
Abstract
Introduction
The prognosis of finger performance after fracture is determined by many factors, 1 including patients’ age, associated diseases and arthritis, socioeconomic status and motivation. Stable, simple and closed fractures can be treated conservatively, and they usually heal well with minimal functional deficit.1,2 On the other hand, operative fixation is usually required for complicated, unstable or open fracture. 2 The latter usually have poorer prognosis.1,2 This happens more commonly in phalangeal fracture and when there are associated soft tissue injuries. Despite stable fixation and aggressive mobilization exercise, many patients still experience a limited range of motion. A secondary salvage procedure is usually required.
Finger stiffness is the most common complication after phalangeal fractures as a result of tendon adhesion and joint capsule contracture. 3 In a retrospective review of complications after plate fixation of phalangeal fractures, 34% (24/64) fractures had stiffness, defined as total range of motion ≤ 180°. 4 Only 11% (4/37) phalangeal fractures achieve a satisfactory range of motion greater than 220°. 5 Finger stiffness is also the most common reason for reoperation after phalangeal fractures, up to 42% to 44%.6,7 Despite the use of low-profile anatomic plate, 31.4% (7/23) patients had removal of hardware and tenolysis/capsulotomy. 8
Tenolysis is a surgical option that may improve the range of motion after hand trauma.9–13 It releases the adhesions around the tendon and joint capsule so as to restore the tendon gliding and range of motion. However, there are only a few papers investigating the outcome of tenolysis after hand fracture.9–12 By retrospectively analyzing the outcomes of tenolysis after phalangeal fractures in our center, we present our local data and aim to shed light on the potential factors that might improve the finger performance.
Method
Patient
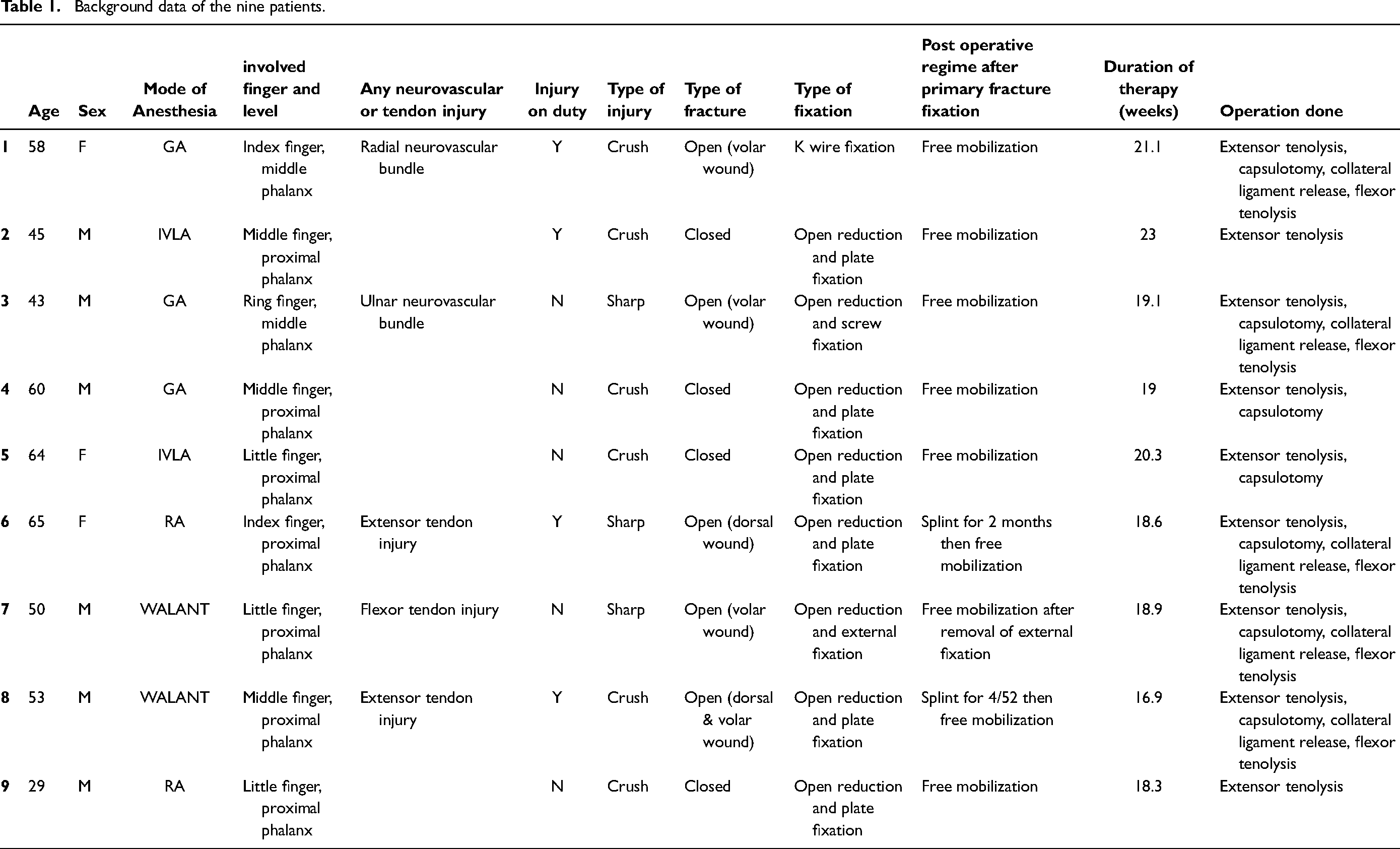
Patients who were admitted to our center between 2015 and 2019 for phalangeal fractures, with subsequent fracture fixation and tenolysis, and plateaued hand function were included in this study (Table 1).
All fractures had either open or close reduction withfixation done. The fractures healed with good union on radiograph. All included patients have completed physiotherapy and achieved the maximum range of motion. Patients were followed up at the hand clinic and the tenolysis decision was made by hand specialists. Decision of tenolysis is individualized for every patient. It is usually indicated when there is restricted active or/and passive flexion of interphalangeal joints, affecting the patients’ functional need. Other factors that affect the decision of tenolysis include radiography