
Abstract
Background
Traditional apprenticeship models in surgery required that trainees performed some menial tasks so that the specialist could supervise the acquisition of knowledge and skills in more complex areas. 1 Because trainees acquire knowledge and skills at different rates and possess different proficiencies, Competence by Design (CBD) was introduced by the Royal College of Physicians and Surgeons of Canada in order to ensure that all graduates of medical speciality programs meet a core set of milestones.1–8 At the start of residency, the trainees are provided with a well-defined set of learning objectives, referred to as Entrustable Professional Activities (EPA's), with progress contingent upon the successful completion of each. 8
Burn care has played an important role in the history and development of plastic and reconstructive surgery, and still contributes significantly to the clinical workload and training of plastic surgeons internationally. Even if patients with burn injuries are referred on to burn sub-specialists, it is essential for all plastic surgeons to be able to assess and initially manage a burn-injured patient. Only the burn rotation provides trainees with exposure to the assessment and management of both minor and major burns, as well as the deteriorating or critically ill patient with a burn injury. The nature of modern burn care also exposes plastic surgical trainees to numerous other clinical activities such as the assessment and management of complex skin and soft tissue wounds, the co-ordination of difficult bio-ethical problems, and the routine integration of scientific research into clinical practice.
And yet, because of the breadth of the speciality and the competing pressures from other sub-specialties, time allocated to the training of plastic surgical residents in burn care has progressively been reduced, compromising clinical service delivery in burn centres, contributing to the predicted shortage of burn surgeons, while also resulting in the suboptimal training of community plastic surgeons who should be capable of providing competent initial assessment and management of many burn injuries and wounds.9–16
The purpose of this study was to determine which plastic surgery EPA's are amenable to completion by plastic surgery residents during their rotation at the Ross Tilley Burn Centre (RTBC) at Sunnybrook Health Sciences Centre in Toronto. The RTBC is responsible for the management of most major adult burn injuries in Ontario, home to approximately one-third of the Canadian adult population. One of only two adult burn centres in Canada verified by the American Burn Association, The RTBC is affiliated with the University of Toronto, and residents from at least two other plastic surgery training programs also complete burn rotations here. We hypothesized that there is exposure to many of the 52 plastic surgery EPA's during a three month burn rotation.
Methods
Out of a total of 52 plastic surgery EPA's defined by the Royal College of Physicians and Surgeons of Canada, 26 were deemed potentially relevant to the burn rotation by the two investigators. These 26 were determined by consensus of the two investigators, based on the procedures and activities commonly undertaken at the burn centre. The remaining 26 were excluded from the survey to reduce its length and because the activities referred to were regarded as more regularly undertaken during other rotations.
An anonymous questionnaire using Survey Monkey (Momentive, San Mateo, California, USA) was distributed to residents who completed a burn rotation in the seven years between 1 January 2015 and 31 December 2021. Data collected included demographics as well as year and length of burn rotation undertaken, as well as the respondent's training program and current career stage. The survey comprised 31 questions, and an opportunity to add additional comments about the burn rotation at the end. Most of the survey requested of the respondents to evaluate their opportunity to perform a list of EPA's, based on a 5 point scale, by selecting one of “none at all”, “a little”, “a moderate amount”, “a lot”, or “a great deal”. Data was transferred from Survey Monkey to Microsoft Excel for graphing and analysis, and represented as numbers of respondents with means and percentages. T-test inferential statistical tests were performed with significance reported as p values less than 0.05.
Results
Forty-nine plastic surgery residents completed the burn rotation at RTBC during the relevant period. Of these, the contact details (email address and cellular telephone numbers) of 42 residents were readily available and invited to participate. Thirty-two residents completed the survey within two weeks of the request, representing a 76% response rate.
