
Abstract
Introduction
The tibia is the most common long bone to be fractured. 1 Whilst, open tibia fractures represent a small proportion, they have a high morbidity.1,2 The Gustilo–Anderson (GA) classification is most commonly used to define open fractures. 3 In GA IIIB fractures, the soft tissue damage is severe and require flap coverage of the defect. The National Institute for Health and Care Excellence guideline recommends that flap coverage of open fractures should be performed within 72 h, while the Orthopaedic Trauma Association recommendation is for within a week.4,5 However, a study in the United States found that most patients do not receive flap coverage within 72 h. 6 A multicentre cohort study found that a delay in flap coverage of the soft tissue defect for more than a week is associated with poor outcomes. 2 Several other studies found that a delay in flap coverage of Grade IIIB fractures can lead to increased infection rate and flap complications.7–9 However, some of these studies only included outcomes in the index admission, 2 while others included tibial plateau, Pilon and ankle fractures.7–10 Also, these studies included patients with bone loss and bilateral open injuries. There is limited literature on the long-term outcomes of GA grade IIIB isolated midshaft tibial fractures (Arbeitsgemeinschaft für Osteosynthesefragen [AO] type 42 fractures). This study will further contribute to the consensus that the timing of flap coverage procedures is a critical component of post-operative outcomes, with specificity to both GA grade IIIB and IIIC, AO type 42 fractures. Furthermore, the benefits in terms of perceived cost savings and patient outcomes may prove substantial in influencing treatment management protocols within tertiary trauma centres.
The aim of study is to investigate whether a delay in flap coverage of AO type 42 tibia fractures results in increased deep infection rate. Secondary outcome measures are revision surgery, union rate and flap failure. Patient with potential confounding factors will be excluded or controlled in the analysis. It is hypothesised that patients with a delay to flap coverage of the soft tissue defect will have a higher rate of deep infections.
Methods
A retrospective cohort study was conducted to compare outcomes from delay to flap coverage. Data was gathered from a consecutive series of patients admitted to a tertiary trauma centre in Brisbane, Australia, with open tibia fractures who were recruited from a prospectively collected trauma database from 2012 to 2020. The patients included were over 18 years of age and had a midshaft (AO-42) open tibia fracture that required soft tissue coverage (GA grade IIIB or C) with at least 6 months follow-up. The exclusion criteria were patients lost to follow-up, with bilateral open fractures or a fracture at the tibial plateau, Pilon or ankle. Potential confounders to outcomes such age, sex, AO fracture classification and smoking status were collected. Ethical approval to review the patient's charts for long-term follow-up was gained from the Hospital Human Research Ethics board (Approval number LNR/2019/QMS/58750).
The patients’ records, imaging and follow-up documentation were reviewed to collect the demographics data and outcomes. Patients were divided into two groups, those who had flap coverage within a week and those covered after a week. The clinical outcomes of interest were deep infection, aseptic non-union, flap failures, revision surgery and the need for amputation. Aseptic non-union was defined as lack of bridging callus on at least three cortices on X-ray or CT scan 6 months after injury. A deep infection was defined as an infection involving the bone on tissue cultures. Flap failure was defined as flap necrosis or return to the operating theatre for revision of the flap. Patient underwent below or above knee amputation if there was a persistent infection despite treatment or painful non-functioning limb.
The standard of care in our orthoplastic unit is that patients have a dose of 2 g Cefazolin administered immediately within 1 h of arrival to the emergency department and continued for 24 h. Additionally, tetanus was given to patients with uncertain vaccination history. Alongside this, surgical debridement was performed within 24 h of presentation. For severe tissue defects, oral antibiotics were continued for 5 days or until soft tissue coverage was established. A negative pressure dressing is placed in the initial debridement, and the aim is to have soft tissue coverage within a week. However, at times due to resource availability or patient factors, a delay to flap coverage occurs.
Statistical analysis
The Program SPSS Statistics v26 (SPSS Inc., Illinois, USA) was used to perform statistical analysis. The primary outcome measure was the rate of deep infection. Secondary outcome measures were revision surgery, aseptic non-union and flap failure. A Pearson chi-squared was used to determine whether there is a significant difference in outcomes between patients who had flap coverage within a week and those who did not. Analysis of the demographic was performed using t-test for normally distributed data, Mann–Whitney U test for data that was not normally distributed and chi-square test for categorical variables. Also, a binary logistics regression analysis was performed to assess the effect of potential confounding factors on deep infection rate. A significance level p < 0.05 was used for analysis.