showing healed fracture and absence of finger joint arthritis, good skin and soft tissue condition and compliant patients. Decision of extensor and/or flexor tenolysis was decided preoperatively according to history of injury and active and passive range of motion. Demographic data such as age, gender, type of fracture, associated injury, and timing of tenolysis were retrieved. Patients with incomplete information, defaulted follow up or operation involving tendon reconstruction were excluded from this study.
Statistical analysis
The range of motion was evaluated and compared preoperatively, intraoperatively, and postoperatively. Complications such as tendon rupture during tenolysis and infection were reviewed. Paired t-test is used to compare the range of motion before and after tenolysis. Mann–Whitney U-test and Kruskal–Wallis test are used to analyze variables affecting tenolysis outcome. Pearson correlation coefficient is used to study the correlation of different variables. P value of <0.05 was considered to be statistically significant. Primary outcome was the range of motion of every finger joint.
Surgical technique
Tenolysis was performed under intravenous local anesthesia, regional anesthesia, Wide Awake Local Anesthesia No Tourniquet (WALANT), or general anesthesia. All patients received tenolysis and removal of implant. For patients with K wire fixation or external fixator applied, the implant was removed before arranging tenolysis.
Incision of extensor tenolysis was either through an old surgical scar or dorsal longitudinal incision. The techniques of extensor tenolysis were adopted as described by Creighton. 14 Extensor insertion was preserved, and extensors were released and mobilized from adhesive scarring laterally. If there was inadequate release after tenolysis due to joint contracture, capsulotomy would be performed with or without collateral ligament release. If there was still limited active flexion after extensor tenolysis and capsulotomy, it signified adhesion in flexor tendon system. Flexor tenolysis would be performed with Bruner incision. Flexor tendons were released and separated. If patient was unable to participate actively intraoperatively for finger flexion, an open traction tenolysis of the flexor digitorium superficialis and flexor digitorium profundus at volar wrist could be performed. However, this is preferred to be done in a separate operation. Meticulous hemostasis would be performed to avoid hematoma. Intraoperative range of motion would be assessed. Outpatient physiotherapy and occupational therapy were referred for continuation of rehabilitation care. Patients are required to follow the rehabilitation protocol and have at least 16 weeks of sessions until the progress reaches plateau.