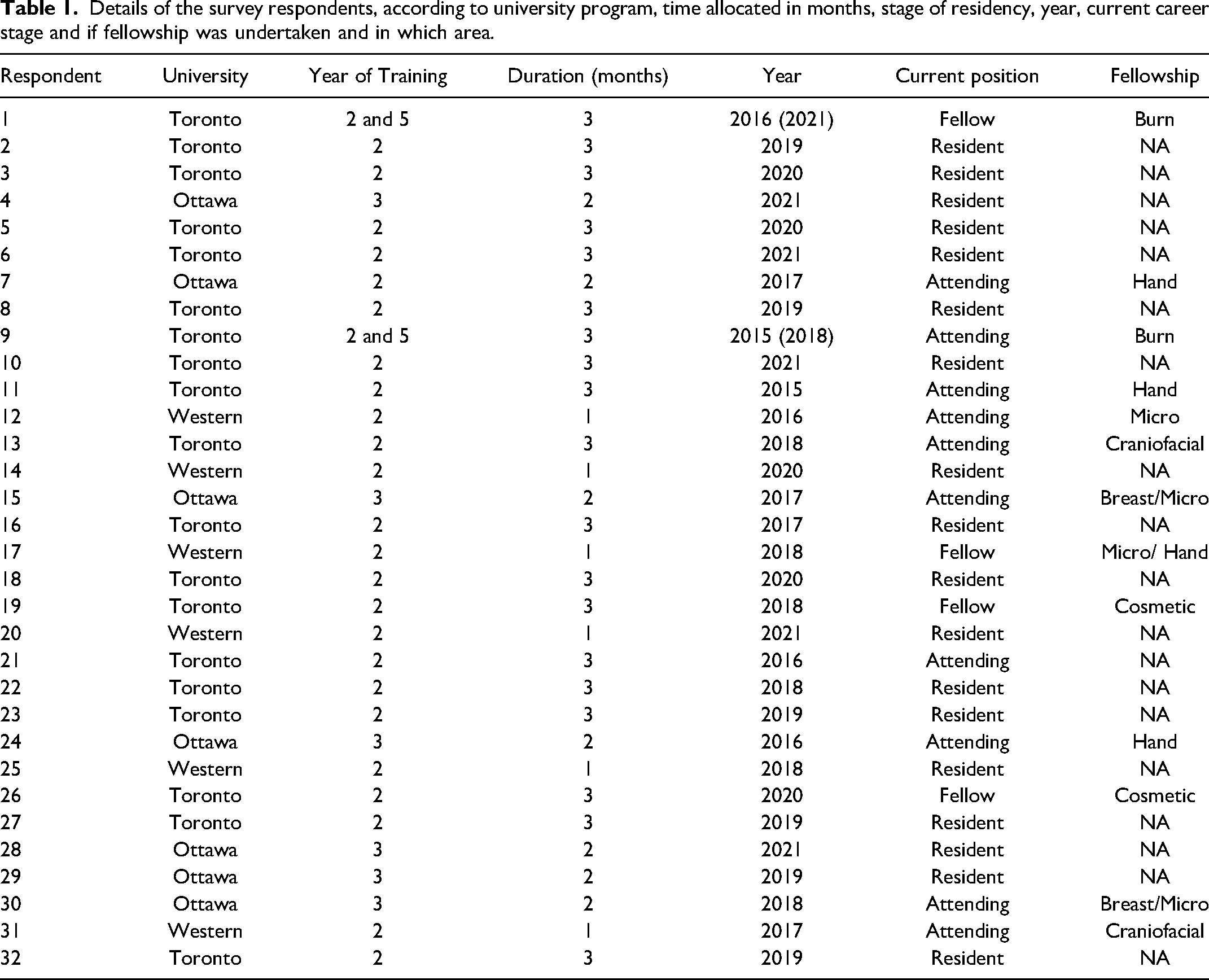
Nineteen of the respondents (59%) undertook their burn rotation in their second year of residency at the University of Toronto, 6 (19%) while in their second year at University of Western Ontario plastic surgery training program, and 7 (22%) during their third year at the University of Ottawa. The largest proportion of residents completed their rotation in 2018 (n = 6, 19%). Two of the residents also undertook a senior rotation in the burn centre, and then a burn fellowship at another centre. The respondents’ details (university program, year, duration allocated to burns, career to date) are summarised in Table 1.
Details of the survey respondents, according to university program, time allocated in months, stage of residency, year, current career stage and if fellowship was undertaken and in which area.