Results
Demographics
A total of 109 patients were drawn from the trauma database who had a grade IIIB or IIIC open tibia fracture from 2012 to 2020 (Table 1). Fifty-five of these patients had an isolated midshaft fracture (AO-42) with a follow up longer than 6 months. 18 (33%) patients had flap coverage within a week and 37 (67%) after a week. Two patients in each group had a GA IIIC injury. The patients’ age, gender, smoking status, Injury Severity Score (ISS) and mechanism of injury were not significantly different between the two groups (Table 1). Also, the two groups had a similar distribution of fracture types as per the AO classification. One patient in the early coverage group required a Masquelet technique.
Patient demographics.
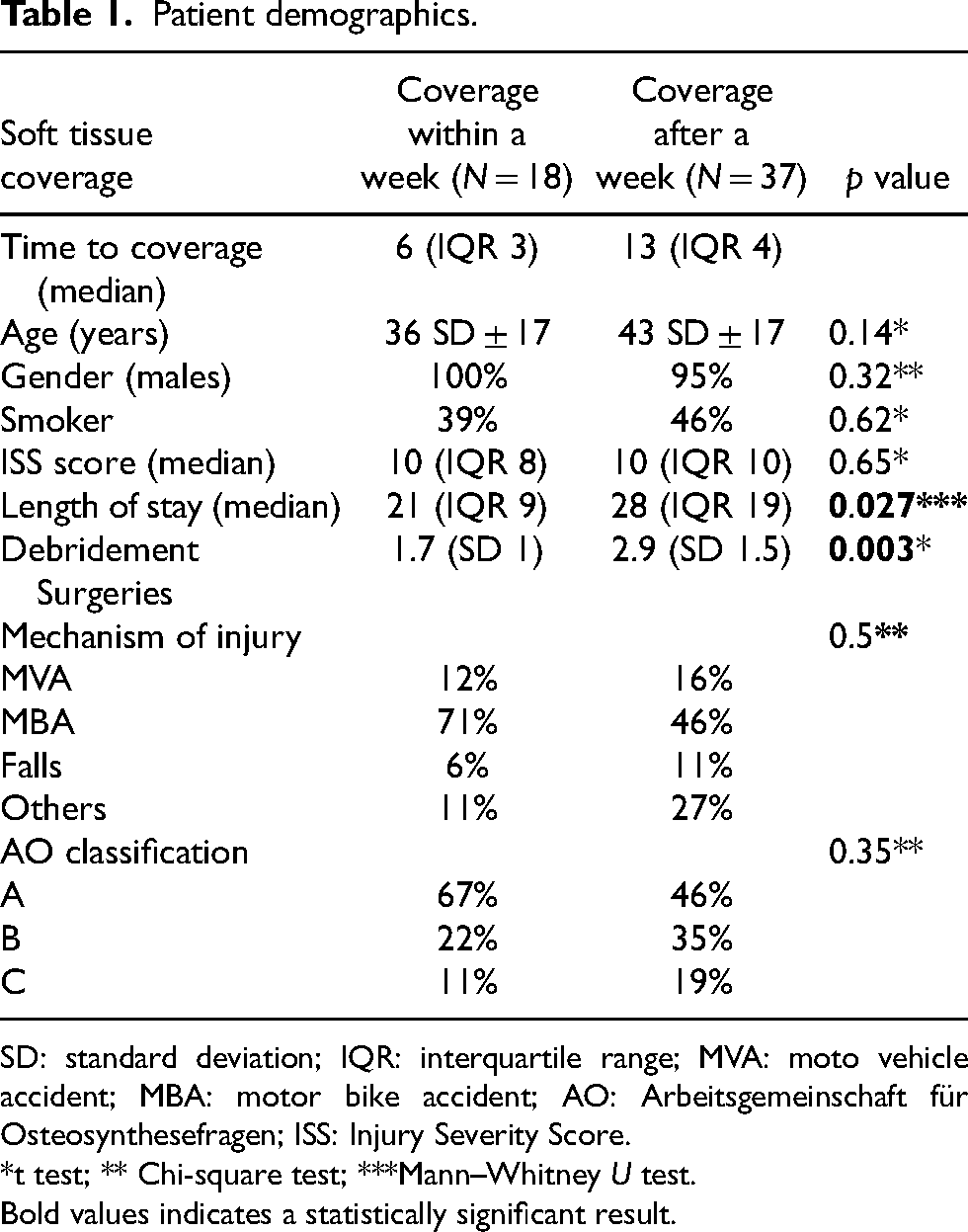
SD: standard deviation; IQR: interquartile range; MVA: moto vehicle accident; MBA: motor bike accident; AO: Arbeitsgemeinschaft für Osteosynthesefragen; ISS: Injury Severity Score.