Results
Between 2015 and 2019, 14 phalangeal fracture with fracture fixation and tenolysis procedures were performed at our center. Five cases were excluded because of insufficient data (three patients) or defaulted follow up (two patients). A total of nine patients, including six men and three women, were recruited in this retrospective study. Among them, four suffered from closed fractures and five suffered from open fractures. There were two intraarticular fractures and seven extraarticular fractures. All patients had fracture at either middle phalanx (two patients) or proximal phalanx (seven patients). Among the open fractures, three had tendon injury and other two had digital nerve injury. Three patients had fracture involving the little finger, three involving the middle finger, two involving the index finger and one involving the ring finger. No patient had multiple finger fractures.
The mean age of these nine patients was 51.9 years (range: 29 to 65). Forty four percent (4/9) of patients were manual workers. There was no delayed fracture. Six patients (all closed fracture cases and two open fracture cases with dorsal wound) had open reduction internal fixation by plate using extensor tendon splitting approach, the remaining three patients had either closed reduction with K wire fixation or open reduction internal fixation by screw or open reduction external fixation. Overall, three patients had operation done under general anesthesia, two under intravenous local anesthesia, two under regional anesthesia with brachial plexus block, and two under WALANT (wide awake local anesthesia no tourniquet) technique. All patients had extensor tenolysis and removal of implant done. Five patients also received flexor tenolysis at zone II. For patients with flexor tenolysis done, 4 of 5 had a volar laceration at the initial injury. Five patients underwent proximal interphalangeal joint or metacarpophalangeal joint capsulotomy.
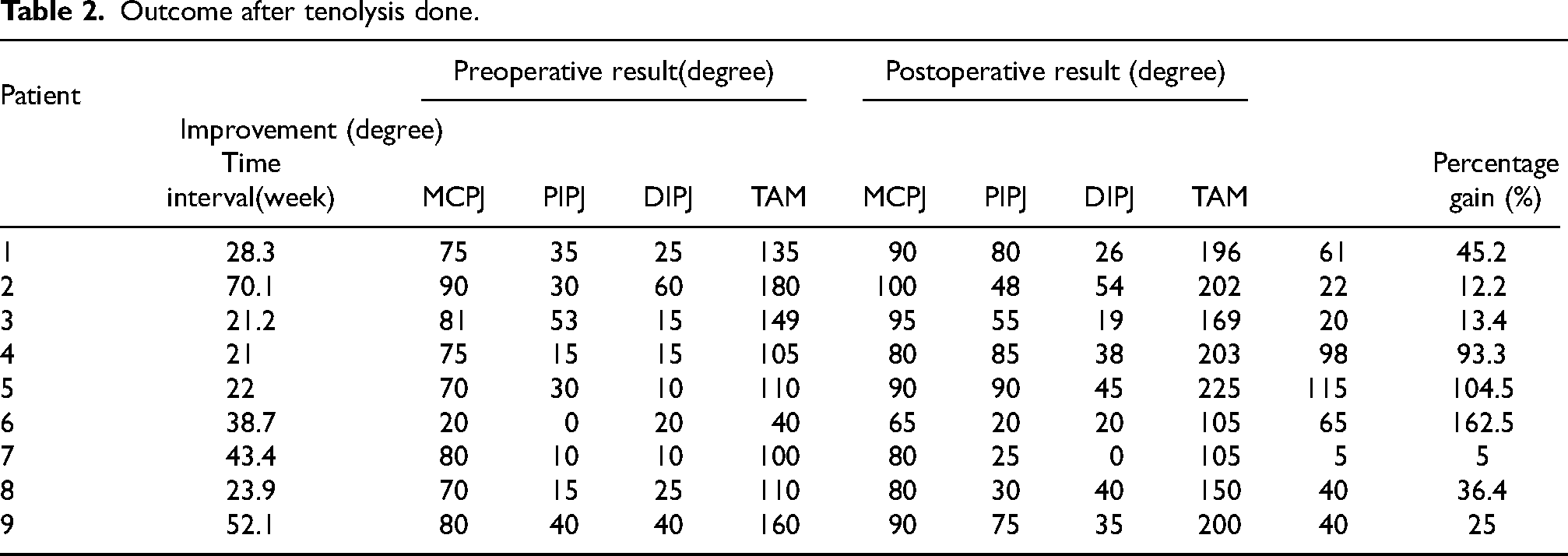
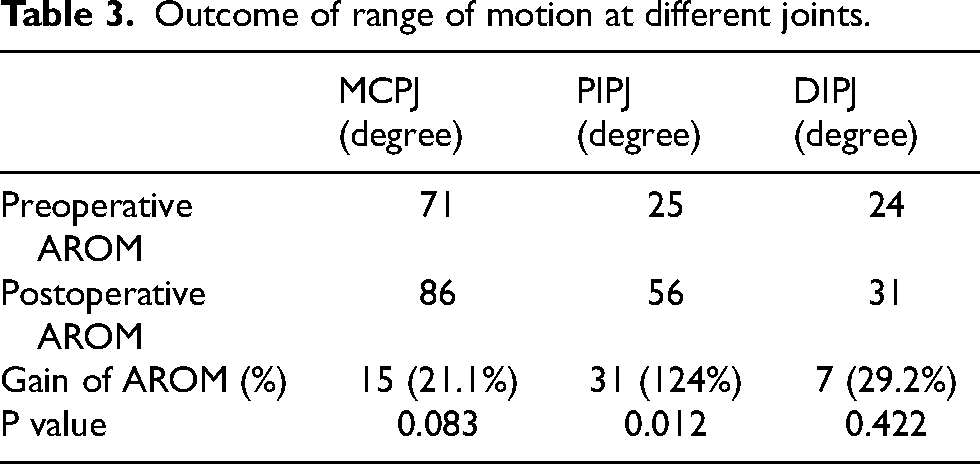
