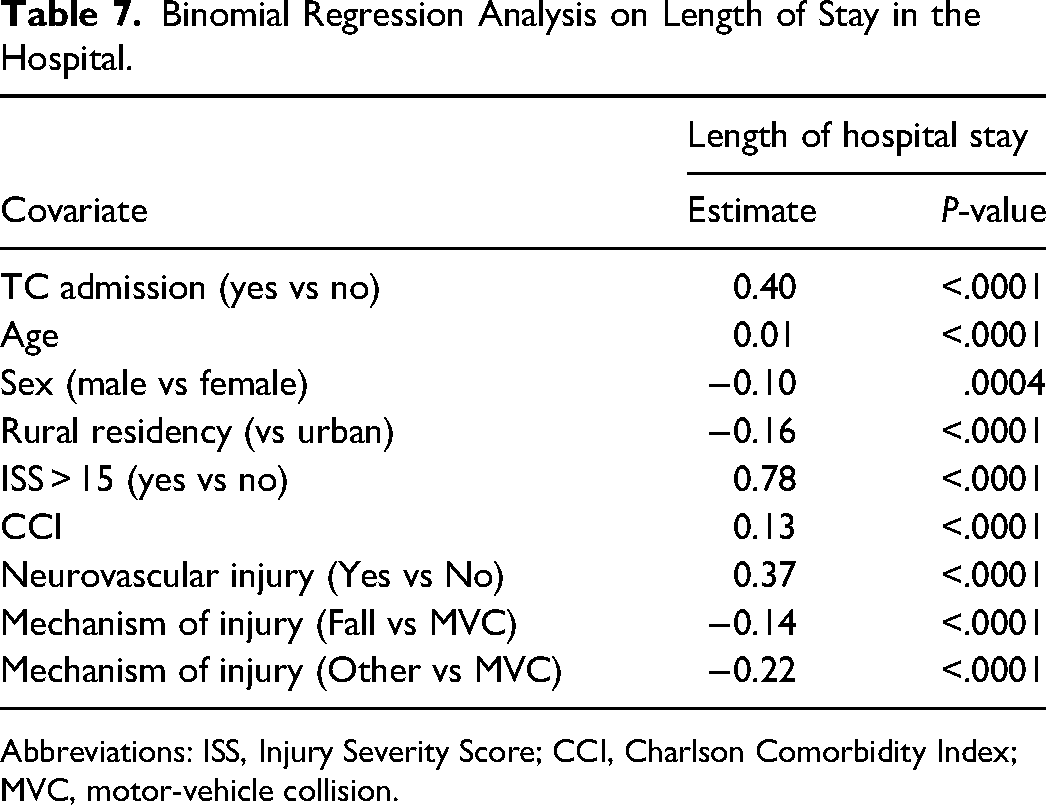
Abbreviations: ISS, Injury Severity Score; CCI, Charlson Comorbidity Index; MVC, motor-vehicle collision.
Discussion
Open extremity injuries are challenging to manage. Open tibial fractures are known for high rates of complications including infection, osteomyelitis and amputation.16-19 Expedited management with a coordinated approach by multiple experienced personnel is integral for the best patient outcome. This work aimed to describe the patient population affected by these injuries in Ontario describe their management pathways including the admission location, soft-tissue reconstruction, and rates of complications.
Utilizing the ICES, a linked-population level database, we identified our cohort population in Ontario, with all health data gathered for one year following injury. In addition to demographics and injury characteristics, the role of soft-tissue reconstruction was examined. We saw that 9.8% of those with open tibial fractures received reconstructive surgery for their soft tissue injuries. This is similar to a nationwide study in Sweden where 9% of open lower extremity injuries had significant soft tissue injury to require soft-tissue reconstruction. 12
Early soft-tissue reconstruction in open extremity injuries has been shown to improve patient outcomes.12,17,20-28 In our cohort of patients who had soft-tissue reconstruction, 97 out of 416 (23%) had the surgery within 72 h. Overall, the mean time to the surgery was 19.5 days for the entire cohort. While long, this was consistent with recent literature that time to definitive reconstructive surgery can range up to 90 days, especially with the recent use of negative pressure wound therapy.28-32 Ontario patients in this cohort undergoing management at a trauma centre had increased time from injury to soft-tissue reconstruction, which was in contrast to previous literature that showed tertiary centres with both orthopedic and plastic surgery specialists contribute to earlier definitive management.2,3 Prolonged duration between injury and definitive soft-tissue reconstruction may be from a number of factors, including critical illness, human or infrastructure availability, or local care patterns.33,34
Amputation after open tibial fractures is common. In our analysis, we looked at a 7-day timeframe to capture primary amputation, which we defined as amputation without an attempt at limb salvage. We saw significantly increased odds of primary amputation in patients managed at trauma centre, likely related to the severity of their injuries as seen in the regression analysis. When total amputation rate was examined, 4.5% of our cohort had amputation in the first 1 year. This is comparable to previous reports in the literature, where the amputation rate of open tibial fractures is between 3.6% and 8%.5,35-37 Although the majority of amputations likely occur in the first year following an open tibial fracture, we hypothesize that there will be instances of amputation outside of the timeframe examined as a result of osteomyelitis and chronic wounds. Further research in this aspect of care is warranted.
