
Abstract
The advent of minimal pain tumescent local anesthesia injection has improved patient safety by eliminating the need for sedation for many wide awake operations, especially in patients with significant medical comorbidities. Modified radical mastectomy (MRM) for breast cancer is commonly performed under general anesthesia as it requires the dissection of the entire breast and an ipsilateral axillary lymph node dissection (ALND). General anesthesia has been shown to have a high risk in patients with severe medical comorbidities. We present a case of a 78-year-old male patient who was diagnosed with invasive ductal breast carcinoma, cardiac failure, and other metabolic abnormalities. Taking his comorbidities into account, we performed a wide awake MRM and ALND after tumescent minimal pain local anesthesia injection. The patient experienced the successful procedure safely with minimal discomfort.
The advent of minimal pain tumescent local anesthesia injection has improved patient safety, experience, and convenience by eliminating the need for sedation for many wide awake operations (no sedation).1,2 Modified radical mastectomy (MRM) and axillary lymph node dissection (ALND) for breast cancer is commonly performed under general anesthesia. General anesthesia has been shown to have a high risk in patients with medical comorbidities. We present a case of a 78-year-old male with invasive ductal breast carcinoma, cardiac failure, and other metabolic abnormalities. We performed a wide awake MRM and ALND after tumescent minimal pain local anesthesia local anesthesia injection. The patient experienced a successful procedure with minimal discomfort.
We recommend 300–500 mL of tumescent solution which contains 50 mL of 1% lidocaine with 1:100 000 epinephrine and 5 mL of 8.4% bicarbonate diluted in saline. We used a total of 300 mL of this solution in this lean male to infiltrate all tissue dissection planes as shown in Figure 1. We started with a gauge 27 needle using a gentle pinch followed by longer larger needles which were advanced only in clearly tumesced, numb tissue to avoid any sting after the first needle poke. Infiltration of the entire tissue plane under the breast was done by gently lifting it off the anterior chest wall as shown in Video 1 [accessible online at https://journals.sagepub.com/doi/full/10.1177/22925503221120573]. The breast and axilla were tumesced with visible and palpable local anesthesia 2 cm beyond anywhere that dissection was going to occur.
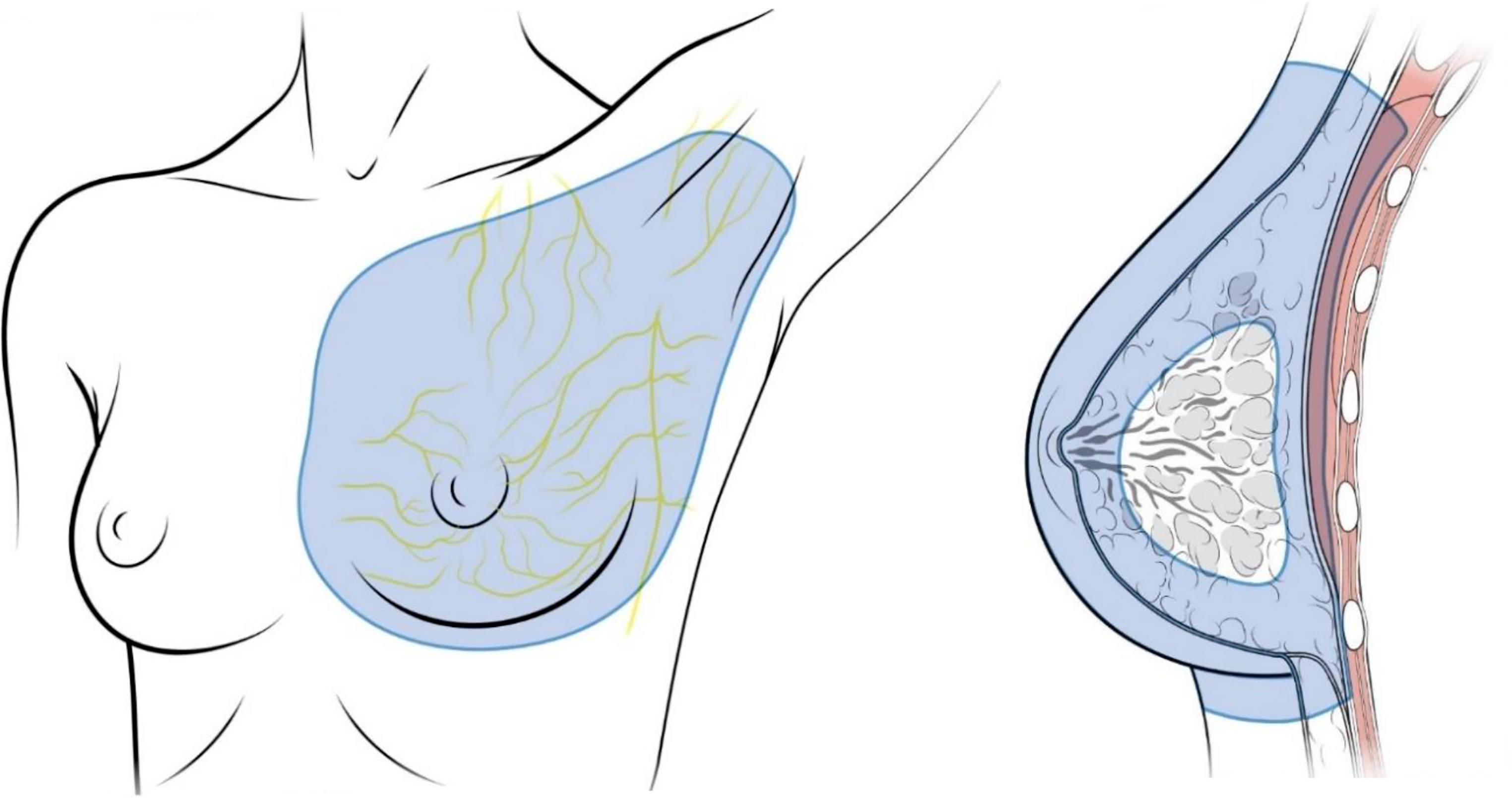
Where to inject tumescent local anesthesia for mastectomy and axillary lymph node dissection. In both males and females, generous volumes of low concentration tumescent local anesthesia should bathe an area of at least 2 cm beyond all dissection planes. Our patient was a male, but the same technique can be applied to females
We waited 30 min to give the epinephrine adequate time to work before starting the procedure Bipolar electrocautery was used to eliminate monopolar cautery conduction pain. The procedure took 40 min with a blood loss of 50 mL. The patient experienced the surgery with minimal discomfort as shown in Video 2 [accessible online at https://journals.sagepub.com/doi/full/10.1177/22925503221120573].
The use of minimally painful injection of tumescent local anesthesia can be a good option to increase availability and safety for this life saving operation. This technique may be applicable in other patients where similar factors and lack of resources limit the use of safe general anesthesia.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.