Patients had received rehabilitation after primary fracture fixation at a mean of 4.5 months. Tenolysis was performed at a mean of 8.2 months after hand fracture (Table 2). Patients were reviewed up to a mean of 6.9 months. All cases had extensor tenolysis done through dorsal incision (either through old surgical scar or longitudinal dorsal incision). The total active motion (TAM) improved from 121° preoperatively to 173° postoperatively (p = 0.02) with a gain of 52° (or a 43% improvement from preoperative motion). Significant improvement of motion was observed at proximal interphalangeal joints (p = 0.012), but not at metacarpophalangeal joints or distal interphalangeal joints (Table 3). There was no significant difference in the outcome of TAM in relation to the presence of tendon injury or neurovascular injury (p = 0.661 and p = 0.606, respectively). No significant difference in outcomes was observed between the timing of tenolysis and improvement in TAM (r = −0.325, p = 0.393). All patients’ motion improved after surgery.
Background data of the nine patients.
Outcome after tenolysis done.
Outcome of range of motion at different joints.
Postoperatively, all except one patient started immediate mobilization. There was one case of extensor digitorum communis rupture during tenolysis. The patient was given a resting splint postoperatively and the mobilization exercise was delayed.
Discussion
The study by Fetrow et al. showed 7% people had either worse result or tendon rupture after tenolysis. 10 Lutsky et al. noted 4 of 18 patients had loss of motion after tenolysis. 12 We found that our result is comparable to those reported from previous studies. There was no loss of motion after tenolysis in our study, even in the case with ruptured extensor digitorum comminus during operation. Although the patient was given a resting splint for immobilization, there was a good outcome eventually with 163% gain in TAM.
Our results showed a gain of TAM of 52° after tenolysis for finger stiffness after phalangeal fracture. This result compared favorably with a gain of TAM of 54° in Creighton study and 41° in Lutsky case series of tenolysis for finger stiffness after phalangeal fractures and metacarpal fractures, respectively.9,12 Of the 18 patients in the cohort study by Lutsky, 12 were phalangeal fractures. 12 There was 47° gain in TAM among 12 phalangeal fractures. In general, a smaller degree of preoperative TAM will have a higher percentage change in TAM [Graph 1]. The preoperative TAM value may serve as a reference to the surgeon whether tenolysis is worth performing.