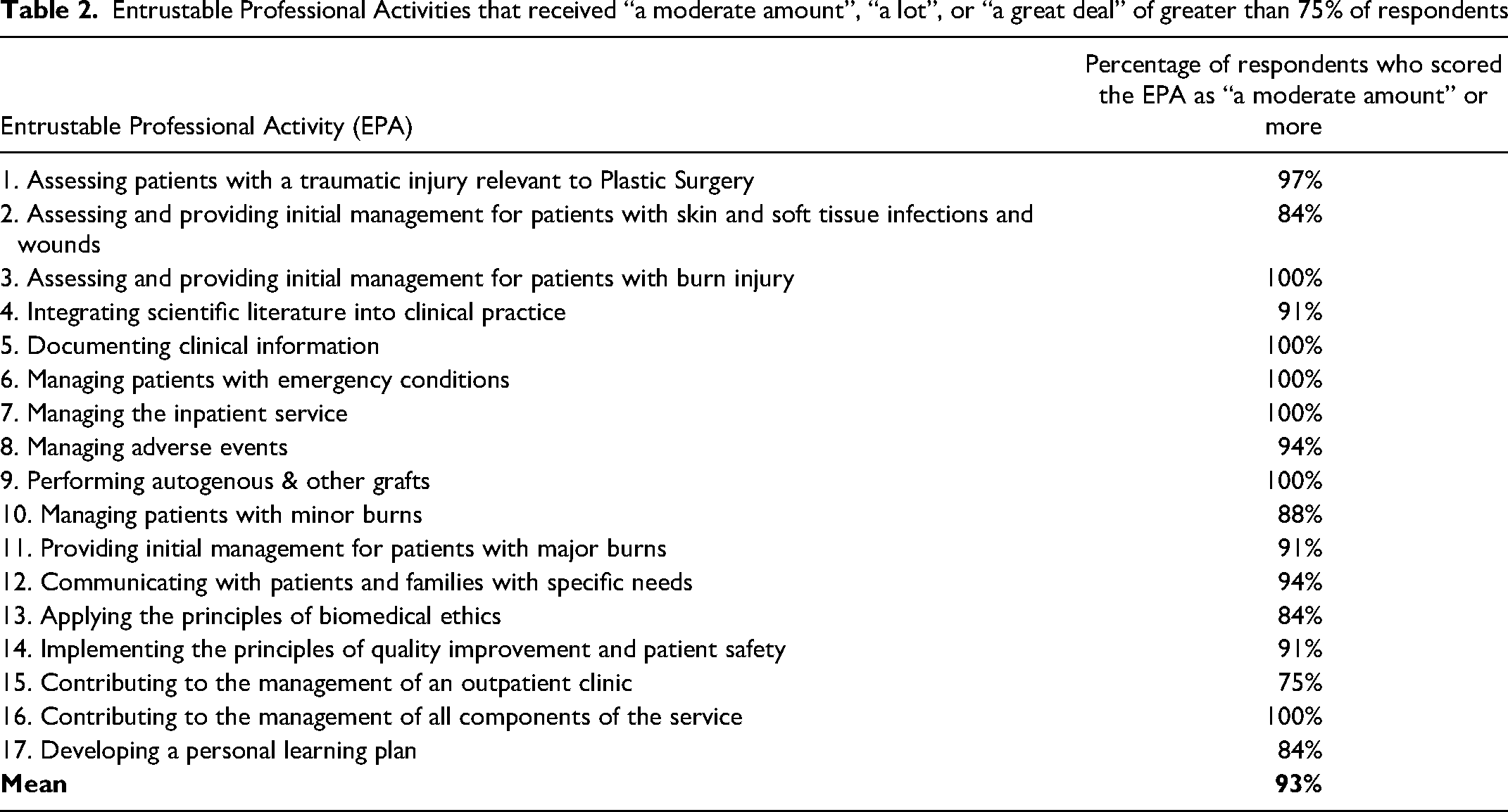
Seventeen of the 26 EPA's evaluated were judged by more than 75% of respondents as “a moderate amount”, “a lot” or “a great deal” (Table 2). These reflect activities relevant to the management of the inpatient burn and plastic surgery service, such as assessing and providing initial management for patients, accurately documenting clinical information, excising burn wounds and covering them with either autograft or allograft, managing emergencies and communicating with the patient and family. Six EPA's received “a moderate amount”, or more, from all respondents (Table 2).