*t test; ** Chi-square test; ***Mann–Whitney U test.
Bold values indicates a statistically significant result.
Management
The two groups received similar management (Table 2). All patients had broad-spectrum intravenous antibiotics and tetanus on arrival in the emergency department. The initial management was external fixation and debridement in most cases. Negative pressure dressing was used in 95% of patients in both groups. In patients covered within a week, 10 (56%) received a gracilis flap, 4 (22%) an anterolateral thigh flap, 2 (11%) a latissimus dorsi flap and 2 (11%) a local flap. In patients covered after a week, 16 (44%) received a gracilis flap, 12 (32%) an anterolateral thigh flap, 2 (5%) a latissimus dorsi flap, 2 (5%) a radial artery free flap and 5 (14%) a local flap.
Management characteristics of patients with open tibia fractures requiring flap coverage.

Outcomes
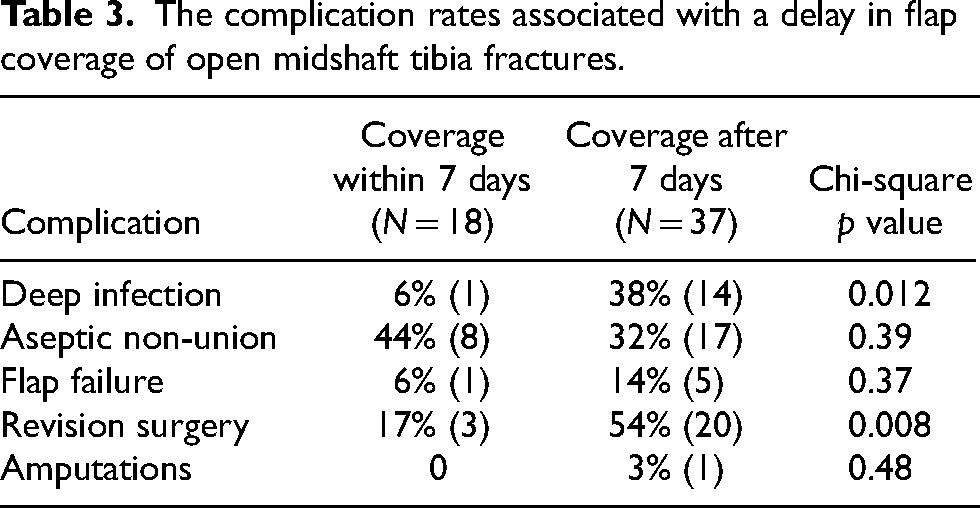
Chi-square analysis result is demonstrated in Table 3. The rate of infections and revision surgery was significantly higher in patients who had delayed flap coverage. The patient who had a deep infection in the early coverage group had an ipsilateral grade IIIB femur fracture which complicated the clinical course. The infection was suggested to begin in the femur and later involve the tibia. The most common causes of infections were multi-organisms, Staphylococcus aureus and Serratia marcescens (Table 4). The single flap failure in patients covered within a week was necrosis of the flap which required debridement and split thickness skin graft. The five flap failures in the delayed group were returned to theatre for revision of the flap. Four of the five failed flaps were due to infection and necrosis of the flap, while the other was due to poor perfusion in the days following the procedure.
The complication rates associated with a delay in flap coverage of open midshaft tibia fractures.
The types of bacteria causing deep infection in Gustilo–Anderson grade IIIB/C fractures.