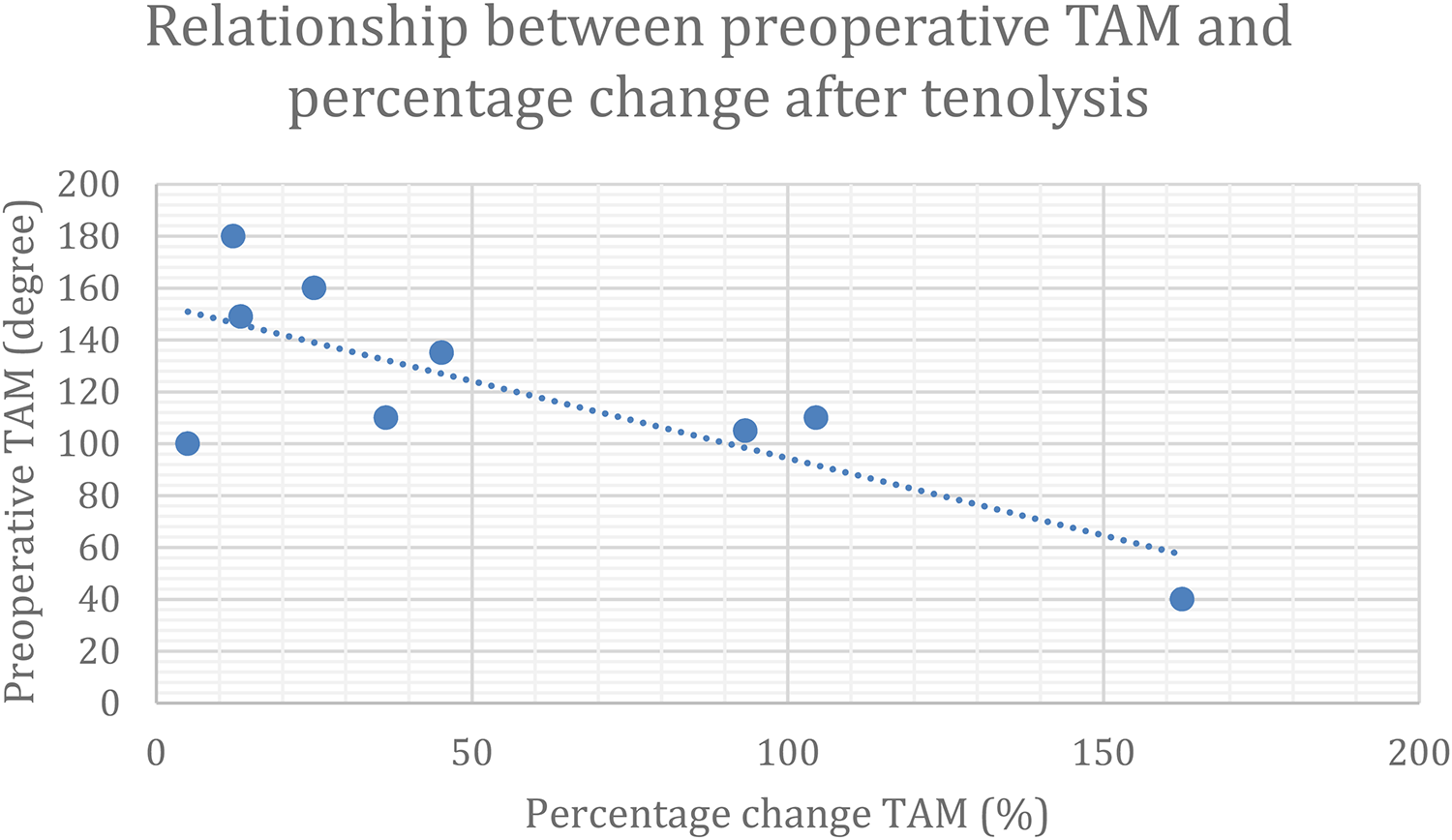
Relationship between preoperative Total active motion (TAM) and percentage change after tenolysis.
Another study by Guelmi et al. reported a gain of 34° (from 44° preoperatively to 78° postoperatively) at proximal interphalangeal joint (PIPJ) in 18 patients, 11 in which the outcome may improve the functional activity of patients.12,15 There was significant improvement in the proximal interphalangeal joint in our study. Since most fractures were located at the proximal phalanx, the difference in distal interphalangeal joints may not be significant.