Wound infection is one of the most common complications of open extremity injuries, with the reported rates as high as 34.3%.18,19,38,39 The incidence of wound infection in our cohort was 33.8%. While admission location did not appear to have a significant impact on the likelihood of infection, the severity of injury as indicated by ISS and the presence of neuro-vascular injury significantly increased the odds of requiring irrigation and hardware removal. Complex injuries are often heavily contaminated and require numerous staged operations for debridement, orthopedic fixations, and reconstructions. These increase exposure to infections, which all could have contributed to our finding. Our methodology, which looked at patients who underwent irrigation and debridement or hardware removal, has limitations. It overestimates the infection cases since not all hardware removal is due to infection, and sometimes due to pain or malunion.40,41 On the contrary, it may also underestimate, as some infections do not require surgical debridement and are managed medically with antibiotics.
It was previously shown that lower extremity trauma patients who were directly admitted to a trauma centre had a shorter hospital stay.4,11 In our analysis, we saw the length of stay was longer in this group. The discrepancy in our results versus the other literature is likely because they compared those directly admitted to a trauma centre, to those who were transferred from a peripheral centre. On the other hand, our study compared those directly admitted to a trauma centre, to those directly admitted to a nontrauma centre. In our regression analysis, all examined co-variates including admission location, age, sex, severity of injury, and mechanism contributed to the length of stay in the hospital. These findings are consistent with factors previously discussed in the literature, with tertiary centre admissions being impacted by more complex injury, 13 complications, and repeat operations.4,11,42 Patient factors, such as increasing age and comorbidities also affect the length of stay, which we saw in our analysis.43,44
A general limitation of the study is that we were not able to account for other bodily injuries. While the ISS > 15 premium-fee code was used to adjust for other injuries, more granular information would have been valuable in the analysis. Additionally, we used administrative codes, and discrepancies can exist between what was completed in the hospital and what was recorded. 45 In addition, some of the procedures for soft-tissue reconstruction are not always well-captured by the simplified procedure codes that get documented. Future studies can address these limitations and improve methodology to better investigate extremity traumas and their outcomes.
Overall, the current study highlights the importance of close, integrated working relationships of orthopedic and plastic surgery teams in managing complex lower extremity traumas. Centralization of complex care to major tertiary centres has been proposed to expedite care, where dedicated specialists are available for assessments and management. Our analysis showed that soft-tissue reconstruction can still be significantly delayed in trauma centres, likely due to a variety of reasons including critical illness, concomitant injuries, and lack of hospital resources such as staffing. While the provision of complex care may be more available in larger centres, without the coordination of teams and resources, delays may occur, unnecessarily prolonging the time to reconstruction and increasing the likelihood of complications.10,17,27,46
A new concept that could be entertained to optimize care in this patient population is an “orthoplastic” surgery team. The orthoplastic team, as the name suggests, would have both orthopedic and plastic surgeons that would assess lower extremity traumas simultaneously for the need for bony and soft tissue surgery early in the trauma triage process. In addition to the accelerated assessments, a dedicated operating time where such multidisciplinary team can work concurrently, can ultimately save resources for the healthcare system. This model has been highly successful in other public healthcare settings,1-3 and something that could be adopted in Canada in high volume trauma centres.
Conclusion
This study is the first of its kind to analyse lower extremity trauma management in Ontario. It provides evidence for initiating conversations on trauma triage and management at an institutional and provincial level to discuss new guidelines and policies for best outcomes in extremity traumas. These results may be used as a baseline for future studies, including implementation of interventions to improve outcomes. There remains room for improvement in aspects of open fracture management, including encouraging better coordination between different surgical teams, and facilitating earlier soft-tissue reconstruction for best patient outcomes.
Footnotes
Acknowledgments
The authors thank Dr Blayne Welk for his role as an ICES scientist in overlooking the study.
Author Contributions
A.S. provided study conception, funding, and longitudinal guidance. S.K., AM
Statement
This work was completed as part of the Masters of Science in Surgery project of the first author (S.K.). The complete thesis has been published in the online library of Western University.
Ethical Statement
The use of the data in this project is authorized under section 45 of Ontario's Personal Health Information Protection Act (PHIPA) and does not require review by a Research Ethics Board.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). The study was completed at the ICES Western site, where core funding is provided by the Academic Medical Organization of Southwestern Ontario, the Schulich School of Medicine and Dentistry, Western University, and the Lawson Health Research Institute. This study also received funding from the Dr Christopher G. Scilley Fund, which is administered by the Schulich School of Medicine and Dentistry, Western University. This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from ©Canada Post Corporation and Statistics Canada. Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information (CIHI) and the Ontario MOH. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.