Entrustable Professional Activities that received “a moderate amount”, “a lot”, or “a great deal” of greater than 75% of respondents
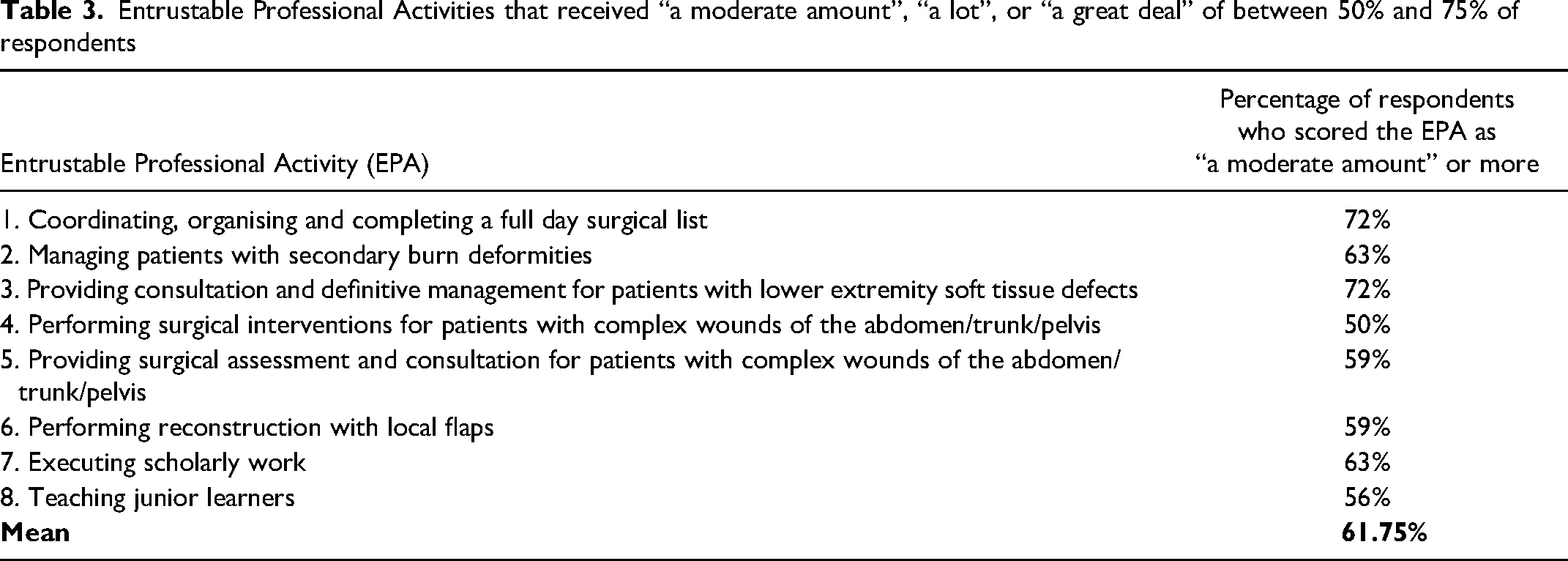
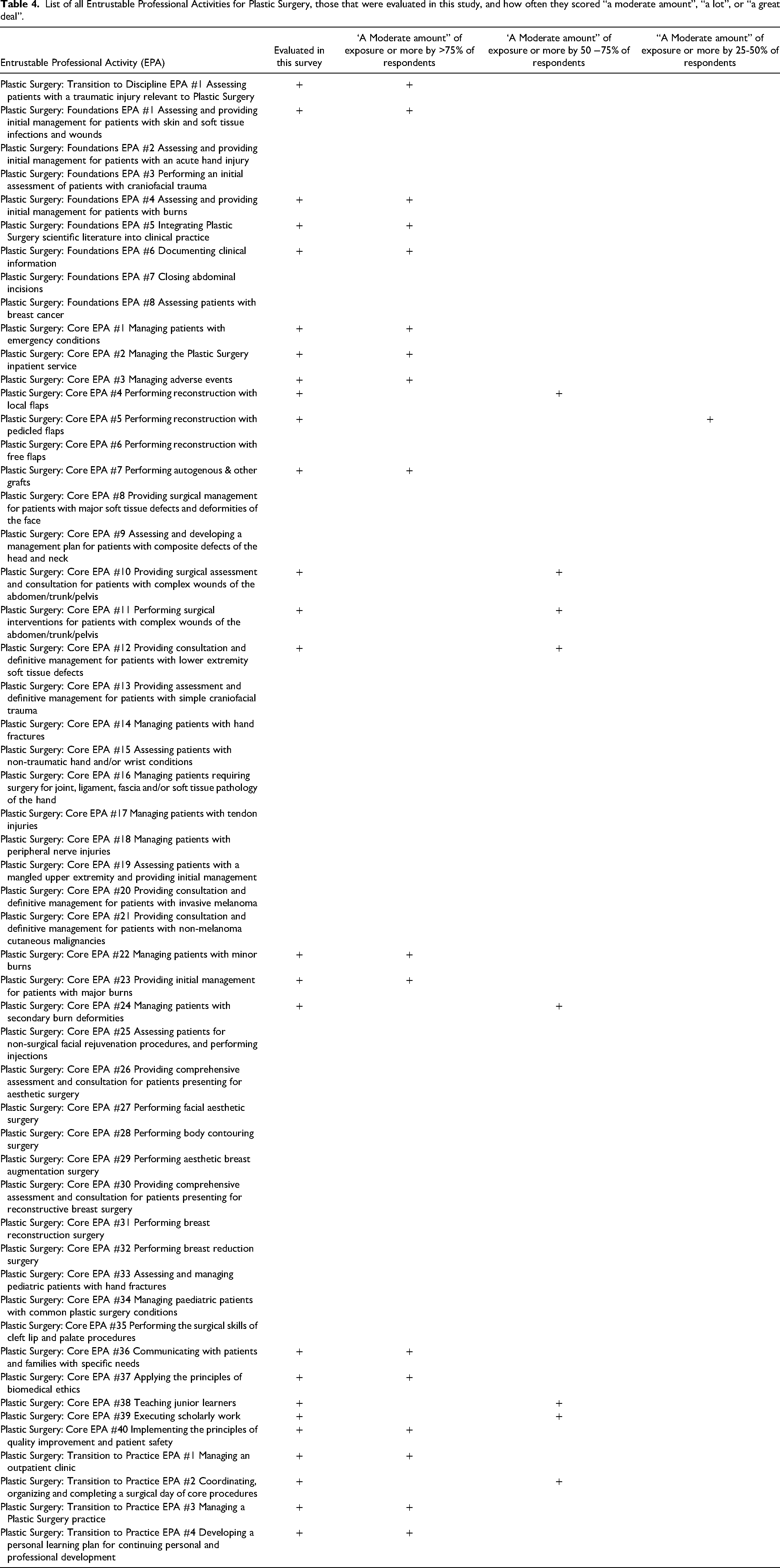
Those EPA's which received more than 50% but less than 75%, for “a moderate amount”, or more, are listed in Table 3, and include a further 8 EPA's. The complete list of all plastic surgery EPA's, those that were judged in this survey, and how they scored relative to others, are documented in Table 4.
Entrustable Professional Activities that received “a moderate amount”, “a lot”, or “a great deal” of between 50% and 75% of respondents
List of all Entrustable Professional Activities for Plastic Surgery, those that were evaluated in this study, and how often they scored “a moderate amount”, “a lot”, or “a great deal”.
The EPA that was regarded as the least available for completion of the 26 was “performing reconstruction with a pedicled flap”, with 28% (n = 9) of respondents stating they were exposed to this EPA “a moderate amount”, “a lot” or “a great deal”. “Executing scholarly work” (n = 8; 25%) and “performing reconstruction with a pedicled flap” (n = 7; 22%) were the only two EPA's evaluated in this survey that received “none at all” from more than 20% of respondents.
Comparing those who undertook a three month rotation (ie those from the University of Toronto; n = 19) versus those whose rotations were shorter (n = 13), the percentage of respondents who scored the EPA's in Table 3 as “a moderate amount” or more, was significantly lower for the latter category of trainees (mean EPA score 55.8%; population mean 61.8%; p = 0.048). This difference was not noted in the first group of (higher scoring) EPA's represented in table one (mean EPA score 91.6% vs population mean 93%; p = 0.23).