Hume et al. reported functional flexion posture required 61° at metacarpophalangeal joint (MCPJ), 60° at PIPJ and 39° at the distal interphalangeal joint (DIPJ) to complete functional tasks. 15 A more recent paper on functional range of motion of finger by Bain et al. suggested functional arc of motion is greatest in PIPJ of 64° and it is mainly in the flexion part of the arc. The arc of functional range of motion of MCPJ and DIPJ is 52° and 54°, respectively. 16 In our study, functional arc/range of motion was achieved in 8 of 9, 0 of 9 and 2 of 9 patients (according to Hume et al. study) and 8 of 9, 0 of 9 and 1 of 9 patients (according to Bain et al. study) preoperatively in MCPJ, PIPJ and DIPJ respectively.15,16 Postoperatively, functional arc/range of motion was achieved in 9 of 9, 4 of 9, and 3 of 9 patients (according to Hume et al. study) and 9 of 9, 4 of 9, and 1 of 9 patients (according to Bain et al. study) in MCPJ, PIPJ, and DIPJ, respectively. The most significant improvement was observed in PIPJ.15,16
Surgical approach of fracture fixation should be carefully considered to reduce hand stiffness. Stable fixation and early painless mobilization may be obtained by plate fixation, tension band wiring, multiple lag screw fixation, or combinations. External fixation of finger may tether the extensor hood, impair the active motion of finger joints, and lead to hand stiffness. Our study also showed that patients with external fixation achieved the least percentage gain (5% gain in TAM) while those with plate fixation performed had the best result (mean 72.3% gain in TAM). Mid dorsal extensor splitting approach is a commonly used approach to fix the phalangeal fractures. A recent systematic review by Sivakumar et al. 17 reported that TAM was greater in the extensor sparing group compared to the extensor splitting group for proximal phalangeal fractures. In our study, all plate fixation used dorsal extensor splitting approach. Randomized controlled trial comparing different fracture fixation approaches is needed to provide more evidence on minimizing hand stiffness after phalangeal fracture fixation.
Studies have reported that capsulectomy can provide functional gain to hand stiffness. Gould and Nicholson 18 noted an average gain of 13° to 18° after MCPJ and PIPJ capsulectomy. Creighton and Steichen 9 suggested adding dorsal capsulotomy if passive flexion was limited despite extensor tenolysis. There are controversies in the correlation between the extent of structural release and gain of motion.12,18 We observed that the majority of patients (7 of 9) required additional structures released other than removal of implant and extensor tenolysis. When we compare the result of extensor tenolysis (n = 2) versus extensor tenolysis and capsulotomy (n = 2) versus extensor tenolysis, capsulotomy, collateral release, and flexor tenolysis (n = 5), we observed that more structural release did not result in a better percentage gain postoperatively (p = 0.119). Yet, comparing the correlation among them is difficult due to heterogeneity of the adhesion causes and surgical procedures to be performed.
Creighton et al. suggested that flexor tenolysis should be considered when there is limited active flexion after extensor tenolysis. 14 Distal flexor tenolysis is not recommended in the same setting due to digital swelling, pain, and conflicts in the treatment protocols that may hinder the flexion outcome postoperatively. Among the patients who had tenolysis done under general anesthesia, two of them also had flexor tenolysis done. Flexor tenolysis was decided using “traction check” by pulling on the flexors through a volar wrist incision and estimating the potential range of motion after flexor tenolysis. We believe the outcome may improve further if patients had tenolysis done under local anesthesia with better examination of discrepancy between active and passive flexion after extensor tenolysis and capsulotomy.
In cases of hand stiffness caused by tendon laceration, most authors recommended tenolysis at 3 to 6 months after initial injury.10,19 However, there is limited data on the preferable timing for tenolysis after hand fracture. We believe the exact timing will be similar to tendon injury. Certainly, fracture has to heal first before further aftercare procedures are contemplated. In our study, no correlation was found between the timing of tenolysis and the total active range motion. However, this finding could be just due to the small sample size.