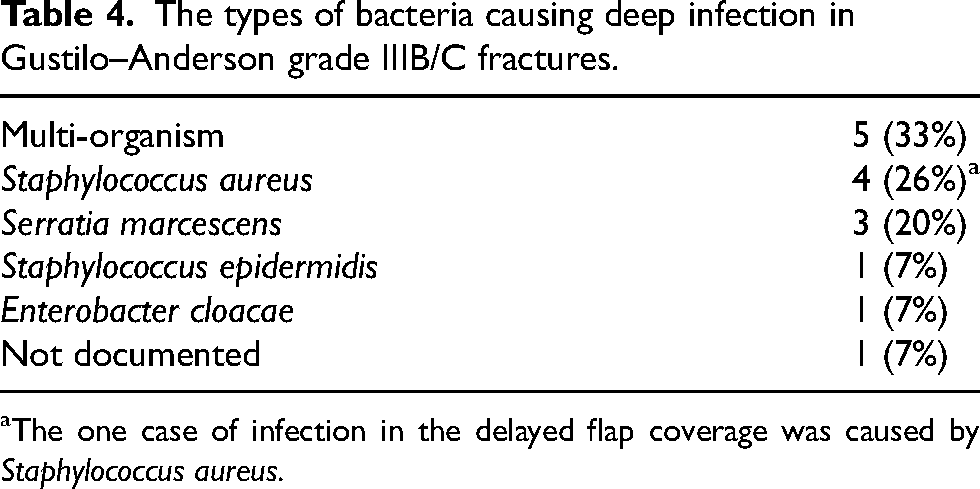
aThe one case of infection in the delayed flap coverage was caused by Staphylococcus aureus.
Revision surgery was 17% in patients who had soft tissue coverage within a week and 54% in those later than a week. In the early coverage group, the revision surgeries were two tibial nail dynamisations and one removal of metalware. In the delayed coverage group, the revision surgeries were eight tibial nail exchanges, seven removal metalware and external fixation, three tibial nail dynamisation, one bone grafting of the fracture site and one removal of metalware. The rate of non-union was high in patients who had early flap coverage. However, only two (2/8) patients required dynamisation to reach union, while the rest achieved union without an intervention. In the delayed coverage group, (8/17) eight patients required operative intervention to achieve union which is double the rate of patients with early coverage. Two (12%) superficial flap infections occurred in patients covered within a week that were treated with antibiotics. One patient in the delayed coverage group progressed to a below knee amputation.
A forward model binary logistics regression for deep infection was performed and included coverage group, age, ISS score smoking status, AO classification and fixation method. Patients who had flap coverage after a week were 10 times more likely to develop a deep infection (95% confidence interval: 1.2–83, p = 0.034).
Discussion
The results of this study indicate that a delay in soft tissue coverage of open tibia fractures is associated with an increase rate of deep infection and revision surgery. This study supports previous literature to further illustrate the importance of early flap coverage of open tibia fractures.2,10–12 Our study controlled for potential confounding factors such the ISS, smoking status, age, fracture severity and fixation method. Also, our minimum follow up of 6 months allowed for the assessment of the rate of non-union which other studies did not.2,8 Pincus et al. performed a retrospective study across 140 trauma centres in North America. Similarly, to our findings, most patients in that study (61.3%) did not have flap coverage within 7 days. Pincus et al. demonstrated a significant increase in surgical complications when compared with early definitive flap coverage (16.7% vs. 6.2%; p < 0.001). However, Pincus et al. only studied the complications rate in the index admission and included fractures in the Pilon, ankle or plateau; while our study included long-term follow up and excluded those type of fractures. Another study that included Pilon and plateau fractures, found for a delay in coverage after 7 days, the risk of infection rises by 16% daily. 8 Some authors went as far to suggest a radical fix and flap approach.7,9,13 However, it is acknowledged that such approach is not always possible usually due to the presence of multiple other injuries. 7 The current literature supports the findings of this study that a delay in flap coverage increases the risk of infections.
Our patients had a comparable rate of aseptic non-union and revision surgery to previous studies.14,15 The high rate of non-union can be explained by the severity of soft tissue injury and high proportion of smokers.16–19 A sub-analysis demonstrated that the rate of patients with aseptic non-union that require surgical intervention to achieve union is doubled by a delay in flap coverage (25% vs. 47%). This further illustrates that patients who had delayed flap coverage and develop non-union are more likely to need surgical intervention even without an infection.
Limitations
The limitations of this study are that it is retrospective and the reasons for delay were not documented. The study had low numbers in each group and is underpowered despite a long recruitment period due to the rarity of such injury. We were not able to determine whether flap coverage within 72 h improved outcomes as very few patients were in that group. In addition, the patient functional outcomes were not recorded.
Conclusion
A delay in soft tissue coverage of open tibia fractures greater than a week is associated with an increase rate of deep infection and revision surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.