In the free text sections following each multiple choice question, a variety of comments regarding the burn rotation were shared with the investigators. Exposure to the comprehensive care of the major acute burn, and quality improvement processes, were regarded as positive aspects of the rotation. Consistent themes that emerged included the need to introduce three month rotations for those training programs allocating shorter (one or two month) rotations, and requests for greater exposure to complex wound surgery and reconstructive burn surgery. Furthermore, the consistent allocation of at least two residents to this program, in addition to the two fellows, was considered necessary to allow for greater involvement in the important area of outpatient follow-up, while not compromising on acute burn surgery and burn critical care. Respondents also identified interest in more opportunities to participate in traditional research and quality improvement interventions while allocated to burns.
Discussion
Our survey revealed that plastic surgery residents have an excellent opportunity to complete one-third (17 out of 52) of the required plastic surgery EPA's during their burn rotation. Furthermore, there is at least some opportunity to complete a further 8 EPA's, thus accounting for 25 (almost half) of all those required by the Royal College of Surgeons.
Our results reinforce not only the educational benefits of the burn rotation, but also demonstrate an excellent opportunity to increase resident exposure to the assessment and comprehensive surgical management of complex wounds (necrotising soft tissue infections, surgical wound complications, pressure injuries, degloving wounds, and exfoliative skin conditions), which are conditions seldom managed in other rotations. More than half of the respondents identified at least “a moderate amount” of exposure to EPA's related to complex wound assessment and care.
An unintended but potential consequence of the introduction of EPA's to specialty training, is that program directors may utilise the number of EPA's potentially acquired during a rotation, to justify the distribution and allocation of residents. In fairness, the number of potential EPAs might be one of several criteria used by program directors to deal with the practical problem of where, and for how long, to assign residents. Our findings strongly counter any argument that the burn service is a “low yield” rotation from an EPA acquisition perspective. Instead, the results of this survey should provide reassurance to program directors that a burn rotation will help trainees achieve the mandatory number of EPA's.
We have consistently noted that residents who undertook short rotations (1-2 months) had less opportunity to be involved in the range of activities undertaken in the burn centre in comparison with those who had a dedicated 3 month rotation. 13 This survey has shown that this is especially true in the category of EPA's where 50-75% of respondents selected “a moderate amount”, or more. This suggests the importance of at least a three month burns rotation for junior or intermediate residents. In addition to direct clinical experience and the coordination of a busy in- and outpatient service during their burn rotation, residents find particular value in being exposed to the burn centre's quality improvement program, issues of biomedical ethics, and the management of adverse events.
While it is clear that trainees usually obtain excellent exposure to burn resuscitation, critical care and acute burn surgery, the qualitative commentary associated with this survey reflected the need to balance clinical service on the burn critical care unit, with greater involvement in the burn clinic, particularly with respect to the assessment and management of secondary burn deformities in follow-up, as well as greater opportunities to undertake burn related research.
This study has some limitations. First, not every resident who completed a burn rotation at the RTBC over the last seven years completed this survey. However, a majority were contacted and we had a 76% survey completion rate of those invited to participate. Second, the authors, who sub-specialize in total burn care, selected the EPA's to be included in the survey, and also trained the respondents. This introduces a bias towards reporting a higher number of potential EPA's. We would argue that this is not a major limitation because the residents themselves rated the selected EPA's, and all responses were anonymous.
In conclusion, the burn rotation remains a fundamentally important part of plastic surgery training, and offers residents a significant number of the Entrustable Professional Activities (EPA's) that they require. Given the breadth of plastic surgery and the marked variation in terms of service provision to training ratios, both the number of potential EPA's as well as other criteria, (perhaps average time required to master the EPA's and site specific service considerations), should be utilised to determine the distribution of plastic surgery residents across the academic sites. We would also recommend that a comprehensive assessment of EPA's available per rotation should be regularly undertaken to ensure that resident needs are being met.
Footnotes
Author Contributions
Both authors were involved in all stages of data collection, conception, analysis, editing and final submission of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.