Recurrence of adhesion is a major cause of failure after tenolysis. Immediate mobilization and careful surgical technique are the current practice to reduce the chance of adhesion formation.10,12,13 Different biological products have also been advocated to limit the adhesion formation. The use of hyaluronic acid can improve tendon gliding by acting as a tissue lubricator and prevent adhesion formation from its anti-inflammatory activity. Recent clinical trials proved that hyaluronic acid can result in significant increase in the total active and passive range of motion after flexor tendon repair compared to placebo groups in the long term.20,21 Although the use of this biological agent remains limited, it is speculated that hyaluronic acid can exert a positive effect on tenolysis as well.
It is crucial to tackle the causes of restricted digital motion in order to make tenolysis successful. Surgeons should understand the interaction between the tendon gliding and joint structures. Schneider et al. and Hunter et al. have advocated the use of local anesthesia to perform tenolysis.13,22 On table assessment and interaction with patients will be possible.22,23 In our study, local anesthesia will be the preferred option of anesthesia. If a patient is unfit for local anesthesia or a prolonged operation is required due to extensive scarring, brachial plexus block or general anesthesia will be performed. However, brachial plexus block will alter the true active finger motion due to the effect of muscle paralysis. Patient participation is even impossible in general anesthesia. Structures released in general anesthesia can only be predicted and decided preoperatively.
A newer type of local anesthesia, Wide Awake Local Anesthesia No Tourniquet (WALANT), has emerged with increasing popularity in hand surgery. The only medication required is an amino-amide anesthetic (e.g., lidocaine or Bupivacaine) with epinephrine. 24 It provides a bloodless field without the need of a tourniquet. Tourniquet related discomfort from intravenous local anesthesia has been a major concern when sedation is not used. However, this can be avoided in WALANT. 25 Injection of epinephrine into the hand region has once been discouraged due to the issue of digital artery ischemia. However, recent studies have proven it is a safe procedure.26,27 Depending on the dosage combination of the mixture, anesthesia time can be up to 2.5 h. 24 Decreased postoperative pain and higher patient satisfaction were also reported in WALANT patients compared to monitored anesthesia care or intravenous local anesthesia. 28 In our institution, WALANT has been used for hand surgery since 2018. Two of our cases also had tenolysis done under WALANT. They well tolerated the procedures without any complications. On average, 65.8% of intraoperative TAM was maintained at the last follow up. We expect more WALANT cases will be recruited in the future to study the patient satisfaction and the possible additional benefit on tenolysis compared to intravenous local anesthesia.
There are a few limitations in our study. First of all, the small sample size limited the power of our conclusion. Patients who were lost to follow up or physiotherapy were excluded from this study. It is possible that this group of patients might have worse result, leading to selection bias. Fortunately, only two patients did not come back for follow up after operation, owing to the thorough preoperative counselling on surgical indication, as well as the clear explanation of the importance of postoperative rehabilitation. Secondly, the type of fracture, the concomitant soft tissue or neurovascular injuries, and the procedures involved in tenolysis varies. In some patients, there was delayed tenolysis up to 16 months. The timing of tenolysis varies among surgeons. Tenolysis is usually not recommended for more than 1 year after the injury. 29 One patient in our study refused tenolysis initially. We should review the benefit of tenolysis in cases with prolonged presentation of finger stiffness. Another limitation is the short average follow up of 6 months only. The improvement may not reach plateau yet. Last but not least, more parameters can be used to document the outcome of tenolysis such as the distance between the fingertip and the distal palmar crease while making a fist, QuickDASH scores and patient subjective satisfaction.
In summary, tenolysis can provide an encouraging improvement of active motion for stiff finger after hand fractures. Tailor-made decisions should be made for every patient, depending on their functional need and soft tissue condition, with individualized surgical plan or conservative management. Further study is required to demonstrate any correlation between the extent of structure released and the gain of motion. Type of fracture fixation and surgical approach may also affect the outcome after tenolysis. Use of biological products may provide additional benefits. Recent results using WALANT technique showed satisfactory outcome without any complications. Our pilot result echoes the outcome of WALANT in the literature. Future prospective trial on WALANT technique may further consolidate its potential benefit.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.